Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Executive function in tourette's syndrome and obsessive–compulsive disorder
Psychological Medicine, 2005, 35, 571–582.
Executive function in Tourette’s syndrome
L A U R A H. W A T K I N S 1, B A R B A R A J. S A H A K I A N 2*, M A R Y M. R O B E R T S O N 4,
D A V I D M. V E A L E 4, R O B E R T D. R O G E R S 3,5, K A T H R Y N M. P I C K A R D 1 ,
M I C H A E L R. F. A I T K E N 3 A N D T R E V O R W. R O B B I N S 3
1 MRC Cambridge Centre for Brain Repair, Departments of 2 Psychiatry and 3 Experimental Psychology,
University of Cambridge, Cambridge, UK ; 4 Department of Psychiatry and Behavioural Sciences, Royal Free
and University College School of Medicine, University of London ; UK ; 5 Department of Psychiatry,
Background. Cognitive performance was compared in the genetically and neurobiologically relateddisorders of Tourette’s syndrome (TS) and obsessive–compulsive disorder (OCD), in three domainsof executive function : planning, decision-making and inhibitory response control.
Method. Twenty TS patients, twenty OCD patients and a group of age- and IQ-matched normalcontrols completed psychometric and computerized cognitive tests and psychiatric rating scales. The cognitive tests were well-characterized in terms of their sensitivity to other fronto-striatal dis-orders, and included pattern and spatial recognition memory, attentional set-shifting, and a Go/No-go set-shifting task, planning, and decision-making.
Results. Compared to controls, OCD patients showed selective deficits in pattern recognitionmemory and slower responding in both pattern and spatial recognition, impaired extra-dimensionalshifting on the set-shifting test and impaired reversal of response set on the Go/No-go test. Incontrast, TS patients were impaired in spatial recognition memory, extra-dimensional set-shifting,and decision-making. Neither group was impaired in planning. Direct comparisons between the TSand OCD groups revealed significantly different greater deficits for recognition memory latency andGo/No-go reversal for the OCD group, and quality of decision-making for the TS group.
Conclusions. TS and OCD show both differences (recognition memory, decision-making) and simi-larities (set-shifting) in selective profiles of cognitive function. Specific set-shifting deficits in theOCD group contrasted with their intact performance on other tests of executive function, such asplanning and decision-making, and suggested only limited involvement of frontal lobe dysfunction,possibly consistent with OCD symptomatology.
usually develop in adolescence (Freeman, 1992).
Tourette’s syndrome (TS) is a neurodevelop-
Despite the quite different clinical profiles of
mental condition characterized by motor and
these two disorders, there is good evidence for
vocal tics that typically develop at 5–7 years
genetic linkage between them (State et al. 2003).
of age (APA, 1994 ; Robertson, 1994, 2000).
TS and half of OCD cases are thought to be
Obsessive–compulsive disorder (OCD) sufferers
inherited in autosomal dominant fashion, with
a single (as yet unidentified) locus for trans-mission, but with incomplete penetrance and
* Address for correspondence : Professor Barbara Sahakian,
variable phenotype (Pauls & Leckman, 1986 ;
Department of Psychiatry (Box 189), University of Cambridge,
Eapen et al. 1993 ; Pauls et al. 1995 ; Leckman
Addenbrooke’s Hospital, Cambridge CB2 2QQ, UK.
Both disorders are thought to have a neuro-
biological basis in the frontal cortex and basal
test results [values are mean (standard deviation)]
ganglia. Changes in regional cerebral blood flow(rCBF) and metabolism have been observed in
TS patients, particularly in the ventral striatum,
lateral orbito-frontal cortex (OFC) and the an-
terior cingulate gyrus (ACG) (Braun et al. 1993 ;
for review see Weeks et al. 1996 ; Leckman et al.
1997). Dopaminergic abnormalities observed
in TS (Devinsky, 1983 ; Leckman et al. 1997)
suggest an imbalance in the interactions of the
striatum. Similarly, many studies have found
abnormal rCBF or metabolism in OCD : with
the OFC, ACG and caudate nucleus typically
showing overactivity (for review, see Saxena
Disruption to fronto-striatal circuitry leads
to impairment in tasks requiring executive
Upper panel : PVIQ, predicted pre-morbid verbal IQ ; MMSE,
Mini Mental-State Examination ; BDI, Beck Depression Inventory.
Lower panel : Arithmetic, arithmetic subtest of Wechsler Adult
decision-making, i.e. tasks requiring higher level
Intelligence Scale ; Pattern, pattern recognition memory test ; Spatial,
cognition and optimization of complex cogni-
spatial recognition memory test ; RT, correct response latency ; N.S.,not significant ; Statistic, statistical difference.
tive performance (Tranel et al. 1994 ; Robbins,1996). Thus, whilst spatial working memory andplanning tasks strongly involve dorsolateral
issues. First, it provides a direct comparison
prefrontal cortex (DLPFC) circuitry (Alexander
between the two disorders, to test the hypothesis
et al. 1986 ; see Robbins, 1996, for review ; Baker
that a common genetic basis and similar neuro-
et al. 1996 ; Owen et al. 1996 ; Bechara et al.
biological background would lead to similar
1998), decision-making between options with
cognitive deficits. Second, we tested the hypoth-
variable degrees of rewarding and punishing
esis that the cognitive deficits seen in these two
feedback relies on circuitry of the OFC (Bechara
disorders would be more similar to those seen
et al. 1998 ; Rahman et al. 1999 ; Rogers et al.
in other disorders that disrupt the OFC circuitry
1999, 2000). Go/No-go and reversal paradigms
to a greater extent than the DLPFC circuitry
have also long been known to be sensitive to
(e.g. mild frontal-variant fronto-temporal de-
frontal dysfunction, particularly in the OFC
mentia) than to conditions that preferentially
region (Iversen & Mishkin, 1970 ; Butters et al.
disrupt the DLPFC rather than OFC circuitry
1973 ; Drewe, 1975 ; Petrides, 1986 ; Rolls et al.
(e.g. mild Huntington’s disease, see Lawrence &
1994 ; Godefroy et al. 1996 ; Dias et al. 1996)
and provide measures of inhibitory controlmechanisms that may well be disturbed in such
Despite its proposed fronto-striatal neuro-
pathology, studies of complex task performance
Permission for this study was obtained from the
in TS are sparse and findings in OCD have
Local Research Ethics Committee and all sub-
proved inconsistent. This study, therefore, com-
jects gave written informed consent. The patient
pared performance in the domains of atten-
tional control, planning and decision-making in
patients and 20 age- and IQ-matched control
patients with TS and OCD using neuropsycho-
subjects (Table 1). TS patients were diagnosed
logical tools that have been well-characterized
and recruited by MMR from the out-patient
in terms of their sensitivity to other fronto-
clinic at the National Hospital for Neurology
striatal disorders. This is, thus, perhaps the
first detailed neuropsychological comparison of
made on the basis of interview and completion
these groups. The study addresses two main
of the National Hospital Interview Schedule
Cognition in Tourette’s syndrome and OCD
(Robertson & Eapen, 1996). OCD patients were
Ten patients were unmedicated, eight were
Priory Hospital or an OCD support group.
taking SSRIs (five taking paroxetine, two taking
Subjects who scored below 24 on the Mini-
fluoxetine and one taking sertraline), one was
taking a tricyclic antidepressant (clomipramine)
excluded (Folstein et al. 1975), as were those
and one was taking both a monoamine oxidase
with a history of neurological or psychiatric
inhibitor (moclobemide) and an antipsychotic
conditions other than those under study [except
(trifluoperazine). The mean score on the Yale–
depression and attention deficit hyperactivity
Brown Obsessive–Compulsive Scale (YBOCS ;
disorder (ADHD)]. Twenty control subjects
Goodman et al. 1989) was 19.3 (S.D.=14.3).
were recruited by advertisement in Cambridgeand chosen to match the patient groupsaccording to age, pre-morbid IQ and gender
ratio. Severity of depression was assessed using
The background psychometric tests were as
the Beck Depression Inventory (BDI ; Beck et al.
follows : MMSE, National Adult Reading Test
1961) and severity of ADHD in TS patients was
[NART ; Nelson, 1982, to provide an estimate
assessed using the Attention Deficit Scale for
of pre-morbid verbal IQ (PVIQ)], letter fluency
Adults (ADSA ; Triolo & Murphy, 1996).
(Benton, 1968), semantic fluency and finallythe arithmetic subtest from the Wechsler Adult
Intelligence Scale (WAIS ; Wechsler, 1981). The
Six patients were unmedicated, 10 were taking
fluency and arithmetic tests were included as
a single medication and the remaining four were
examples of ‘ standard ’ tests of executive func-
taking more than one medication. Antipsy-
tion, the arithmetic test assessing working-
chotic medications were the most frequent : four
patients were taking sulpiride, six were taking
haloperidol, three were taking pimozide, two
portable microcomputer fitted with a Datalux
were taking risperidone and one was taking
touch-sensitive screen, which was positioned
clonidine. One patient was taking an anti-
approximately 0.5 m from the subject. Three
muscarinic drug (benzoptropine), three were
taking a selective serotonergic reuptake inhibi-
tor (SSRI) (fluoxetine) and one was taking a
benzodiazepine (lormetazepam). The mean Yale
Global Tic Severity Scale (YGTSS ; Leckman
et al. 1989) was 43.5 [standard deviation (S.D.)=
19.3] out of 100 ; this scale assesses motor and
vocal tics and their impact on daily activities.
puterized tests was counterbalanced.
After exclusion of patients with distinct co-morbid OCD by the clinician, all remaining
candidates were pre-screened with the Leyton
This test of discrimination learning assesses
Obsessional Inventory (LOI ; Cooper, 1970 ;
the ability to selectively attend to and set-shift
Snowdon, 1980) ; those who scored outside the
normal range were not tested. The mean LOI
dimensions (Downes et al. 1989). Measures were
score of the 20 TS patients included in the study
number of subjects passing each stage, errors
was 11.1 (S.D.=6.1), which is comparable to
and latency at the intra-dimensional (ID) and
the means obtained by Cooper (1970) of 8.7
(S.D.=5.6) for male controls (n=40) and 11.4(S.D.=6.7) for female controls (n=60). TSpatients scored a mean of 153.6 (
One-touch Tower of London (one-touch TOL)
the ADSA, which is within 1 S.D. of the norma-
This is a spatial planning test, involving plan-
tive mean of 141. Three patients scored greater
ning a sequence of moves to achieve a goal
than 2 S.D. from the normative mean, indicating
arrangement of coloured balls without moving
the balls (Owen et al. 1995). Measures were the
proportion of perfect solutions and latency to
age, MMSE score or predicted PVIQ [largest
F(2, 57)=1.54, p=0.22], although the groupsdiffered in mean (square-root-transformed) BDI
scores F(2, 55)=24.75] TS patients had higher
This test of decision-making and risk-taking
BDI scores than did the OCD or control groups
has previously been described by Rogers et al.
[smaller t(55)=5.03], who did not differ signifi-
(1999). Main measures were the latency to make
a decision, the proportion of decisions with the
As the patient groups were not completely
most likely outcome and the mean percentage
matched for age and sex ratio, care was taken
to ensure this did not confound interpretation. All subsequent ANOVAs were conducted both
with gender and age as predictors (fixed factor,
This test examines the ability to attend and
and covariate respectively). If these factors had
respond to relevant targets while inhibiting
no significant effects (Ff1.0), they were dis-
responses to distractors (McLean et al. 2004).
carded from the model ; thus, hypotheses on the
Measures were response, latencies, correct target
group factor are tested on the observed means
presses or ‘ hits ’, misses and false-positive errors.
only. Otherwise, both full and restricted models
Switch blocks (blocks on which the response
were analysed (observed and estimated marginal
contingencies are reversed from the previous
means), and the more conservative of the two
block) can be compared to non-switch blocks.
p values obtained was used for each hypothesistest on the group factor.
Data were analysed using SPSS version 11.0.1
(SPSS Inc., 2001). Comparisons of the means of
Results of the background neuropsychological
the three groups were via analysis of variance
tests are shown in the lower rows of Table 1. The
(ANOVA). Standard transformations of each
three groups did not differ on WAIS arithmetic,
subject’s mean score (Howell, 1997) were used
category fluency or letter fluency (F<1), nor on
to increase homogeneity of variance when this
response latency in the motor screening task
assumption was untenable (p<0.10, Levene’s
[F(2, 53)=2.40, p=0.10]. Significant main effects
of group were observed on both (arcsine-trans-
Significant main effects were investigated by
formed) accuracy and (logarithmic-transformed)
Fisher’s LSD test (protected t procedure for
latencies for the spatial and pattern recognition
three means), to give a strict control of maxi-
memory tasks [smallest F(2, 53)=3.43]. The
mum family-wise error rate, and a significance
OCD patients were slower than the other groups
level of 0.05 is used throughout. Where par-
to respond in both tasks [smaller t(53)=2.12];
ametric analyses were unsuitable, data were
response latencies were similar for TS and
analysed using the likelihood ratio method
controls (t<1). The two patient groups did not
(Kullback, 1968 ; Robbins, 1977) or Mann–
differ in accuracy of performance on either
task [larger t(53)=1.33, p=0.19] ; OCD patientswere less accurate than controls at the patternrecognition task, and TS patients were less ac-
curate than controls on both tasks [smaller
For five subjects, one of the tests was not com-
pleted successfully, and these data are missingfrom the analyses : BDI (two patients in the
OCD group) ; Go/No-go (one OCD) ; decision-
making task (one TS) ; TOL (one TS).
For purposes of analysis, subjects were scoredas to whether they successfully completed all
phases, or whether they failed before or after
One-way ANOVAs revealed no significant dif-
starting the ED shift phase. Likelihood-ratio
ferences between the three groups in terms of
analyses confirmed that a higher proportion of
Cognition in Tourette’s syndrome and OCD
response latencies on these two key dimen-
sional shift stages is possible by contrasting
model as a repeated-measures factor. However,estimates of mean population differences in
performance will be slightly conservative, as the
worst performing subjects in the patient groupsdid not contribute to these stages.
The groups differed in overall error rates
the ED shift phase [F(1, 53)=45.95], and there
was a significant interaction between these two
factors [F(2, 53)=4.21]. Separate analysis of thetwo stages confirmed the pattern seen in pass/
fail data. Whilst there were no group differences
in errors at the ID shift stage [F<1], there was asignificant effect of group upon error rates at
the ED shift stage [F(2, 55)=4.73)], with both
patient groups making more errors than controls
[smaller t(53)=2.24]. The two patient groups
did not differ in ED shift error rates (t<1).
Response latencies (logarithm-transformed)
were similar for all groups, and stages, with no
interaction [largest F(1, 49)=1.68, p=0.20].
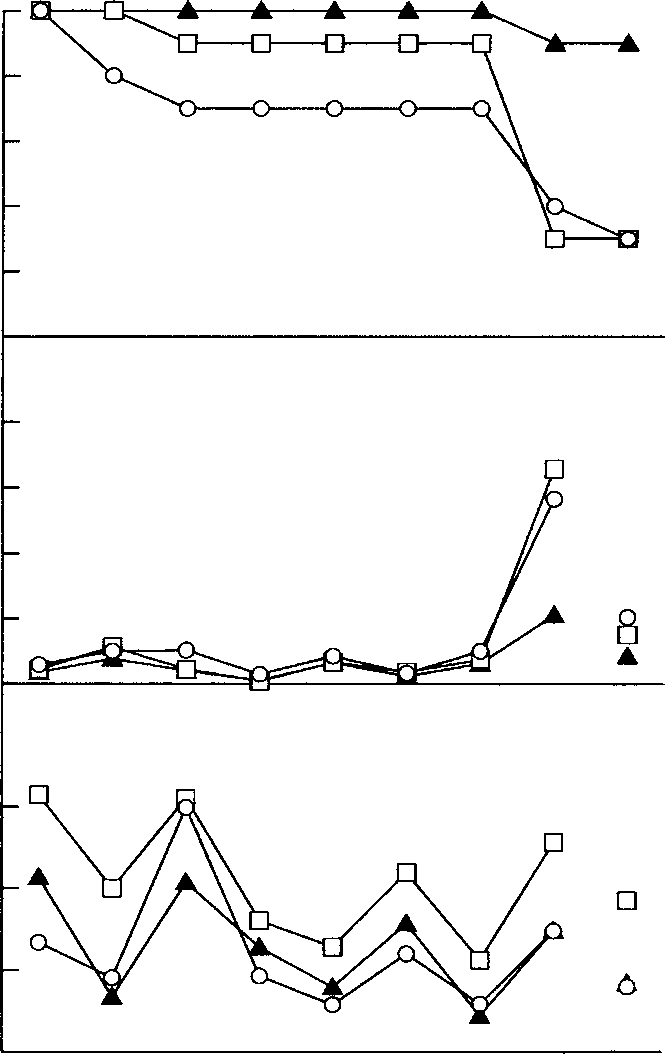
Attentional set-shifting test. –#–, TS ; –%–, OCD ; –m–,
The results of this test are shown in Table 2.
control. (a) Percentage of subjects passing each stage, shown as a
Separate ANOVAs were performed, contrast-
cumulative attrition curve. OCD patients and controls performedsimilarly up to the intra-dimensional reversal (IDR) stage, but sig-
ing (arcsine-transformed) proportion of trials
nificantly more OCD patients failed at the extra-dimensional shift
correct first attempt, and (logarithmic-trans-
(EDS) stage than controls. (b) Mean errors at intra-dimensional shift(IDS) and EDS stages of the attentional set-shifting test. Data are
formed) mean latency to first response for the
included for all subjects who attempted both stages, regardless of
three groups, with trial difficulty as a within-
outcome on the EDS stage. Both TS patients and OCD patients
subject factor. There was a main effect of diffi-
made disproportionately more errors at the EDS stage comparedwith the matched control group. Error bar=1 standard error of the
culty on both measures [smaller F (4, 208)=
mean (S.E.M.). (c) Mean correct response latencies. There were no
31.66], but they did not interact with group
significant differences, although the OCD patients tended to be slow.
reversal ; CDr, superimposed compound discrimination/reversal ;
groups to take longer and make fewer correct
IDSr, intra-dimensional shift/reversal ; EDSr, extra-dimensional
first responses were non-significant [larger
shift/reversal. Note that for (b) and (c) performance at the EDris disconnected from the EDS stage, as a number of patients failed
at the EDS, and therefore did not attempt the EDr.
patients than controls failed to complete all
The proportion of trials on which subjects chose
stages [x2(2)=7.51], as shown in Fig. 1a. The
the most likely outcome were 95.9, 98.1 and
tendency of TS patients to be more likely than
98.6 % for the TS, OCD and control groups
OCD patients to fail prior to the EDS phase was
respectively. With half or more of the subjects
non-significant [x2(1)=1.99, p=0.27].
in each group scoring 100 %, these data cannot
Error rates and response latencies for those
be made suitable for parametric analyses.
subjects who attempted the ED shift stage of the
task are shown in Fig. 1(b, c). Because all sub-
groups differed [x2(2)=6.65], Mann–Whitney
jects who undertook the ID shift stage also
tests confirming that OCD patients and controls
undertook the ED shift stage (20 controls, 19
chose similarly well (ZU=0.53) and that TS
OCD, 17 TS), comparison of group errors and
patients chose the more likely outcome less
Performance on psychological tests (values are untransformed cell means)
% Bet, mean percentage of points staked on trials on which the more likely outcome was chosen. % First, mean percentage of problems on
which the correct response was chosen first. Analysis revealed no significant differences between groups on these measures.
frequently than did the other groups (smaller
methods do not allow estimation of the contri-bution of age and sex to these differences.
The mean choice latency and bet sizes for
this task are shown in Table 2. Analysis of the
(logarithm-transformed) choice latency and the
mean percentage bet size was performed by
separate ANOVA models with ratio condition
included as a within-subject factor. Ratio sig-
nificantly influenced bet size [F(3, 156)=31.10],
but not choice latency (F<1). Crucially, neither
measure was influenced by group, nor were
there any grouprratio interactions (all F ’s<1).
Mean change in percentage false alarm rate between switch
and non-switch trials for the three groups in the Go/No-go task. Error bars represent 2 S.E.D., estimated from the error term of for the
Very few targets were missed : 0.7, 0.9 and 1.0 %
grouprswitch interaction in an ANOVA, using harmonic mean n.
of targets for TS, OCD and control groups
Means and error bars calculated from untransformed values.
respectively. These data are unsuitable forparametric analysis ; Kruskal–Wallis analysis
in Fig. 2. OCD patients had a significantly
revealed no effect of group upon omission errors
greater switch cost (increase in false-positive
[x2(2)=1.16, p>0.5]. Somewhat higher pro-
errors following switch blocks) than did TS
portions of non-targets were responded to (false-
patients [t(56)=2.43], which was also margin-
positive errors) : 11.8, 8.3 and 7.4 of targets for
ally greater than controls [t(56)=1.95, p=0.055].
TS, OCD and control groups respectively.
TS patients were no more or less influenced by
Analysis of these (arcsine-transformed) data
was conducted with block type (switch ornon-switch) as a repeated-measures factor. This
revealed the expected effect of switch, in that
The results from the patient groups were further
subjects made significantly more false-positives
analysed to investigate the effects of medi-
on switch blocks [F(1, 56)=36.78]; any tendency
cation on patient performance. Antipsychotic-
for the groups to differ in overall false-positive
medicated TS patients were significantly more
rate was not significant [F(2, 56)=2.32, p>0.1].
accurate on the spatial recognition memory test
Critically, the detrimental effect of switch on
[U=13.5, p<0.05] than TS patients who were
error rates was significantly influenced by sub-
not taking antipsychotic medication but none of
ject group [F(2, 56)=3.30]; these data are shown
the other core test measures differed between
Cognition in Tourette’s syndrome and OCD
these two groups. There were no significant dif-
new information on previously unstudied as-
ferences between the OCD patient group taking
pects of cognitive functioning in OCD.
SSRIs and the unmedicated OCD patients on
By contrast to their intact verbal fluency,
arithmetic performance, planning and decision-making, OCD patients were selectively im-paired at the ED shift stage of the attentional
set-shifting test. Three previous studies of OCD(Veale et al. 1996 ; Purcell et al. 1997 a, 1998)
This study is the first systematically to compare
have analysed the data for this test differently
a broad range of ‘ frontal ’ executive functions in
by using trials to criterion (rather than errors
TS and OCD. Overall, the results clearly show
to criterion) to index rule learning and Purcell
qualitative similarities in cognitive performance
et al. (1997 a, 1998) did not compare the ID
between TS and OCD with some differences
and ED shift stages directly. Veale et al. (1996)
in the exact form and degree of deficits. This
found gradual attrition throughout the test
profile was particularly evident for the tests of
stages, but their OCD group were mostly in-
inhibitory control where both groups were sig-
nificantly impaired on the shifting component
clinically disabled or had a higher degree of
co-morbidity than the current group, probably
group more significantly so) and at the extra-
resulting in fewer patients attempting the ED
shift stage, thus reducing the power of detect-
attentional-set formation and shifting task. TS
ing differences in attentional set-shifting per se.
patients showed a non-significant tendency to
From Veale et al. (1996) and the current study
have more difficulties with the stages earlier
it appears that ED shift performance in OCD
than the extra-dimensional shift. Thus the OCD
depends on severity ; less clinically impaired
group, in particular, showed impressive evidence
OCD patients (present group) are impaired
of selectivity of deficits at the shifting stages
selectively at the ED shift stage, whereas sev-
erely affected in-patients show attrition at
attentional set-shifting tests. For the tests of
earlier stages. It is relevant to compare the
recognition memory, again both groups were
performance of depressed unipolar patients of
impaired, however, with some differences, for
similar age, where there has been little con-
example the OCD patients had significantly
sistent evidence to support an ED shifting
slowed response latencies. Both groups had
deficit (Purcell et al. 1997 b ; Elliott et al. 1998 ;
spared executive function, in terms of perform-
Sweeney et al. 2000), although this may depend
ance on conventional tests of verbal fluency
on factors such as the severity of depressive
and working memory (WAIS arithmetic), the
TOL test of planning and decision-making tests.
The clear-cut nature of the deficits of the
However, the TS group did show a small deficit
in quality of decision-making. These profiles of
other stages, thus suggests a selective deficit in
cognitive impairment are striking, given the
cognitive flexibility in this group, probably not
close genetic relationship between the two con-
due to depressed mood, but consistent with the
ditions and additional similarities of under-
hypothesis that some of the tendency towards
lying neuropathology (for review, see Leckman
compulsive modes of behaviour and ruminative
et al. 1997 ; Saxena et al. 1998). This discussion
tendencies arises from a generalized impair-
focuses on the cognitive profiles of the two
ment in inhibitory function at the cognitive
patient groups, particularly with respect to their
level that normally allows adaptive shifting be-
relationship to clinical symptoms, and impli-
tween different actions and thoughts. Further
cations for the neuroanatomical bases of these
support for this view can be found in the
significant deficits by the OCD group in theswitching of the Go/No-go reversal task.
Whilst the OCD group neither made signifi-
The data for the OCD group help to resolve
cantly more false-positive errors overall than
inconsistencies in the literature and also provide
controls, nor had a particular difficulty in the
challenging situation of withholding respond-
et al. 1997 a, 1998 ; Schmidtke et al. 1998). Use
ing to a non-target subsequent to a response
of the one-touch TOL in this study has avoided
to the previous target (which is impaired in
the potential confounds of online monitoring
Huntington’s disease patients ; Watkins, L.,
of (and possibly ruminating over) performance
unpublished observations), the OCD group did
(Goel & Grafman, 1995), allowing confirmation
respond excessively to the previously rewarded
of intact planning ability in OCD, which con-
stimulus category (i.e. they perseverated) when
trasts markedly with the impairments seen in
required to reverse response categories on
depressed patients of similar age (Elliott et al.
switch blocks. This reversal is somewhat akin
to tests of simple alternation, in which subjects
The OCD patients were also unimpaired on a
must reverse reward contingencies on each
test of decision-making in which they had to
trial, and which are very sensitive to OCD
select from and ‘ bet ’ on outcomes with dif-
(Abbruzzese et al. 1995 ; Gross-Isseroff et al.
fering probabilities. Although they exhibited
1996 ; Cavedini et al. 1998). Behavioural pro-
some slowing in deliberation time, this was
not significant, and contrasts with the slow-
paradigms have been particularly associated
ing observed in depression. OCD patients are
with the ventro-lateral prefrontal region, from
also unimpaired in accuracy on probabilistic
studies with non-humans (e.g. Iversen &
reasoning tasks (Volans, 1976 ; Fear & Healy,
Mishkin, 1970 ; Butters et al. 1973), patients
with frontal lobe damage (Aron et al. 2003)
Although the robust impairment we observed
and using functional imaging in healthy hu-
in visual recognition memory on this test may
mans (Kawashima et al. 1996 ; Casey et al.
well reflect impaired temporal lobe function
1997 ; Konishi et al. 1998). The OCD patients
(Owen et al. 1995), it is also possible that it
in this study were impaired only when reversing
reflects prefrontal cortex (PFC) dysfunction,
Go/No-go contingencies, suggesting that, as
there being good evidence that the more pos-
well as implicating the ventro-lateral region
terior OFC regions and the anterior cingulate
(see Cools et al. 2002), such a deficit could be
are important in visual recognition memory
more closely related to the reversal deficits seen
(Bachevalier & Mishkin, 1986 ; Elliott & Dolan,
after ventral frontal damage (Daum et al. 1991 ;
1999 ; Frey & Petrides, 2000). The OCD patients
Rolls et al. 1994 ; Dias et al. 1996). Indeed,
were not significantly impaired on the spatial
Rolls et al. (1994) study employed a Go/No-go
recognition memory task, which, in contrast
to visual pattern recognition resembles those
frontal lesion patients although unimpaired on
tests of spatial working memory that activate
the initial Go/No-go discrimination stage, then
the DLPFC (Owen et al. 1996), as well as being
perseverated to the previously correct stimulus
more sensitive to frontal as opposed to tem-
in subsequent reversal stages ; a similar pattern
poral lobe lesions in humans (Owen et al. 1995).
to that seen in the OCD patients here. The
However, the OCD patients were significantly
selectivity of this impairment is particularly
slower on both tasks, which may reflect a speed-
important as the intact Go/No-go performance
error trade-off strategy that compensates effec-
overall by OCD patients shows that they were
tively for spatial working-memory deficits. The
not impaired in global aspects of response in-
lengthened latencies of the OCD patients on
hibition, leading for example, to excessively
the memory recognition tasks were not matched
disinhibited or impulsive responding.
by significant overall slowing on the other tasks.
The deficient performance of OCD patients
However, it should be pointed out that de-
on tests of response inhibition contrasted
pressed patients are also impaired in recognition
markedly with their intact performance on other
‘ frontal ’ executive tests less dependent on in-hibitory processes. The preservation of ‘ look-
ahead ’ planning accuracy in these patients is
By comparison with OCD, the TS group gen-
consistent with previous findings of intact ac-
erally showed qualitatively similar, although
curacy on TOL planning tasks and the related
smaller, deficits, except for the decision-making
Tower of Hanoi task (Veale et al. 1996 ; Purcell
test. Such impairment was unlikely to have
Cognition in Tourette’s syndrome and OCD
preservation also of several aspects of fronto-
TS group since neither the mean ADSA score
(Triolo & Murphy, 1996) nor the mean LOI(Cooper, 1970 ; Snowdon, 1980) score were
Conclusions and implications for the neural
significantly different from normative data
substrates of cognitive deficits in OCD and TS
and neither score correlated with cognitive
This study has identified a distinct profile of
deficits, especially in terms of response inhi-
Overall, the cognitive changes in TS were
bition, in the genetically related disorders of
much less clear-cut than for OCD. Over one-
third of TS patients failed to complete all stages
of cognitive shifting in OCD, despite intact
of the attentional set-shifting test but the pattern
planning and decision-making helps to resolve
was one of gradual attrition, suggesting diffi-
several previous discrepancies in the literature.
culties in set-formation and set-maintenance,
These deficits reflect a general difficulty in shift-
as well as set-shifting. The only previous study
ing of set in OCD patients, which is also seen
comparing performance of TS patients with
in their obsessive and compulsive symptoms,
matched control subjects on the Wisconsin Card
perhaps resulting from impaired functioning
Sorting Test found no evidence for impairment
of fronto-striatal circuitry. The set-shifting im-
(Sutherland et al. 1982). However, the results of
pairments are consistent with dorsolateral and
the current study show that some TS patients
ventrolateral prefrontal dysfunction. However,
have difficulties with set-shifting, and possibly
such dysfunction is unlikely to be global, as
performance on the TOL test, which is sensitive
Possibly the most surprising finding in the
to dorsolateral prefrontal dysfunction (see
TS group was that of relatively intact Go/
Manes et al. 2002), was strikingly unimpaired.
No-go performance. This test was designed to
detect inhibitory problems at three distinct
abilities in a test also sensitive to orbito-frontal
levels of behavioural regulation : general in-
damage (Rogers et al. 1999), also suggests that
ability to withhold responding to non-targets ;
OCD patients do not suffer from global OFC
inability to withhold responding to non-targets
deficits either. Overall, the pattern of fronto-
in the particularly taxing situation of when
executive impairment in OCD is consistent
non-targets directly follow targets ; and in-
with the nature of their clinical symptoms, but
ability to switch between response categories
does not indicate generalized executive mal-
on different blocks. Only for the last measure
function. In comparison, TS patients showed a
was there a statistically marginal tendency for
similar, but less clear-cut pattern of impair-
TS patients to be impaired. Ozonoff et al.
ment on tests of pattern and spatial recognition
(1994) also found intact Go/No-go and Go/
memory, attentional set-formation and shift-
No-go reversal in children with TS. Thus TS
ing and quality of decision-making, consist-
patients appear able to inhibit the well-in-
ent with the genetic relationship with OCD.
tegrated responses required in the Go/No-go
Their limited profile of cognitive impairments,
paradigm. This indicates that tics are not a re-
was not, however, simply restricted to fronto-
sult of fronto-executive inhibitory dysfunction
executive function, including, for example a
operating at a cognitive level of response con-
visual recognition memory deficit. The most
trol, but instead are caused by impairments at a
interesting area of relative preservation of
lower level of response control, possibly striatal
function in TS was for those Go/No-go test
measures of impulsive, as distinct from com-
The TS patients were unimpaired on the one-
pulsive (switching set), modes of responding.
touch TOL, but had a minor deficit in selecting
Thus, the TS patients were able to inhibit highly
the most likely outcome on the decision-making
pre-potent voluntary responses, although their
tests. In summary, the TS patients had some
syndrome is characterized by a difficulty in
significant deficits in decision-making, atten-
suppressing involuntary behaviour. Consistent
tional set-shifting and in visual pattern and
spatial recognition memory accuracy, including
tested here, it is possible that this difference
a test of spatial working memory, but showed
results from impairments in response control
mechanisms at the striatal, rather than the
Bachevalier, J. & Mishkin, M. (1986). Visual recognition impairment
follows ventromedial but not dorsolateral prefrontal lesions inmonkeys. Behavioural Brain Research 20, 249–261.
Baker, S. C., Rogers, R. D., Owen, A. M., Frith, C. D., Dolan, R. J.,
co-morbid feature of OCD and TS, possibly
Frackowiak, R. J. & Robbins, T. W. (1996). Neural systemsengaged by planning : a PET study of the Tower of London task.
However, a recent study by McLean et al. (2004)
Bechara, A., Damasio, H., Tranel, D. & Anderson, S. W. (1998).
Dissociation of working memory from decision making withinthe human prefrontal cortex. Journal of Neuroscience 18, 428–437.
battery, showed a distinctly different profile
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J. E. & Erbaugh,
on the Go/No-go test, ADHD patients being
J. K. (1961). An inventory for measuring depression. Archives
slower to respond but not impaired at shifting,
Benton, A. L. (1968). Different behavioral effects in frontal lobe
and also being worse at planning, than their
disease. Neuropsychologia 6, 53–60.
age-matched controls. Overall, these data are
Braun, A. R., Stoetter, B., Randolph, C., Hsiao, J. K., Vladar, K.,
Gernert, J., Carson, R. E., Herscovitch, P. & Chase, T. N. (1993).
consistent with a cognitive pattern of deficits in
The functional neuroanatomy of Tourette’s syndrome : an FDG-
OCD that mainly appears to contribute to or
PET study. I. Regional changes in cerebral glucose metabolism
promote the perseverative or compulsive tend-
differentiating patients and controls. Neuropsychopharmacology9, 277–291.
ency, rather than reflecting what Hollander &
Butters, N., Butter, C., Rosen, J. & Stein, D. (1973). Behavioural
Rosen (2000) describe as the impulsivity pole of
effects of sequential and one-stage ablations of orbital prefrontal
the compulsive–impulsive spectrum.
cortex in the monkey. Experimental Neurology 39, 204–214.
Cambridge Cognition (2004). CANTAB (www.camcog.com). Cam-
bridge Neuropsychological Test Automated Battery. Cambridge,UK.
Casey, B. J., Trainor, R. J., Orendi, J. L., Schubert, A. B., Nystrom,
L. E., Giedd, J. N., Castellanos, X., Haxby, J. V., Noll, D. C.,Cohen, J. D., Forman, S. D., Dahl, R. E. & Rapoport, J. L. (1997).
We are grateful to the participants of this study
A developmental functional MRI study of prefrontal activation
and their families, to Professor M. Trimble and
during performance of a Go-No-Go task. Journal of Cognitive
Dr E. Krishnamoorthy for help with recruiting
Cavedini, P., Ferri, S., Scarone, S. & Bellodi, L. (1998). Frontal
in the TS clinic and to Dr A. Rosser and Elise
lobe dysfunction in obsessive-compulsive disorder and major de-
DeVito for helpful discussion. This work was
pression : a clinical-neuropsychological study. Psychiatry Research78, 21–28.
Cools R, Clark, L, Owen, A. M. & Robbins, T. W. (2002). Defining
grant (no. 019407) and was completed within
the neural mechanisms of probabilistic reversal learning using
the MRC Centre for Behavioural and Clinical
event-related functional magnetic resonance imaging. Journal ofNeuroscience 22, 4563–4567.
Neuroscience. L.H.A.W. was supported by the
Cooper, J. (1970). The Leyton Obsessional Inventory. Psychological
Huntington’s Disease Association and the
Daum, I., Schugens, M. M., Channon, S., Polkey, C. E. & Gray, J. A.
unilateral temporal or frontal lobe lesions in man. Cortex 27,613–622.
Devinsky, O. (1983). Neuroanatomy of Gilles de la Tourette’s
syndrome. Archives of Neurology 40, 508–514.
Dias, R., Robbins, T. W. & Roberts, A. C. (1996). Dissociation in
B.J.S. and T.W.R. both consult for Cambridge
prefrontal cortex of affective and attentional shifts. Nature 380,
Downes, J. J., Roberts, A. C., Sahakian, B. J., Evenden, J. L.,
Morris, R. G. & Robbins, T. W. (1989). Impaired extra-dimen-sional
Parkinson’s disease. Neuropsychologia 27, 1329–1343.
Drewe, E. A. (1975). Go-No Go learning after frontal lobe lesions in
Abbruzzese, M., Ferri, S. & Scarone, S. (1995). Wisconsin Card
Sorting Test performance in obsessive-compulsive disorder : no
Eapen, V., Pauls, D. L. & Robertson, M. M. (1993). Evidence for
evidence for involvement of dorsolateral prefrontal cortex.
autosomal dominant transmission in Gilles de la Tourette
Syndrome – United Kingdom cohort study. British Journal of
Alexander, G. E., Delong, M. R. & Strick, P. L. (1986). Parallel
organization of functionally segregated circuits linking basal
Elliott, R. & Dolan, R. J. (1999). Differential neural responses during
ganglia and cortex [Review]. Annual Review of Neuroscience 9,
performance of matching and non-matching to sample tasks at
two delay intervals. Journal of Neuroscience 19, 5066–5073.
APA (1994). Diagnostic and Statistical Manual of Mental Disorders
Elliott, R., McKenna, P. J., Robbins, T. W. & Sahakian, B. J. (1998).
(4th edn). American Psychiatric Association : Washington, DC.
Specific neuropsychological deficits in schizophrenic patients
Aron, A. R., Fletcher, P. C., Bullmore, E. T., Sahakian, B. J. &
with preserved intellectual function. Cognitive Neuropsychiatry 3,
Robbins, T. W. (2003). Stop-signal inhibition disrupted by damage
to right inferior frontal gyrus in humans. Nature Neuroscience 6,
Elliott, R., Sahakian, B. J., McKay, A. P., Herrod, J., Paykel, E. S.
& Robbins, T. W. (1996). Neuropsychological impairment in
Cognition in Tourette’s syndrome and OCD
unipolar depression : the influence of perceived failure on sub-
Owen, A. M., Sahakian, B. J., Semple, J., Polkey, C. E. &
sequent performance. Psychological Medicine 26, 975–989.
Robbins, T. W. (1995). Visuospatial short term recognition
Fear, C. F. & Healy, D. (1997). Probabilistic reasoning in obsessive-
memory and learning after temporal lobe excisions, frontal lobe
compulsive and delusional disorders. Psychological Medicine 27,
excisions or amygdale hippocampectomy in man. Neuropsycho-
Folstein, M. F., Folstein, S. E. & McHugh, P. R. (1975). Mini-mental
Ozonoff, S., Strayer, D. L., McMahon, W. M. & Filloux, F. (1994).
state. Journal of Psychiatric Research 12, 189–198.
Executive function abilities in autism and Tourette syndrome : an
Freeman, C. P. (1992). What is obsessive compulsive disorder ?
information processing approach. Journal of Child Psychology and
International Clinical Psychopharmacology 7 (Suppl. 1), 11–17.
Psychiatry, and Allied Disciplines 35, 1015–1032.
Frey, S. & Petrides, M. (2000). Orbitofrontal cortex : a key prefrontal
Pauls, D. L., Alsobrook, J. P., Goodman, W., Rasmussen, S. &
region for encoding information. Proceedings of the National
Leckman, L. F. (1995). A family study of obsessive-compulsive
Academy of Sciences USA 97, 8723–8727.
disorder. American Journal of Psychiatry 152, 76–84.
Godefroy, O., Lhullier, C. & Rousseaux, M. (1996). Non-spatial
Pauls, D. L. & Leckman, J. F. (1986). The inheritance of Gilles de
attention disorders in patients with frontal or posterior brain
la Tourette’s syndrome and associated behaviours : evidence
for autosomal dominant inheritance. New England Journal of
Goel, V. & Grafman, J. (1995). Are the frontal lobes implicated in
planning functions – interpreting data from the Tower of Hanoi.
Petrides, M. (1986). The effect of periarcuate lesions in the monkey
on the performance of symmetrically and asymmetrically
Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C.,
reinforced visual and auditory Go, No-Go tasks. Journal of
Fleischmann, R. L., Hill, C. L., Heninger, G. R. & Charney, D. S.
Purcell, R., Maruff, P., Kyrios, M. & Pantelis, C. (1997 a). Cognitive
Development, use, and reliability. Archives of General Psychiatry
deficits in obsessive-compulsive disorder on tests of frontal-striatal
function. Biological Psychiatry 43, 348–357.
Gross-Isseroff, R., Sasson, Y., Voet, H., Hendler, T., Luca-Haimovici,
Purcell, R., Maruff, P., Kyrios, M. & Pantelis, C. (1997 b).
K., Kandel-Sussman, H. & Zohar, J. (1996). Alternation learning
Neuropsychological function in young patients with unipolar
in obsessive-compulsive disorder. Biological Psychiatry 39,
major depression. Psychological Medicine 27, 1277–1285.
Purcell, R., Maruff, P., Kyrios, M. & Pantelis, C. (1998).
Hollander, E. & Rosen, J. (2000). Impulsivity. Journal of Psycho-
Neuropsychological deficits in obsessive-compulsive disorder.
Archives of General Psychiatry 55, 415–423.
Howell, D. C. (1997). Statistical Methods for Psychology. Duxbury
Rahman, S., Sahakian, B. J., Rogers, R. D., Hodges, J. R. & Robbins,
T. W. (1999). Specific cognitive deficits in early frontal variant
Iversen, S. D. & Mishkin, M. (1970). Perseverative interference in
frontotemporal dementia. Brain 122, 1469–1493.
monkeys following selective lesions of the inferior prefrontal con-
Robbins, T. W. (1977). A critique of the methods available for the
vexity. Experimental Brain Research 11, 376–386.
measurement of spontaneous locomotor activity. In Handbook of
Kawashima, R., Satoh, K., Itoh, H., Ono, S., Furumoto, S., Gotoh, R.,
Psychopharmacology VII (ed. L. L. Iversen and S. D. Iversen),
Koyama, M., Yoshioka, S., Takahashi, T., Thakahashi, K.,
Yanagisawa, T. & Fukuda, H. (1996). Functional anatomy of Go/
Robbins, T. W. (1996). Dissociating executive functions of the
No-Go discrimination and response selection – a PET study in
prefrontal cortex. Philosophical Transactions of the Royal Society
of London. Series B, Biological Sciences 351, 1463–1470.
Konishi, S., Nakajima, K., Uchida, I., Sekihara, K. & Miyashita, Y.
Robertson, M. M. (1994). Gilles de la Tourette Syndrome – an
(1998). No-go dominant brain activity in human inferior pre-
update. Journal of Child Psychology and Psychiatry, and Allied
frontal cortex revealed by functional magnetic resonance imaging.
European Journal of Neuroscience 10, 1209–1213.
Robertson, M. M. (2000). Tourette syndrome : associated conditions
Kullback, S. (1968). Information Theory and Statistics. Dover Press :
and the complexities of treatment. Brain 123, 425–462.
Robertson, M. M. & Eapen, V. (1996). The National Hospital
Lawrence, A. & Sahakian, B. J. (1996). The neuropsychology
Interview Schedule for the assessment of Gilles de la Tourette
of fronto-striatal dementias. In Handbook of the Clinical
Syndrome. International Journal of Methods in Psychiatric
Psychology of Aging (ed. R. T. Woods), pp. 243–265. John Wiley :
Rogers, R. D., Andrews, T. C., Grasby, P. M., Brooks, D. J. &
Leckman, J. F., Peterson, B. S., Anderson, G. M., Arnsten, A. F. T.,
Robbins, T. W. (2000). Contrasting cortical and sub-cortical
Pauls, D. L. & Cohen, D. J. (1997). Pathogenesis of Tourette’s
activations produced by attentional-set shifting and reversal
syndrome. Journal of Child Psychology and Psychiatry, and Allied
learning in humans. Journal of Cognitive Neuroscience 12,
Leckman, J. F., Riddle, M. A., Hardin, M. T., Ort, S. I., Swartz,
Rogers, R. D., Everitt, B. J., Baldacchino, A., Blackshaw, A. J.,
K. L., Stevenson, J. & Cohen, D. J. (1989). The Yale Global Tic
Swainson, R., Wynne, K., Baker, N. B., Hunter, J., Carthy, T.,
Severity Scale : initial testing of a clinician-rated scale of tic sev-
Booker, E., London, M., Deakin, J. F., Sahakian, B. J. & Robbins,
erity. Journal of the American Academy of Child and Adolescent
T. W. (1999). Dissociable deficits in the decision-making cognition
of chronic amphetamine abusers, opiate abusers, patients with
Manes, F., Sahakian, B. J., Clark, L., Rogers, R., Antoun, N., Aitken,
focal damage to prefrontal cortex, and tryptophan-depleted nor-
M. & Robbins, T. W. (2002). Decision making processes following
mal volunteers : evidence for monoaminergic mechanisms. Neuro-
damage to the prefrontal cortex. Brain 125, 624–639.
McLean, A., Dowson, J., Toone, B., Young, S., Bazanis, E., Robbins,
Rolls, E. T., Hornak, J., Wade, D. & McGrath, J. (1994). Emotion-
T. W. & Sahakian, B. J. (2004). Characteristic neurocognitive
related learning in patients with social and emotional changes
profile associated with adult attention-deficit/hyperactivity dis-
associated with frontal lobe damage. Journal of Neurology,
order. Psychological Medicine 34, 681–692.
Neurosurgery and Psychiatry 57, 1518–1524.
Nelson, H. E. (1982). National Adult Reading Test Manual. NFER :
Sahakian, B. J., Morris, R. G., Evenden, J. L., Heald, A., Levy, R.,
Philpot, M. & Robbins, T. W. (1988). A comparative study of
Owen, A. M., Doyon, J., Petrides, M. & Evans, A. C. (1996).
visuospatial memory and learning in Alzheimer-type dementia
Planning and spatial working memory : a positron emission tom-
and Parkinson’s disease. Brain 111, 695–718.
ography study in humans. European Journal of Neuroscience 8,
Saxena, S., Brody, A. L., Schwartz, J. M. & Baxter, L. R.
obsessive-compulsive disorder. British Journal of Psychiatry ; the
(ed. A. J. Friedhoff and T. N. Chase), pp. 311–322. Raven Press :
Journal of Mental Sciences 173 (Suppl. 35), 26–37.
Schmidtke, K., Schorb, A., Winkelmann, G. & Hohagen, F. (1998).
Sweeney, J. A., Kmiec, J. A. & Kupfer, D. J. (2000). Neuro-
Cognitive frontal lobe dysfunction in obsessive-compulsive dis-
psychologic impairments in bipolar and unipolar mood disorders
order. Biological Psychiatry 43, 666–673.
on the CANTAB neurocognitive battery. Biological Psychiatry 48,
Schwartz, J. M. (1998). Neuroanatomical aspects of cognitive-
behavioural therapy response in obsessive-compulsive disorder.
Tranel, D., Anderson, S. W. & Benton, A. (1994). Development of
An evolving perspective on brain and behaviour. British Journal of
the concept of ‘ executive function ’ and its relationship to the
frontal lobes. In Handbook of Neuropsychology (ed. F. Boller and
Snowdon, J. (1980). A comparison of written and postbox forms
J. Grafman), pp. 125–148. Elsevier : Amsterdam.
of the Leyton Obsessional Inventory. Psychological Medicine 10,
Triolo, S. J. & Murphy, K. R. (1996). Attention Deficit Scales for
Adults (ADSA) : Manual for Scoring and Interpretation. Brunner/
SPSS Inc. (2001). SPSS version 11.0.1. Statistical Package for the
Veale, D. M., Sahakian, B. J., Owen, A. M. & Marks, I. M. (1996).
State, M. W., Greally, J. M., Cuker, A., Bowers, P. N., Henegraiu,
Specific cognitive deficits in tests sensitive to frontal lobe dys-
O., Morgan, T. M., Gunel, M., DiLuna, M., King, R. A., Nelson,
function in obsessive-compulsive disorder. Psychological Medicine
C., Donovan, A., Anderson, G. M., Leckman, J. F., Hawkins, T.,
Pauls, D. L., Lifton, R. P. & Ward, D. C. (2003). Epigenetic ab-
Volans, P. J. (1976). Styles of decision-making and probability
normalities associated with a chromosome 18 (q21–q22) inversion
appraisal in selected obsessional and phobic patients. British
and a Gilles de la Tourette syndrome phenotype. Proceedings of
Journal of Social and Clinical Psychology 15, 305–317.
the National Academy of Sciences USA 100, 4684–4689.
Wechsler, D. (1981). Manual for the Wechsler Adult Intelligence
Sutherland, R. J., Kolb, B., Schoel, W. M., Whishaw, I. Q. &
Scale – Revised. Psychological Corporation : New York.
Davies, D. (1982). Neuropsychological assessment of children and
Weeks, R. A., Turjanski, N. & Brooks, D. J. (1996). Tourette’s
adults with Tourette syndrome : a comparison with learning
syndrome : a disorder of cingulate and orbitofrontal function ?
disabilities and schizophrenia. In Gilles de la Tourette Syndrome
Quarterly Journal of Medicine 89, 401–408.
A PSO/ACO Approach to Knowledge Discovery in a Pharmacovigilance Context ABSTRACT at any dose is suspected to have resulted in adverse outcome in a We propose and evaluate the use of a PSO/ACO methodology for classification and rule discovery in the context of medication Given the limitations of premarketing trials, e.g. highly selected postmarketing surveillance or pharmacovigilan
 Cognition in Tourette’s syndrome and OCD
response latencies on these two key dimen-
sional shift stages is possible by contrasting
model as a repeated-measures factor. However,estimates of mean population differences in
performance will be slightly conservative, as the
worst performing subjects in the patient groupsdid not contribute to these stages.
Cognition in Tourette’s syndrome and OCD
response latencies on these two key dimen-
sional shift stages is possible by contrasting
model as a repeated-measures factor. However,estimates of mean population differences in
performance will be slightly conservative, as the
worst performing subjects in the patient groupsdid not contribute to these stages.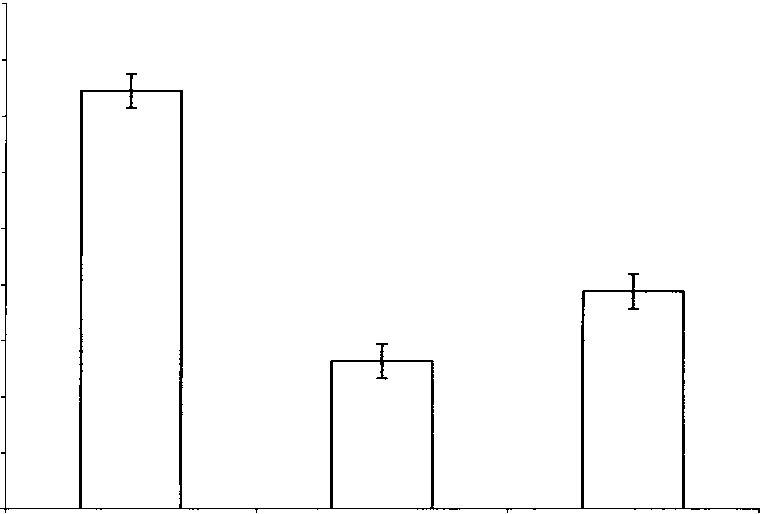 Performance on psychological tests (values are untransformed cell means)
% Bet, mean percentage of points staked on trials on which the more likely outcome was chosen. % First, mean percentage of problems on
which the correct response was chosen first. Analysis revealed no significant differences between groups on these measures.
Performance on psychological tests (values are untransformed cell means)
% Bet, mean percentage of points staked on trials on which the more likely outcome was chosen. % First, mean percentage of problems on
which the correct response was chosen first. Analysis revealed no significant differences between groups on these measures.