Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Untitled
Clinical Kidney Journal Advance Access published December 10, 2013
Clin Kidney J (2013) 0: 1–3doi: 10.1093/ckj/sft141
Renal phospholipidosis possibly induced by ranolazine
Christoph Scheurle1, Maximilian Dämmrich2, Jan U. Becker2 and Martin W. Baumgärtel1
1Medizinische Abteilung, St. Franziskus-Hospital, Münster, Germany and 2Institute of Pathology, Hannover Medical School, Hannover,Germany
Correspondence and offprint requests to: Martin W. Baumgärtel; E-mail: martin.baumgä[email protected]
A 76-year-old male Caucasian patient was treated in our hospital for acutely decompensatedheart failure due to restrictive cardiomyopathy. Acute-on-chronic kidney failure developed withserum creatinine rising from 160 to 345 μmol/L (1.8–3.9 mg/dL); therefore, a kidney biopsy was per-formed. Besides secondary focal-segmental glomerulosclerosis and minimal amyloidosis, histo-logical analysis showed zebra bodies in the cytoplasm of some podocytes, suggesting renalphospholipidosis (PL). Possible causes for this storage disorder encompass Fabry’s disease, in rare
cases silicosis, and an iatrogenic drug-induced aetiology. The main suspects are cationic amphiphi-lic drugs, such as amiodarone and chloroquine. The only cationic amphiphilic drug our patient hadtaken was the anti-anginal ranolazine, a compound not yet associated with PL. The patient hadtaken ranolazine for diastolic dysfunction over a period of 9 months until 6 weeks before renalbiopsy. In the absence of a hereditary disorder, silicosis and well-known pharmaceutical triggers, acausative role of ranolazine seems likely, and this drug should be considered in the differential di-agnosis of drug-induced PL.
Keywords: cationic amphiphilic drugs; myelin bodies; ranolazine; renal phospholipidosis; zebra bodies
benign nephrosclerosis with moderate arteriolar hyalino-sis, fibrosis and kinking and ∼20% cortical tubular atrophy
and interstitial fibrosis and minimal acute tubuloepithelial
A 76-year-old male Caucasian patient was treated in our
damage; Congo-red stains were negative. On ultra struc-
hospital for acutely decompensated heart failure due to
tural examination, podocyte foot process effacement of
restrictive cardiomyopathy. A diagnosis of smouldering
only 5% indicated secondary FSGS. Also, a few mesangial
myeloma (IgG λ) had been made 2 months earlier (serum-
fibrils were found—suspicious, but not diagnostic for
IgG 30.8 g/L [normal range 7.5–15.6 g/L], serum-free light
chain ratio κ/λ: 0.6 [normal range in renal insufficiency
Surprisingly, the cytoplasm of a few podocytes was
0.37–3.1]). Because of the restrictive cardiomyopathy, sys-
ladened with zebra and myelin bodies (see as
temic amyloidosis with cardiac involvement was sus-
described, these bodies are considered to represent an ex-
cessive accumulation of phospholipids in the lysosome,
The patient had chronic kidney disease stage G3bA1
and typically found in phospholipidosis (PL) [, ].
with stable renal function during the previous 12 months
During the next few days after renal biopsy, the
(MDRD-eGFR ∼40 mL/min per 1.73 m2, albuminuria 279
patient’s decompensated heart failure got worse in spite
mg/24 h); his blood pressure was hypo- to normotensive
of intensive diuretic therapy, and renal replacement
(between 90/60 and 120/70 mmHg) and remained so
therapy had to be initiated. After some weeks of dialysis,
cardio-renal function recovered sufficiently to stop extra-
A few days after hospital admission, the patient devel-
oped acute-on-chronic kidney failure with serum creati-nine rising to 345 μmol/l (3.9 mg/dL) and progressive
proteinuria (465 mg/g creatinine, mostly Bence Jones
protein). Urinalysis did not show any casts or haematuria.
As renal involvement of the known gammopathy and
Renal PL is an intracellular storage disease characterized
the suspected amyloidosis was assumed, a kidney biopsy
by accumulation of phospholipids within several types of
renal cells, ranging from mesangial and glomerular endo-
The major light microscopic findings were secondary
thelial cells and podocytes to tubuloepithelial and intersti-
focal and segmental glomerulosclerosis not otherwise
specified (according to the classification proposed by
Electron microscopic analysis shows intra-lysosomal
D’Agati et al. []), affecting 2 of 31 glomeruli, moderate
membranous lamellar inclusions, termed myelin or Zebra
The Author 2013. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved. For permissions, please email: [email protected].
or burning pain), and a normal α-galactosidase A activity
Even though the patient had been exposed to silica over
several years, we did not find any signs of silicosis in ahigh-resolution CAT scan of the chest.
Finally, a drug-induced PL had to be considered [As
cationic amphiphilic drugs (i.e. amiodarone, chloroquine,aminoglycosides) are the main reasons for PL, we stronglysuspected such a drug as the cause. However, the patienthad never taken any of the drugs classically described tocause PL.
The only cationic amphiphilic drug the patient had
taken was the anti-anginal ranolazine, a compound neverpreviously linked to PL. The patient had taken 375 mgranolazine twice daily for diastolic dysfunction over aperiod of 9 months until 6 weeks before renal biopsy. His general physician had discontinued it in order to cutdown on the extensive medication the patient had beenprescribed.
Even though some cases of acute kidney injury have
been attributed to PL induced by cationic amphiphilicdrugs [], PL is generally not believed to have any nega-tive consequences for renal function
In our patient, GFR had remained stable while he was
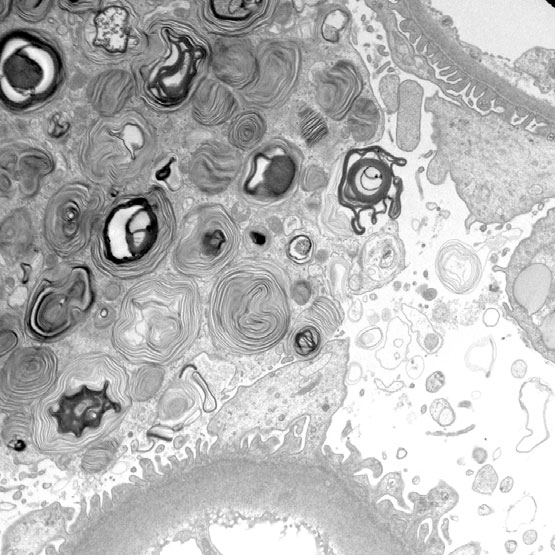
Fig. 1. Transmission electron micrograph of a podocyte with massive
taking ranolazine, and only worsened 6 weeks after rano-
accumulation of zebra bodies and myelin bodies (round structures) within
the cytoplasm. The glomerular basement membrane (top right corner and
lazine had been discontinued; therefore, the drug did not
bottom edge) appears unremarkable, foot processes and glomerular
seem to have any impact on kidney function; neither did
endothelium on either side of the glomerular basement membrane are
the other histological pathologies described above—
well preserved. Original magnification ×6300.
except for the acute tubular damage.
Retrospectively, cardio-renal syndrome due to restrictive
cardiomyopathy was the cause of the patient’s acute-on-
bodies, as the ultra-structural correlate of the accumu-
One can only speculate as to the reason why ranolazine
A decreased activity of lysosomal phospholipase leads
caused PL in this patient. The patient had been prescribed
to an impaired elimination and hence accumulation of
a rather low dose of the drug, and had not taken a larger
phospholipids in the lysosomes. Several organs besides
the kidney may be involved, i.e. lung, liver and heart [].
A dosage adjustment is recommended only when crea-
Hereditary as well as acquired causes of reduced phos-
tinine clearance falls below 30 mL/min and therefore did
not seem necessary in our patient (initial MDRD-eGFR of
Fabry’s syndrome is an X-linked disease. An inborn
mutation results in a reduced activity of α-galactosidase A
However, our patient had low muscle mass, so the real
and consecutively in systemic PL []. Renal symptoms
GFR may lie well under the creatinine-based estimated
usually include a progressive loss of renal function and
proteinuria; Fanconi syndrome has been described in
Considering the (minimal) amyloidosis, it is tempting to
some cases []. Angiokeratomas and neuropathic pain are
draw an analogy to digitalis toxicity in this disease. As
typical extra-renal manifestations [Cardiac involve-
early as 1981, Rubinow et al. [] described that isolated
ment (such as left ventricular hypertrophy, coronary
amyloid fibrils bind digoxin and suggested this phenom-
artery disease, conduction abnormalities) is common and
enon as the reason for increased digitalis toxicity in amy-
loidosis. It is beyond the scope of this report to test this
Acquired PL is mostly iatrogenic and caused by a variety
hypothesis, but one may well conjecture that a similar
of drugs. Typically, cationic amphiphilic substances, such
mechanism concerning ranolazine might play a role in
as amiodarone, chloroquine and aminoglycosides, induce
this case of renal PL. To the best of our knowledge, no
PL [, , ], probably all except the latter without any
association between monoclonal gammopathy or amyloi-
dosis and PL has ever been described in the literature.
In rare instances, exposure to silica may lead to similar
Thus, in the absence of any other likely causative
histological changes and mimic Fabry’s disease [
factors, ranolazine should be considered in the differential
Therefore, the histological finding of renal PL should
lead to an extensive search for possible causes of thisstorage disorder.
Since it is virtually impossible to distinguish an iatro-
Conflict of interest statement. None declared.
genic drug-induced PL from Fabry’s disease on ultra-struc-
tural analysis of kidney tissue, the clinician has to use thepatient’s family history, extra-renal symptoms, and bio-
chemical features, such as a reduced α-galactosidase A
activity, to differentiate these two entities.
1. D’Agati VD, Fogo AB, Bruijn JA et al. Pathologic classification
In our case, the patient’s negative family history, the
of focal segmental glomerulosclerosis: a working proposal.
absence of typical signs or symptoms (i.e. angiokeratoma
Renal phospholipidosis possibly induced by ranolazine
2. Bracamonte ER, Kowalewska J, Starr J et al. Iatrogenic phos-
8. Stratta P, Quaglia M, Messina M et al. The challenges of diag-
pholipidosis mimicking Fabry disease. Am J Kidney Dis 2006;
nosing Fabry disease. Am J Kidney Dis 2008; 51(5): 860–864
9. Waldek S, Manesh RP, Banikaemi B et al. Life expectancy and
3. Zarate YA, Hopkin RJ. Fabry’s disease. Lancet 2008; 372:
cause of death in males and females with Fabry disease: find-
ings from the Fabry Registry. Genet Med 2009; 11(11): 790–796
4. Reasor MJ, Hastings KL, Ulrich RG. Drug-induced phospholipi-
10. Albay D, Adler SG, Philipose J et al. Chloroquine-induced lipido-
dosis: issues and future directions. Expert Opin Drug Saf 2006;
sis mimicking Fabry disease. Mod Pathol 2004; 18(5): 733–738
11. Müller-Höcker J, Schmid H, Weiss M et al. Chloroquine-
5. Reasor MJ, Kacew S. Drug-induced phospholipidosis: are there
induced phospholipidosis of the kidney mimicking Fabry’s
functional consequences? Exp Biol Med 2001; 226(9):
disease: case report and review of the literature. Hum Pathol
6. Halliwell WH. Cationic amphiphilic drug-induced phospholipi-
12. Pairach P, Cook WJ. Progressive renal insufficiency associated
dosis. Toxicol Pathol 1996; 25(1): 53–60
with renal phospholipidosis. Kidney Int 2008; 74: 1354–1357
7. Terryn W, Cochat P, Froissart R et al. Fabry nephropathy: indi-
13. Rubinow A, Skinner M, Cohen AS. Digoxin sensitivity in
cations for screening and guidance for diagnosis and treat-
amyloid cardiomyopathy. Circulation 1981; 63(6): 1285–1288
ment by the European Renal Best Practice. Nephrol DialTransplant 2013; 28(3): 505–517
Received for publication: 22.2.13; Accepted in revised form: 7.11.13
New Zealand Code of Practice Medical Emergencies in Dental Practice Endorsed by DCNZ March 2005 CONTENTS CODE OF PRACTICE Introduction …………………………………………………………………… 3 Preparation for Emergencies ……………………………………………. 3-4 ……………………………………………………………
Mitteilungsblatt Fleischforschung Kulmbach (2012) 51, Nr. 195 – Praxis-Informationen Die Medikation bewirkte eine größere Anzahl und Homogenität in dem Set von Resistenz-genen unter den behandelten Individuen. Zudem war eine erhebliche Zunahme der Häufig-keit von 23 Resistenzgenen detektierbar. Das betraf v. a. die Gruppen der Effluxpumpen und Sulfonamidresistenzen. Die Zunahme der Häuf
 or burning pain), and a normal α-galactosidase A activity
Even though the patient had been exposed to silica over
several years, we did not find any signs of silicosis in ahigh-resolution CAT scan of the chest.
or burning pain), and a normal α-galactosidase A activity
Even though the patient had been exposed to silica over
several years, we did not find any signs of silicosis in ahigh-resolution CAT scan of the chest.