Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Oncofertility.northwestern.edu
Chapter 2 Gonadotoxicity of Cancer Therapies in Pediatric and Reproductive-Age Males Jill P. Ginsberg Introduction
Recent epidemiological studies estimate that approximately 1 in every 1,300 young males in the United States is a childhood cancer survivor ] . Of this population, approximately 30% received gonadotoxic cancer treatments that resulted in perma-nent infertility ] . Therefore, approximately 1 in every 5,000 young males is at risk for infertility due to their pediatric cancer treatment. This is in large part because of the sensitivity of male germ cells to injury by cytotoxic drugs and radiation therapy (RT). Germ cells that produce spermatozoa are more sensitive to chemotherapy and radiation compared to Leydig cells that generate testosterone . Thus, a common late effect of cancer therapy for male patients is infertility rather than impaired pubertal development or impaired sexual function .
Anatomy of the Testis
The testis is composed of three principal cell types: germ cells that develop into sperm, Sertoli cells that support and nurture developing germ cells and are also the site of production of the glycoprotein hormone inhibin, and Leydig cells that are responsible for testosterone synthesis ] . The seminiferous tubules—the site of
J. P. Ginsberg , M.D. (*) Cancer Survivorship Program , Children’s Hospital of Philadelphia, Perelman School of Medicine at the University of Pennsylvania , Colket Translational Research Building, 3501 Civic Center Boulevard, Room 10307 , Philadelphia , PA 19104 e-mail: [email protected]
C. Gracia and T.K. Woodruff (eds.), Oncofertility Medical Practice: Clinical Issues and Implementation,DOI 10.1007/978-1-4419-9425-7_2, Springer Science+Business Media New York 2012
spermatogenesis—are surrounded by a basement membrane (tunica propria) and embedded in a connective tissue matrix containing interspersed Leydig cells, blood vessels, and lymphatics. Within the tubules, the seminiferous epithelium contains germ cells and Sertoli cells. Leydig cells lie near the basal compartment of the semi-niferous tubules, enabling them to deliver high concentrations of testosterone neces-sary for normal spermatogenesis and male secondary sexual characteristics .
Spermatogenesis takes place in the seminiferous epithelium inside the tubule. The
least differentiated germ cells, spermatogonia, divide to form spermatocytes that immediately undergo meiosis. The haploid cells (spermatids) that are formed develop into fl agellate motile spermatozoa. This process requires up to 74 days ] . Since spermatozoa are continuously produced in adult men, a constant supply of germ cell precursors is necessary. The newly formed spermatozoa are transported through the lumen of the seminiferous tubules into the epididymis where they are stored.
Effects of Chemotherapy
Early studies based on histological assessment of testicular tissue and measurement of basal follicle-stimulating hormone (FSH) levels from a small number of patient samples suggested that the immature testis was relatively resistant to chemotherapy ] . However, more recent studies have demonstrated that the prepubertal and puber-tal testes are highly vulnerable to cytotoxic agents used in cancer therapy . The extent and reversibility of cytotoxic damage in the testis generally depends on the agent and cumulative dose received, although signi fi cant variations between individuals have been observed (see Table 1.1 in of this volume for a com-prehensive list). The gonadotoxic effects of alkylating agents have been most exten-sively studied ] , and alkylators often used to treat pediatric cancers are highly gonadotoxic . Alkylating agents that are known to cause infertility include busulfan, cisplatin, cyclophosphamide, ifosfamide, and procarbazine . The total dose of a chemotherapeutic agent is the critical determinant of gonado-toxic damage, as a higher total dose will incur more damage to sperm-forming cells. Currently, the overwhelming majority of pediatric cancer patients receive multiple chemotherapeutic drugs as part of their therapeutic regimen. Unfortunately, this approach may cause infertility even at lower doses of individual alkylating agents because of the synergistic gonadotoxicity that occurs with delivery of multiple alky-lator compounds.
The alkylator cyclophosphamide, either alone or in combination with other
agents, is known to damage the germinal epithelium. A meta-analysis of 30 studies that examined gonadal function following various chemotherapy regimens noted that gonadal dysfunction correlated with total cumulative dose of cyclophosph-amide, with doses higher than 300 mg/kg associated with a greater than 80% risk of gonadal dysfunction . A study of men who had been treated for pediatric solid tumors reported permanent azoospermia in 90% of those who received cumulative cyclophosphamide doses greater than 7.5 g/m 2 ] . Other studies have similarly
2 Gonadotoxicity of Cancer Therapies in Pediatric and Reproductive-Age Males
found that 7.5–9 g/m 2 of cyclophosphamide is associated with a signi fi cant risk of testicular injury .
Although tumor cytotoxicity data indicate that 1.1 g/m 2 cyclophosphamide is
approximately equivalent to 3.8 g/m 2 ifosfamide ] , the relative gonadotoxic effect of ifosfamide is not well known. In a recent study, investigators assessed pubertal development and performed semen analysis in a series of males who were treated using sarcoma protocols that contained ifosfamide as the only potential gonadotoxic agent ] . Biochemical evaluation also included a measurement of gonadotropins and inhibin B. In this study, all 32 males progressed normally through puberty, and no gonadal dysfunction was seen at a total ifosfamide dose of less than 60 g/m 2 . In those with a dose greater than 60 g/m 2 , however, two-thirds of those who underwent semen analysis were subfertile, 31% had elevated FSH, and 50% showed decreased inhibin B, suggesting germ cell failure ] .
Treatment of patients with Hodgkin’s disease (HD) has historically included the
use of procarbazine, together with alkylators such as chorambucil, mechlorethamine, and cyclophosphamide. Many survivors of these treatment protocols are infertile [ . Patients treated with six or more courses of mechlorethamine, vincristine, pro-carbazine, and prednisone (MOPP) demonstrated permanent azoospermia attribut-able to the alkylating agents mechlorethamine and procarbazine. Hassel et al. studied testicular function after OPA/COMP (vincristine, prednisone, adriamycin/cyclophosphamide, vincristine, methotrexate, prednisone) chemotherapy without procarbazine in boys with HD. These patients showed no major testicular damage compared with boys who had received OPPA/COPP (which includes procarbazine), providing strong evidence that procarbazine is a potent gonadotoxic agent . A number of studies have reported permanent azoospermia in 99–100% of patients with HD who were treated with 6–8 courses of combination chemotherapy regi-mens such as COPP (cyclophosphamide, vincristine, procarbazine, and predniso-lone) . CHOP (cyclophosphamide, doxorubicin, vincristine, prednisolone) or CHOP-like regimens such as those used for non-Hodgkin’s lymphoma (NHL) are generally less gonadotoxic than those used for HD, presumably due to the absence of procarbazine ] . Efforts to reduce the risk of sterility after HD include the use of ABVD (adriamycin, bleomycin, vinblastine, dacarbazine), an effective com-bination that does not contain the alkylating agents chlorambucil or procarbazine [ ] , and other related regimens. In one study, Viviani and colleagues showed that while recovery of spermatogenesis after MOPP was rare, all patients who expe-rienced oligospermia after ABVD recovered completely by 18 months ] .
The gonadal toxicity of alkylating agents is clear when we contrast the above
outcomes to those of children with acute lymphoblastic leukemia (ALL). In general, testicular function is normal in boys after chemotherapy for ALL , and the clas-sic antimetabolites used in the treatment of childhood ALL are not associated with long-term gonadal toxicity. While both vincristine and corticosteroids can cause immediate inhibition of spermatogenesis, recovery of spermatogenesis occurs fol-lowing the cessation of these agents .
The use of cisplatin is also associated with male infertility, with doses above
600 mg/m 2 associated with signi fi cant impairment of spermatogenesis . Patients
treated with cisplatin-based chemotherapy for osteosarcoma and testicular cancer are at risk for azoospermia. Lampe et al. evaluated 170 patients treated for testicular cancer who had received therapy with either carboplatin-based chemotherapy or cisplatin . A median of 30 months after treatment, 32% of patients were azoo-spermic and 25% were oligospermic. The probability of recovery was found to be higher in men who received carboplatin-based rather than cisplatin-based therapy and in those treated with fewer than fi ve cycles of chemotherapy .
Leydig cells are much less vulnerable to damage from cancer therapy than germ
cells, likely due to their slow rate of turnover . Chemotherapy-induced Leydig cell failure resulting in androgen insuf fi ciency or requiring testosterone replace-ment therapy is rare. However, studies suggest that Leydig cell dysfunction may be observed following treatment with alkylator-based regimens. When Leydig cell dysfunction occurs prior to or during puberty, affected individuals will experience delayed and/or arrested pubertal maturation and lack of secondary sexual character-istics ] . If the insult follows completion of normal pubertal development, observed symptoms include loss of libido, erectile dysfunction, decreased bone density, and decreased muscle mass . Measurements of testosterone and gonadotropin con-centrations are therefore warranted following chemotherapy treatment. Males with a raised luteinizing hormone (LH) concentration in the presence of low testosterone levels should be considered for androgen replacement therapy.
Effects of Radiation
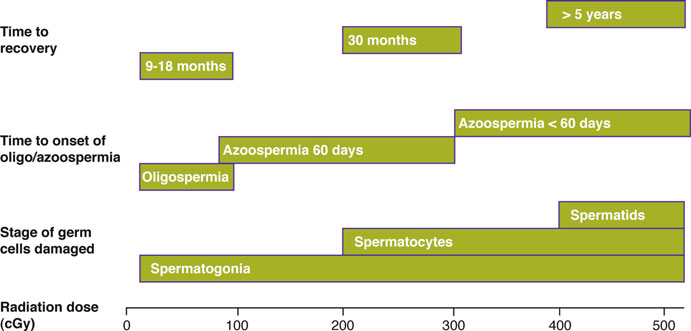
Data on human gonadal function following fractionated radiotherapy comes from patients with cancer who have received treatment in fi elds near the testes and where scatter has occurred or who have testicular cancer or ALL in which the testes are likely to contain disease and are irradiated directly. The testis is exquisitely radio-sensitive, with even very low doses causing signi fi cant impairment of function. illustrates the impairment of spermatogenesis following single-dose irra-diation and the time to onset and recovery from the resulting germ cell damage.
Ash summarized the data from several older studies that examined tes-
ticular function following radiation for patients who were treated for a range of cancers including HD, prostate cancer, and testicular cancer . Oligospermia occurred at doses as low as 10 cGy and azoospermia at 35 cGy, though this was generally reversible. Alternatively, exposure to 200–300 cGy resulted in azoo-spermia that did not reverse, even years after irradiation. These results have been supported by subsequent reports . Kinsella et al. studied 17 patients who received low-dose scattered irradiation for treatment of HD ] . In cases where the testicular dose was less than 20 cGy, radiation had no effect on FSH levels or sperm counts. Doses between 20 and 70 cGy did cause a temporary dose-dependent increase in FSH and reduction in sperm concentration, though normal values returned within 12–24 months.
There are also data on germ cell function after treatment for testicular cancer.
Hahn et al. examined gonadal function in 14 patients who were irradiated to the
2 Gonadotoxicity of Cancer Therapies in Pediatric and Reproductive-Age Males
Fig. 2.1 Effect of radiation dose on germ cell damage (Adapted from Howell et al. , with permission from Oxford University Press)
para-aortic and ipsilateral pelvic/inguinal lymphatics with a “hockey stick” fi eld following orchiectomy for seminoma ] . The scatter dose to the remaining testicle in these 14 patients ranged from 32 to 114 cGy (median 82 cGy). Ten patients, all of whom received ³ 70 cGy to the testes, developed azoospermia between 10 and 30 weeks following radiation. All patients except two recovered spermatogenesis, and the recovery time from azoospermia was dose dependent.
The previous data includes only patients who received incidental irradiation to
the testes; however, there are situations in which children receive direct irradiation of the testes. Sklar et al. examined testicular function in 60 long-term survivors of childhood ALL . All patients in the study had received identical chemotherapy; however, the RT fi elds varied signi fi cantly: (1) craniospinal radiation and 1,200 cGy to the abdomen and testes (n = 11), (2) craniospinal RT with 1,800 or 2,400 cGy (estimated gonadal dose 36–360 cGy; n = 23), or (3) cranial RT with 1,800 or 2,400 cGy (negligible testicular dose; n = 26). Based on measurements of serum FSH and testicular volume, which commenced at either 12 years of age or 7 years after diagnosis of ALL, gonadal function abnormalities occurred in 55%, 17%, and 0% of patients in groups 1, 2, and 3, respectively.
Leydig cells in the testes are more resistant to radiation than germ cells. In the
study by Kinsella and colleagues described previously ] , patients with HD who received 6–70 cGy of scatter dose to the testes showed no elevation in LH or decrease in testosterone. However, higher radiation doses to the testes result in more marked Leydig cell damage. Petersen et al. followed 48 patients who received 1,400–2,000 cGy of radiation for carcinoma in situ in the remaining testis following orchiectomy for testicular carcinoma . All patients had serial hormone analyses and at least one testicular biopsy more than a year after irradiation. Out of 42 men for whom data was available, 18 received hormonal supplementation therapy because of symptoms of androgen insuf fi ciency. Irradiation with 2,000 cGy led to a complete eradication of germ cells; however, Sertoli and Leydig cells were still present in the seminiferous tubules and in the intertubular space, respectively.
Data regarding Leydig cell function in young males following radiation comes
primarily from studies that followed boys who received direct testicular irradiation for ALL. In the analysis by Sklar et al. mentioned previously , only 1 out of 53 boys tested for gonadotropins had an increased LH level, and only 2 out of 50 patients tested had a reduced testosterone level. None of the boys had received greater than 1,200 cGy to the testes, however. By contrast, Blatt et al. followed seven boys who received 2,400 cGy testicular irradiation for relapsed ALL , and all boys had elevated FSH. Four of these boys had documented bilateral testicular disease, and three of these showed delayed sexual maturation with low testosterone levels. There are data that suggest that the prepubertal testis is more susceptible to Leydig cell injury than the adult testis . Based on a study by Shalet et al. in seven prepubertal boys with ALL who were irradiated with 2,400 cGy to the testes, six of the seven ultimately developed overt Leydig cell failure and required andro-gen replacement therapy .
There are also data on germ cell function following total body irradiation (TBI)
as part of transplant conditioning. Sarafoglou et al. followed 17 boys who had received cyclophosphamide and TBI (either 1,375 cGy or 1,500 cGy in 125 cGy tid fractionation) prior to puberty as part of a transplantation regimen for leukemia . Fourteen of 17 patients (82%) entered puberty spontaneously, and of these, 13 had normal testosterone levels. Of the three who did not enter puberty spontane-ously, one patient had received a 1,200 cGy testicular boost in addition to TBI, and the remaining had very low levels of FSH and LH consistent with a prepubertal state. In a similar study, Couto-Silva et al. followed 29 boys who received TBI for different malignancies in combination with a variety of chemotherapy regimens . TBI was given as a single 1,000 cGy fraction in 12 patients and in 200 cGy × 6 fractions (1,200 cGy) in 17 patients. At the last follow-up (average 10 years), 19/29 boys (66%) had tubular failure associated with elevated FSH, and 8 (28%) also had Leydig cell failure. There was no relationship between the age at the time of bone marrow transplant (BMT) and serum FSH, LH, or testosterone levels.
Sanders et al. reported the Seattle Marrow Transplant Team’s fi ndings of a high
incidence of pubertal developmental delay in boys undergoing transplantation for leukemia who received cyclophosphamide and TBI (900–1,000 cGy in a single fraction or 1,200–1,575 cGy in 200–225 cGy daily fractions over 6–7 days) . In the study, 31 boys were prepubertal at the time of transplantation (between the ages of 13 and 22), and 21 of these patients had delayed development of secondary sex-ual characteristics. Serum gonadotropins were obtained in 25 of the 31 boys; of these, LH was elevated in 10 boys, normal in 12, and at prepubertal levels in 3.
Assessment of Testicular Function
It is clear from the medical literature that the male reproductive tract is highly sus-ceptible to the toxic effects of chemotherapy and RT, which may damage the testes directly as well as disrupt the endocrine axis by altering Leydig cell function.
2 Gonadotoxicity of Cancer Therapies in Pediatric and Reproductive-Age Males
Assessment of the effects of chemotherapy or radiation therapy on testicular maturation and function in male cancer patients is an important part of care and involves pubertal staging, plasma hormone analysis, and semen analysis. Pubertal staging provides clinical information about the two testicular functions: germ cell production and steroidogenesis. The development of normal secondary sexual char-acteristics would suggest intact Leydig cell function with normal steroidogenesis, while testicular volume is an important indicator of spermatogenesis. Testicular vol-ume of less than 12 mL, determined using a Prader orchidometer, is strongly sug-gestive of impaired spermatogenesis.
Hormone analysis involves measurement of plasma FSH, LH, and sex steroids;
however, in prepubertal children, this is an unreliable predictor of gonadal damage because the hypothalamic-pituitary-testicular axis is still quiescent. In postpubertal boys, elevated LH and diminished testosterone levels would indicate Leydig cell dysfunction, whereas elevated FSH and diminished inhibin B would suggest germ cell failure.
The gold standard for assessing a male patient’s fertility status after cancer ther-
apy is semen analysis ] . It is important that semen samples are properly col-lected, which usually involves the patient abstaining from sexual intercourse for 3–5 days and then collecting the specimen by masturbation. Sperm count and qual-ity can provide useful information about the likelihood of natural fertility or whether assisted reproduction may be required.
Conclusions
Cancer survivors are at risk for long-term treatment-related gonadal failure and infertility. It is essential for oncologists to consider the potential impacts of treat-ment on every patient’s fertility. Counseling and treatment should begin prior to initiating chemotherapy or radiation therapy when a window of opportunity may exist to preserve future reproductive potential ] and discussed in more detail
Acknowledgments This work was supported by the Oncofertility Consortium NIH/NICHD 5UL1DE019587. References
1. Hewitt M, et al. Childhood cancer survivorship: improving care and quality of life. Washington,
2. Green DM, et al. Fertility of male survivors of childhood cancer: a report from the Childhood
Cancer Survivor Study. J Clin Oncol. 2010;28:332–9.
3. Shalet SM, et al. Vulnerability of the human Leydig cell to radiation damage is dependent
upon age. J Endocrinol. 1989;120:161–5.
4. Meistrich ML. Male gonadal toxicity. Pediatr Blood Cancer. 2009;53:261–6. 5. Sklar C. Reproductive physiology and treatment-related loss of sex hormone production. Med
6. Morris ID. The testis: endocrine function. In: Hiller SG, Kitchener HC, Neilson JP, editors.
Scienti fi c essentials of reproductive medicine. London: Saunders; 1996.
7. Smith KD, Rodgriguez-Rigau LJ. Laboratory evaluation of testicular function. In: Degroot LJ,
editor. Endocrinology. Philadelphia: Saunders; 1989.
8. Sherins RJ, Olweny CL, Ziegler JL. Gynaecomastia and gonadal dysfunction in adolescent
boys treated with combination chemotherapy for Hodgkin’s disease. N Engl J Med. 1978;299:12–6.
9. Hobbie WL, et al. Fertility in males treated for Hodgkins disease with COPP/ABV hybrid.
10. Howell S, Shalet S. Gonadal damage from chemotherapy and radiotherapy. Endocrinol Metab
11. Mackie EJ, Radford M, Shalet SM. Gonadal function following chemotherapy for childhood
Hodgkin’s disease. Med Pediatr Oncol. 1996;27:74–8.
12. Papadakis V, et al. Gonadal function in young patients successfully treated for Hodgkin dis-
ease. Med Pediatr Oncol. 1999;32:366–72.
13. Ahmed SR, et al. Primary gonadal damage following treatment of brain tumors in childhood.
14. da Cunha MF, Meistrich ML, Fuller LM. Recovery of spermatogenesis after treatment for
Hodgkin’s disease: limiting dose of MOPP chemotherapy. J Clin Oncol. 1984;2:571–7.
15. Longhi A, et al. Fertility in male patients treated with neoadjuvant chemotherapy for osteosar-
coma. J Pediatr Hematol Oncol. 2003;25:292–6.
16. Rivkees SA, Crawford JD. The relationship of gonadal activity and chemotherapy-induced
gonadal damage. JAMA. 1988;259:2123–5.
17. Thomson AB, et al. Semen quality and spermatozoal DNA integrity in survivors of childhood
cancer: a case-control study. Lancet. 2002;360:361–7.
18. Aubier F, et al. Male gonadal function after chemotherapy for solid tumors in childhood. J Clin
19. Kenney LB, et al. High risk of infertility and long term gonadal damage in males treated with
high dose cyclophosphamide for sarcoma during childhood. Cancer. 2001;91:613–21.
20. Colvin M. The comparative pharmacology of cyclophosphamide and ifosfamide. Semin
21. Williams D, Crofton PM, Levitt G. Does ifosfamide affect gonadal function? Pediatr Blood
22. Viviani S, et al. Gonadal toxicity after combination chemotherapy for Hodgkin’s disease.
Comparative results of MOPP vs ABVD. Eur J Cancer Clin Oncol. 1985;21:601–5.
23. Hassel JU, et al. Testicular function after OPA/COMP chemotherapy without procarbazine in
boys with Hodgkin’s disease. Results in 25 patients of the DAL-HD-85 study. Klin Padiatr. 1991;203:268–72.
24. Charak BS, et al. Testicular dysfunction after cyclophosphamide-vincristine-procarbazine-
prednisolone chemotherapy for advanced Hodgkin’s disease. A long-term follow-up study. Cancer. 1990;65:1903–6.
25. Radford JA, et al. Male fertility after VAPEC-B chemotherapy for Hodgkin’s disease and non-
Hodgkin’s lymphoma. Br J Cancer. 1994;69:379–81.
26. Muller U, Stahel RA. Gonadal function after MACOP-B or VACOP-B with or without dose
intensi fi cation and ABMT in young patients with aggressive non-Hodgkin’s lymphoma. Ann Oncol. 1993;4:399–402.
27. Kulkarni SS, et al. Gonadal function following ABVD therapy for Hodgkin’s disease. Am J
28. Wallace WH, et al. Male fertility in long-term survivors of childhood acute lymphoblastic
leukaemia. Int J Androl. 1991;14:312–9.
2 Gonadotoxicity of Cancer Therapies in Pediatric and Reproductive-Age Males
29. Kreuser ED, et al. Reproductive and endocrine gonadal functions in adults following
multidrug chemotherapy for acute lymphoblastic or undifferentiated leukemia. J Clin Oncol. 1988;6:588–95.
30. Meistrich M, et al. Recovery of sperm production after chemotherapy for osteosarcoma.
31. Lampe H, et al. Fertility after chemotherapy for testicular germ cell cancers. J Clin Oncol.
32. Speiser B, Rubin P, Casarett G. Aspermia following lower truncal irradiation in Hodgkin’s
33. Hahn EW, Feingold SM, Nisce L. Aspermia and recovery of spermatogenesis in cancer patients
following incidental gonadal irradiation during treatment: a progress report. Radiology. 1976;119:223–5.
34. Sandeman TF. The effects of x irradiation on male human fertility. Br J Radiol.
35. Ash P. The in fl uence of radiation on fertility in man. Br J Radiol. 1980;53:271–8. 36. Kinsella TJ, et al. Long-term follow-up of testicular function following radiation therapy for
early-stage Hodgkin’s disease. J Clin Oncol. 1989;7:718–24.
37. Shapiro E, et al. Effects of fractionated irradiation of endocrine aspects of testicular function.
38. Hahn EW, et al. Recovery from aspermia induced by low-dose radiation in seminoma patients.
39. Sklar CA, et al. Effects of radiation on testicular function in long-term survivors of childhood
acute lymphoblastic leukemia: a report from the Children Cancer Study Group. J Clin Oncol. 1990;8:1981–7.
40. Petersen PM, et al. Effect of graded testicular doses of radiotherapy in patients treated for
carcinoma-in-situ in the testis. J Clin Oncol. 2002;20:1537–43.
41. Blatt J, et al. Leydig cell function in boys following treatment for testicular relapse of acute
lymphoblastic leukemia. J Clin Oncol. 1985;3:1227–31.
42. Shalet SM, et al. Leydig cell damage after testicular irradiation for lymphoblastic leukaemia.
43. Leiper AD, Grant DB, Chessells JM. Gonadal function after testicular radiation for acute lym-
phoblastic leukaemia. Arch Dis Child. 1986;61:53–6.
44. Sarafoglou K, et al. Gonadal function after bone marrow transplantation for acute leukemia
during childhood. J Pediatr. 1997;130:210–6.
45. Couto-Silva AC, et al. Factors affecting gonadal function after bone marrow transplantation
during childhood. Bone Marrow Transpl. 2001;28:67–75.
46. Sanders JE, et al. Growth and development following marrow transplantation for leukemia.
47. van Casteren NJ, et al. Effect of childhood cancer treatment on fertility markers in adult male
long-term survivors. Pediatr Blood Cancer. 2009;52:108–12.
48. Redig AJ, et al. Incorporating fertility preservation into the care of young oncology patients.
49. Woodruff TK. The Oncofertility Consortium–addressing fertility in young people with cancer.
50. Howell SJ, Shalet SM. Spermatogenesis after cancer treatment: damage and recovery. J Natl
BPS HEALTH PLAN & WELLNESS HELPING YOU Did you know there are many resources to help you quit smoking? Effective March 1, 2012, if you participate in the BPS Health Plan, administered by CIGNA, you now have smoking cessation medications and aids as part of your pharmacy benefits. • Zyban - Bupropion hcl, marketed as name brand Zyban, is an anti-depressant drug that also wo
For Home Office Associates and Investment ProfessionalsInvestors should be encouraged to type in the entire URL to view the correct website and avoid confusion. Please note: www.edocumentsuite.com is a Remind clients of the correct URL and encourage them to bookmark it different website provided by Pershing LLC; however, it is for investment or save it as a “favorite” for easy access and
 2 Gonadotoxicity of Cancer Therapies in Pediatric and Reproductive-Age Males
Fig. 2.1 Effect of radiation dose on germ cell damage (Adapted from Howell et al. , with
2 Gonadotoxicity of Cancer Therapies in Pediatric and Reproductive-Age Males
Fig. 2.1 Effect of radiation dose on germ cell damage (Adapted from Howell et al. , with