Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
$-amyloid
Unspecific Effects of Caffeine Consumption: When Does the Mind Overrule the Body? Rainer Schneider
University of Osnabrück, Department of Human Sciences,
Differential Psychology and Personality Psychology,
Seminarstr. 20, 49074 Osnabrück, Germany
Abstract
Although much is known about the pharmacokinetics of caffeine (i.e., what the body
does to the drug), its pharmacodynamics (i.e., what the drug does to the body) are less well understood. Specifically, the psychological effects associated with caffeine intake may often run counter to what might be expected pharmacologically. Being one of the most consumed stimulants worldwide the instrumental value of caffeine covers a broad range of partially opposing ends. For example, the effect (caffeinated) coffee exerts on human functioning depends to a great deal on the expectation of the consumer. People drink coffee to get started in morning, to enhance performance, or even to unwind after straining experiences. Likewise, the instrumental value of coffee consumption may be bound to psychosocial factors, such as enhancing group coherence. Also, coffee may be consumed for diet-related health issues to prevent diseases like diabetes, cancer, heart diseases, or gastrointestinal problems.
In this chapter, an overview of placebo studies is given to demonstrate the
importance of psychological factors. Specifically, results from the so called placebo caffeine paradigm will be discussed to show that the study of the placebo caffeine effect lends itself to a better understanding of the psychological factors involved with caffeine effects. Several ways to methodologically disentangle pharmacologic and psychological effects will be introduced. From this, it will be concluded that the widely employed way of testing drug effects (the Randomized Control Trial) is insufficient to fully understand
∗ Tel.: ++49 761 476 67 75, Email: [email protected]
the health effect of caffeine since it is aimed at minimizing psychological factors enhancing the effect (e.g., learning effects, expectation, context). It will be shown that the health effects of caffeine are brought about by synergistically intertwined specific and non-specific factors, which, in real-life situations, always work together and make up the totality of effects. Finally, a functionally oriented psychological theory will be introduced helping to explore the psychological mechanisms associated with unspecific effects.
1. Introduction
Caffeine has a long history of use. Its consumption dates back to early mankind and has
taken many forms. In tea, it has been savored in Asia for almost 5,000 years, in coffee humans have consumed it for some 1,000 years. Over the last hundred years, cola drinks, ready-to-drink tea and coffee beverages have steadily gained in popularity. Today, coffee is the second most consumed beverage in the world next to water. The fact that caffeine is the most widely consumed behaviorally active substance in the world has made it subject to vigorous scientific investigation. The biochemical mechanisms underlying the actions of caffeine are well understood. If consumed in doses habitually consumed by humans, caffeine primarily blocks adenosine A1 and A2A receptors, causing a parallel increase in motor activity and decrease in the expression of genes throughout brain regions like the caudate-putamen and nucleus accumbens (Fredholm, Bättig, Holmén, Nehlig, and Zvartau, 1999; Svenningsson, Nomikos, Ongini, and Fredholm, 1997). Unlike other stimulants (e.g., cocaine), caffeine does not significantly increase the release of dopamine or activate the D1 neurotransmission in the nucleus accumbens. Rather, it increases transmission through cells equipped with dopamine D2 receptors in this nucleus and throughout the basal ganglia. Since the effect is inhibitory in nature, the overall activity of this brain region is much less affected by caffeine. Its effects are biphasic with low doses being stimulant and pleasant and high doses being aversive and disturbing. This U-shaped dose-response determines whether caffeine can act as reinforcing agent and thus enhance beneficial effects on subjects.
The behavioral effects of caffeine cover a broad range of phenomena like increased
subjective alertness, improved reaction time, and enhanced encoding of novel information. For example, in a series of related studies on central nervous effects (Ruijter, De Ruiter, Snel, and Lorist, 2000; Ruijter, Lorist, and Snel, 1999; Ruijter, Lorist, and Snel, 2000; Ruijter, Lorist, Snel, and Ruiter, 2000) caffeine was found to have increasing properties on arousal sustaining attention and attenuating vigilance decrements. This was evidenced by increased amplitudes of different ERPs (event related potentials) in EEG recordings in fatigued participants, showing for example in the frontal P2 and the parietal P3 component. Caffeine displays its effect in the brain in the working memory and higher level control and co-coordinating functions (prefrontal cortex) as well as heightened information processing (parietal cortex). However, although caffeine is supposed to have a general arousing effect due to the binding of adenosine to its receptor sites resulting in an increase in the levels of other neurotransmitters (e.g., acetylcholine, noradrenaline, dopamine, and serotonin), information processing is more pronouncedly affected under conditions in which availability of energetical resources is insufficient (e.g. tiredness or boredom). Moreover, beneficial effects on tasks involving cognitive performance appear to be mainly expected for tasks of
Unspecific Effects of Caffeine Consumption
little complexity showing predominantly in the output stage of the information processing (Lorist and Topsa, 2003).
Despite the still growing body of knowledge about the effects of caffeine on, for
instance, peripheral physiology (cardiovascular system), sleep, mood, arousal, and pain, the pattern of results is far from being homogeneous. In fact, many findings somewhat contradict the fundamental aspects of psychopharmacology with regard to motor, psychomotor, and cognitive performance. Evidently, there appears to be a dissociation between the pharmacokinetics of caffeine (i.e., what the body does to the drug) and its pharmacodynamics (i.e., what the drug does to the body). This instigated a debate arising in the mid 1990s by James (1994) who contended that studies conducted over several decades contained one fundamental methodological flaw by merely including placebo controls without heeding participants’ habitual caffeine intake. According to this line of reasoning, abstinence prior to study participation could result in withdrawal symptoms like headache, sleepiness, or lack of concentration. Hence, the performance and mood effect of caffeine would not reflect a real net gain but rather a restoration of decrements to normal levels of functioning. Therefore, the beneficial effects seen in caffeine would simply be counter-regulating detrimental withdrawal symptoms. In fact, there is empirical evidence for the tenability of this claim (James, 1998; James and Gregg, 2004; James, Gregg, Kane, and Harte, 2005; Phillips-Bute and Lane, 1998; Rogers, Martin, Smith, Heatherley, and Smit, 2003; Yeomans, Ripley, Davies, Rusted, and Rogers, 2002). Interestingly, according to the withdrawal hypothesis, caffeine actually has a detrimental effect on mood quality and cognitive performance.
There are, however, empirical findings which cannot be fully reconciled with the
withdrawal effect. For example, Smit and Rogers (2000) demonstrated psychostimulant properties after overnight caffeine abstinence with surprisingly small doses (12.5 mg) for both high and low caffeine consumers. Quite counter-intuitively, the effects found in this study failed to increase as a function of the doses administered, i.e. a dose eight times higher did not show significant increments. In a study including multiple doses of caffeine, regular coffee consumers who were fatigued by carrying out a prolonged testing schedule reported more positive mood and improved performance on a number of different tasks (Smith, Sutherland, and Christopher, 2005). In a series of double-blind, randomized, controlled experiments investigating the role of hidden versus open administration of caffeine in regular coffee consumers involving a caffeine abstinence period of at least 12 hours, very large effects were found for caffeine consumption compared to control groups in primarily cardiovascular measures (Schneider et al., 2006; Schneider and Walach, in preparation). Moreover, in one experiment employing the use of decaffeinated coffee (Experiment 1, Schneider et al., 2006), participants believing to have consumed a strong cup of coffee reported elevated alertness. Post-hoc analyses showed that this effect was not attributable to caffeine cravings or differences in withdrawal symptoms associated with fasting and caffeine abstinence.
Obviously, the impact caffeine has on human health and performance is multifaceted. It
is clear from the heterogeneity of the findings that the effects may dissociate significantly depending on the method used. Besides specific effects like drug dose, sample compositions, or drinking habits, so called unspecific effects have thus far been widely neglected. Unspecific effects refer to the fact that their underlying mechanisms are as yet unknown
(Schneider, 2007). Unlike other beverages predominantly serving a more fundamental satisfaction of basic biological needs (e.g., water), consumption of caffeine, for instance in the form of coffee, serves many different purposes. These are psychological and psychosocial in nature and thus bound to cognitions (e.g., expectations) and learning experience. For example, an athlete ingesting caffeine prior to working out will ascribe a totally different instrumental value to a cup of coffee than a business manager who socializes with a partner during a meeting. Since large epidemiological studies support the notion that caffeine may have beneficial effects on health, for example as a protective agent in high-risk individuals with liver diseases (American Gastroenterological Association, 2005), caffeine may be assumed to be increasingly consumed for dietary and health care reasons.
In the following, I will outline a fundamental fallacy associated with the thinking that
drug effects can unambiguously be reduced to specific effects to understand their modes of action. It will be shown that this mindset is deeply rooted in the belief that placebo administration in experiments is an exclusive way to control for unwanted effects (artifacts) not otherwise regarded meaningful in explaining the drug effect.
2. Placebo Caffeine Effects
The use of placebos in clinical trials dates back to the introduction of the Randomized Controlled Trial (RCT) in 1948 (British Medical Journal, 1998). Since then it has become the gold standard and cornerstone of pharmacologic efficacy testing (Biller-Andorno, 2004). The logic behind using placebos is that a pharmacological agent should show its superiority to a “sugar pill” exempt from any specific contents. Administration of placebos grounds on the reasoning that any effects emerging are artificial and therefore neglectable. Such confounds encompass the regression to the mean, the natural course of a disease, or spontaneous fluctuations (Kienle and Kiene, 1997). Clinical testing practice, however, shows that placebo responses may considerably compromise the interpretation of trials. Despite the notorious lack of published negative results (which is referred to as the file drawer problem), reviews of existing data bases, for example from the US pharmacologic industry on depression, show a remarkably high rate of non-superiority of pharmacologic agents over placebo (Kirsch, Scoboria, and Moore, 2002; Thase, 1999). Attempts to minimize placebo effects, for instance by identifying placebo responders in placebo run-in phases of clinical trials, largely fail (Lee, Walker, Jakul, and Sexton, 2004). Because placebo effects are to a great deal difficult to replicate, and hence hard to predict, they are considered unspecific. However, active treatment effects, too, are at times unpredictable and unspecific. For example, surreptitiously administered analgesics sometimes exert smaller or even no specific effects at all (Pollo, Vighetti, Rainero, and Benedetti, 2003). From this it may be concluded that the modern biomedical tradition risks being too overly reductionistic by merely focusing on specific treatment components.
There has been much controversy on the real nature of placebo effects. While there have
been overly enthusiastic claims on the powerfulness of placebo effects (Beecher, 1955), in part justified methodological critique has at times been too undifferentiated regarding the conditions which are placebo-responsive and those which are not (Hróbjartsson and
Unspecific Effects of Caffeine Consumption
Gøtzsche, 2004). There is a growing body of evidence substantiating the therapeutic relevance of placebo effects across a wide range of phenomena (Sauro and Greenberg, 2005; Stolk, ten Berg, Hemels, and Einarson, 2003; ter Riet, de Craen, de Boer, and Kessels, 1998; Turner, Deyo, Loeser, von Korff, and Fordyce, 1994; Vase, Riley, and Price, 2002; Vase, Robinson, Verne, and Price, 2003; Vase, Robinson, and Price, 2005).
Nonetheless, there also has been much confusion. One central misunderstanding
regarding placebo effects revolves around definitional clarity. For example, obviously factually wrong definitions attribute to placebos a causative mechanism (cf. Moerman and Jonas, 2002). Fortunately, recent definitions have proven more fruitful. One proposition suggests to regard placebo effects as psychosocial context effects arising from treatment or therapy (Benedetti, 2006). Another related definition points to the meaning of an intervention to which an individual responds (Moerman and Jonas, 2002). These definitions have the advantage to be positive, semiotic, and theory-independent. However, as will be shown later, they do not spell out the psychological mechanisms necessary for placebo effects to show. I will therefore suggest a new definition heeding functional properties.
Much from what has been learned about placebo effects stems from experimental
placebo research. In a nutshell, experimental placebo designs vary conditions such that the probability of the occurrence of the effect is maximized. Unlike in RCTs where subjective probability for placebo administration is set at .5, participants in experimental placebo research are made to believe to receive an active agent when actually given a placebo. From the many models available, the placebo caffeine paradigm particularly lends itself to study placebo effects mainly due to two reasons. First, the effects can be studied in healthy individuals, and second, people share a common cultural stereotype about how coffee operates and what effects are to be expected. There are a number of findings supporting the usefulness of the placebo caffeine paradigm. For example, Kirsch and Weixel (1988) showed that a deceptive administration of placebo caffeine (i.e. decaffeinated coffee) produced an increase on pulse rate, systolic blood pressure, and subjective mood. The magnitude of this effect was paralleled by participants’ confidence that they had in fact consumed caffeine. On the other hand, double-blind administration of decaffeinated coffee produced placebo responses which were approximate mirror images of those found for deceptive placebo administration. Studies varying the expectation about caffeine effects found that positive (enhancing) expectations predicted the placebo effect even when no active agent was administered. Participants who were not instructed, and thus did not have any particular belief about the beverage, did not display any change in psychomotor performance (Fillmore and Vogel-Sprott, 1992; Fillmore, Mulvihill, and Vogel-Sprott, 1994). In a study disentangling expectancy and pharmacologic effects by providing different types of information on the content of the beverages (caffeinated and decaffeinated coffee), different responses were found for different measures. Whilst pharmacologic factors primarily influenced participants’ physiology (blood pressure), expectancy about the drug primarily affected self-reported mood and assessment of performance (Fillmore and Blumenthal, 1992). The modulating effects of expectancy were also demonstrated in a study by Fillmore, Roach, and Rice (2002). Alcohol drinkers who expected an antagonist effect of caffeine showed greater impairment in a pursuit rotor task from alcohol than those expecting no such effect. More importantly, expectancy effects were independent of whether caffeine of placebo
caffeine was administered. This finding is interesting inasmuch as little or no actual antagonist effect of caffeine can be expected on alcohol-induced impairment. In a recent study by Anderson & Horne (in press), sleepy participants were given a cup of decaffeinated coffee and verbally primed to suggest caffeinated coffee. Results showed significantly fewer lapses and shorter reaction times compared to a control group. These results are interesting inasmuch as they relativize the withdrawal effect of caffeine mentioned earlier. Specifically, the alleged restoration of decrements to normal levels of functioning is not dependend on caffeine, but can be elicited by means of suggestion.
It should be noted, however, that placebo effects show in different measures to varying
degrees and establishing the most sensitive indicators is challenging. For example, two studies failed to demonstrate placebo caffeine effects (Walach, Schmidt, Bihr, and Wiesch, 2001; Walach, Schmidt, Dirhold, and Nosch, 2002). While the reproduction of placebo effects is dependent on many as yet not fully understood boundary conditions (Schneider, 2007), the Walach et al. studies most probably failed due to an insufficient induction of a strong expectation and/or the use of rather insensitive measurements. For example, a series of studies investigating caffeine-associated stimuli and information, administering caffeine or placebo in either orange juice or coffee, caffeine-associated stimuli (taste, smell) increased physiological arousal (Flaten and Blumenthal, 1999; Mikalsen, Bertelsen, and Flaten, 2001). Information about the content of the beverage also modulated arousal in the direction indicated by the information. In two recent experiments disentangling pharmacologic from psychological effects by investigating social stereotypes of decaffeinated coffee (smell and taste), no modulating effect on pharmacologic effects could be found (Schneider et al., 2006a). Rather, stimuli-associated stimuli showed to be an important prerequisite for the placebo effect to show (i.e., decaffeinated coffee produced a placebo effect). This pattern of result was paralleled by two subsequently conducted experiments only administering orange juice which was either caffeinated or not (Schneider et al., in preparation). Yet, despite large pharmacologic effects, misinformed information about the alleged content of the beverage did not suffice to produce placebo effects.
3. Mechanisms of the Placebo Caffeine Effect
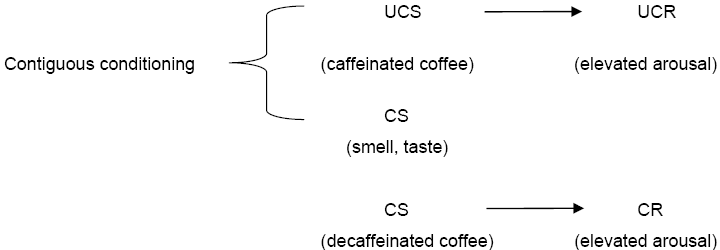
Traditionally, two approaches have been put forward to explain placebo effects.
According to the mentalistic theory, individuals’ cognitions like expectations, meaning, needs, or wishes determine the effect (Kirsch, 1999). According to the conditioning theory, placebo effects are the result of learning processes, i.e. the pairing of unconditioned and conditioned stimuli (Ader, 1993; Wickrameskera, 1980). Figure 1 displays the learning model for placebo caffeine affects. They can be regarded the consequence of the pairing of the unconditioned stimulus [UCS] caffeine with the conditioned stimuli [CS] taste and smell. Hence, the unconditioned reaction [UCR] arousal is elicited by the CS making arousal a conditioned reaction [CR].
Unspecific Effects of Caffeine Consumption
Figure 1. The caffeine placebo effect as a result of conditioned learning.
It should be noted that both approaches are not necessarily mutually exclusive. In fact,
they are often synergistic. Unfortunately, unlike other placebo effect phenomena, the neurobiological mechanisms of the caffeine placebo effect have not yet been subjected to investigation. Placebo analgesia, for example, has been found to be maximal when expectation and conditioning are combined (Amanzio and Benedetti, 1999; Colloca and Benedetti, 2006). Yet, expectancy effects have shown to be associated with a different neurological pathway than conditioning effects: Placebo analgesic effects bearing on expectation can be blocked with the opioid antagonist naloxone. Placebo effects brought about by a conditioned treatment (i.e. the injection) with a non-steroid anti-inflammatory drug (ketorolac), have a different pathway because they can’t be inhibited. Furthermore, a number of several studies have demonstrated that placebo effects involve different brain areas than pharmacologic effects. These involve subcortical processes (e.g., in pain sensitive neuroanatomical areas via opioid release) and cortical ones (via cognitive appraisal), with the latter occurring after some latency and mostly affecting pain experience (Wager, et. al, 2004; Wager, 2005). Similar findings on the mediating role of the prefrontal cortex in placebo effects have been reported on a broad range of symptoms like depression, irritable bowl syndrome, or chronic pain (cf. Pacheco-Lopez, Engler, Niemi, and Schedlowski, 2006; Schneider, 2007) Consequently, when expectations are engaged, the prefrontal cortex, which maintains evaluative information for control and self-knowledge (Craik et al., 1999; Fuster, 2000), exerts a top-down control modulating experience and physiological processes. It is important to note that expectations need not necessarily be conscious in order to exert a placebo effect (Turner, Jensen, Warms, and Cardenas, 2002). As shown above, from the many effects observed for caffeine ingestion, it may be assumed that in addition to the specific (pharmacologic) effects of caffeine, unspecific (psychological) mechanisms exert an influential role over and above specific ones. This requires a somewhat different methodological approach to fully understand the impact of caffeine on health.
4. Methodological Approaches
Several suggestions have been proposed to study the placebo effect. Benedetti (2006)
suggested to surreptitiously administer the pharmacologic agent in order to exempt the treatment form the unspecific effects elicited by the psychosocial context. In so doing, the
proportion of the placebo effect can be determined when open and hidden administrations are compared. Although this is a straightforward methodology, it may be questioned whether its ecological validity is sound. For example, to determine bio-availability, absorption rate and pharmacodynamics of caffeine, hidden administration of the agent is likely to have different effects than oral ingestion. Therefore, to study the effects of caffeine under real life conditions this experimental paradigm is not viable.
Another way of studying pharmacologic and psychological factors of caffeine
consumption is suggested by the so called balanced placebo design (Marlatt and Rohsenow, 1980). It combines the usual placebo design with an “antiplacebo” design resulting in a 2(drug, placebo) x 2(expectation, no expectation) arrangement. By administering placebo and drug under conditions in which the participants expect to receive an inert substance, independent effects of psychological and pharmacologic effects can be parceled out. As can be seen in Figure 2 (dotted line), a “true” pharmacologic effect would be obtained in an experimental condition were participants are given caffeine but are told to have received placebo.
Figure 2. The extended balanced placebo design; Placebo effect: Placebo response minus control.
Likewise, when placebo is given but participants are told they ingested caffeine, placebo
responses are discernable. It is, however, important to note that the balanced placebo design is only able to unravel placebo responses but not placebo effects. This is because placebo responses comprise both placebo effects and confounds like artifacts, spontaneous remission, regression effects and the like (Ernst and Resch, 2003; Kirsch and Sapirstein, 1999). Hence, to determine placebo effects the balanced placebo design must be “extended” by including a zero control group with which placebo responses are compared (solid line).
The balanced placebo design has been primarily used in alcohol research with
expectancy effects comparable to drug effects (for an overview see Marlatt and Rohsenow, 1980). Since then, it has only seldom been fully employed and somewhat fell into oblivion (for a few exceptions, cf. Juliano and Brandon, 2002; Perkins et al., 2004; Perkins et al., 2008). In placebo caffeine research, this is partly due to the fact that placebo response effects showed as main effects having subsequent researchers focus on comparisons of placebo and control group.
Research on the effects of caffeine on health would benefit greatly from employing the
extended balanced placebo design to study the relationship between specific and unspecific effects. However, to understand unspecific effects from a psychological point of view, it may not suffice to primarily focus on conscious thought contents in determining expectations or
Unspecific Effects of Caffeine Consumption
meaning. This is because people only have limited access to mental processes and cannot fully or adequately explicate (verbalize) them. This is suggested by neurobiological findings showing implicit and parallel-holistic processes of the brain (Beeman, Friedman, Perez, Diamond, and Lindsay, 1994; Beeman and Bowden, 2000; Bowden and Beeman, 1998; Bowers, Regehr, Balthazard, and Parker, 1990; Rumelhart and McClelland, 1986) and that these processes also comprise functional properties like self-regulation, motivation, or affect (Craik et al., 1999; Keenan, Nelson, O'Connor, and Pascual-Leone, 2001; Nadel and Moscovitch, 1997; Quirin, Kazén, Rohrmann, and Kuhl, in press; Quirin, Koole, Baumann, Kazén, and Kuhl, 2007; Rotenberg and Weinberg, 1999; Wheeler, Stuss, and Tulving, 1997). Thus, in placebo research, simply asking people about their cognitions may not suffice when meaning and expectations are assessed. Yet, functional approaches, uncovering subsystems describable in terms of classes of functions, have not been employed in placebo research. In the following, a functionally oriented theory is introduced according to which psychologically important subsystems can be evaluated for their significance of placebo effects.
5. Dynamics of Psychological Functions: Personality-Systems-Interaction Theory
Within the framework of Personality-Systems-Interaction (PSI) Theory a comprehensive
functional approach has been developed which lends itself to studying placebo effects (Kuhl, 2000; Kuhl, 2001). The theory comprises two high-level and two low-level systems. These systems may be regarded as complex personality aggregates characterized by distinct functional properties. The two experiential systems generating expectations, and therefore associated with the placebo effect, are extension memory and object recognition. The two behavioral systems are not directly implicated in placebo effects. They are called intention memory and intuitive behavior control with the first being high-inferential and the latter being elementary (see Figure 3). For the sake of simplicity, they will not be further discussed here.
Extension memory is high inferential (complex) and object recognition is low inferential
(elementary). Their activational characteristics are antagonistic, that is, activation of extension memory decreases the activation of object recognition and vice versa. This is depicted by the change of colors in the arrows connecting the antagonist systems. Extension memory derives its denomination from the neuronal fabric of the right prefrontal cortex which consists of extended associative networks (Scheibel et al., 1985; Bowden and Beeman, 1998). These allow for a simultaneous, sub-symbolic computation of a vast number of constraints and multiple inputs from both cognitive and affective subsystems through parallel-processing. Extension memory is a central executive system which simultaneously integrates almost unlimited amounts of information. Extension memory also forms the basis for implicit self-representations (so called autonoetic knowledge), that is, integrated representations of internal states, needs, emotions, somatic feelings, or autobiographical experiences (Keenan et al., 2001; McClelland, Koestner, and Weinberger, 1989; Nyberg,
Cabeza, and Tulving, 1996; Wheeler et al., 1997). Moreover, functions of extension memory also encompass attention processes (vigilance) and enhance those perceptual contents which match actual relevant and implicit networks of needs, expectations, and other self-structures. Due to this characteristic, processes of extension memory are not fully conscious. One of the typical functions of extension memory is down-regulation of negative affect elicited by aversive, threatening or unpredictable experiences because extension memory is tightly linked with vegetative and somatosensory processes (Borod and Madigan, 2000; Garavan, Ross, and Stein, 1999; Kapur et al., 1995; Rotenberg, 2004). This is shown as self-relaxation in Figure 3.
Left Hemisphere Right Hemisphere Intention Memory Extension Memory Thinking Self-relaxation Self-motivation Object Recognition Behavior Control
Generation of “restricted” expectations
Sensation Intuition
Figure 3. Personality-System-Interaction Theory (PSI).
In contrast, object recognition serves to recognize percepts which can be abstracted
(discerned) from their background by specific discrepancy mediating features, for example, concrete things, singular aspects, feelings, sensations etc. Specifically, the system enhances those objects deviating from expectations and self-aspects activated in extension memory. Object recognition is closely linked with one of the cornerstones of cortical pathways (the so-called vision-for-perception stream) where information generated in the primary visual cortex projects into the inferior temporal cortex and further in the prefrontal cortex (Ungerleider and Mishkin, 1982). However, the functional characteristics of object recognition are not limited to these neurological pathways but encompass a number of additional features. As a primarily perceptual system, object recognition focuses on explicit identification and recognition of elementary sensations (e.g., a visual object, an emotion, or semantic category). Characteristic for object recognition (especially in connection with negative affect) is a focus on
Unspecific Effects of Caffeine Consumption
discrepancies and on sensations that diverge from previously held expectations, wishes and the like. Contrary to the functional properties of extension memory, object recognition allows for an explicit, conscious registration of sensory impressions, which encompasses a relatively rigid analytical categorization (i.e., black/white).
6. The Placebo Effect Revisited: Expectation, Meaning, and Their Functional Significance
According to personality systems interaction (PSI) theory, functional properties
determine the powerfulness of placebo-associated expectations and meaning. In other words, different responses follow depending on whether the expectation is generated in extension memory or in the object recognition system. As noted above, strong placebo effects have been found when the meaning of the placebo (treatment) was personally relevant to the participants. This is especially the case for highly aversive states like pain (Zubieta, Yau, Scott, and Stohler, 2006), but basically also holds for placebo caffeine effects (or similar drug effects for that matter). Put differently, only those context factors elicit a placebo effect that are generated and represented in a semantic network of remote associations and coherent complexes of symbolic meaning (extension memory). Furthermore, only expectations generated in extension memory should be accompanied by a placebo effect because extension memory is closely linked with self-regulatory mechanisms affecting a variety of cognitive and somatosensory processes. In contrast, expectations generated in the object recognition system would not suffice to produce significant placebo effects because they lack the connectedness to relevant (meaningful) self-aspects and the network of remote associations requiring (implicit) attention processes (i.e., rare or unexpected effects). Remote associations indeed may be an important prerequisite to elicit placebo effects. For example, Dinnerstein and Halm (1970) and Lyerly, Krugman, and Clyde (1964) found expectancy effects only for experimental conditions where drug effects were introduced as a continuum of possible reactions. Furthermore, as noted above, a number of studies support the notion that placebo effects incorporate self-regulatory mechanisms of the prefrontal cortex which cannot be found for drug effects. This would indicate that active treatment impairs self-regulation whilst placebo treatment fosters it. This implication is supported by leading neuroscientists who recently called for a systematic investigation of self-regulatory factors to psychologically better understand placebo effects (Benedetti, Mayberg, Wager, Stohler, and Zubieta, 2006). Given that placebo caffeine research also found bodily and mental changes when no caffeine was administered, the effects found for caffeinated substances at least in part may bear on such underlying mechanisms. This would explain the somewhat opposing effects found for caffeine: whether a strong cup of coffee exerts an effect on, for instance, cognitive performance, would be mediated by the psychosocial context in which it is consumed and the expectation and meaning which are associated with it. Clearly, the relationship between caffeine and placebo caffeine effects may assume different forms. For example, the psychological mechanisms may supersede or counter-regulate the pharmacologic effects (Fillmore and Blachburne, 2002; Schneider et al., 2006), be neglectable when no expectations are associated with the caffeinated beverage (James, 1998)
or be additive when specific and unspecific effects are stressed (Flaten and Blumenthal, 1999).
One corollary derived from PSI Theory is that subsymbolic mechanisms are associated
with the placebo effect because expectations and cognitions involved are not fully conscious. Bearing on the findings from hemispheric activation stimulation to activate extension memory (Baumann, Kuhl, and Kazén, 2005) contiguously activating the extension memory, for example, by squeezing a soft ball with the counterlateral hand, upon intake of placebo should ensue much stronger placebo effects. Likewise, since extension memory affords complex cognitive processes, for example the detection of semantic coherences (Baumann and Kuhl, 2002; Bolte, Goschke, and Kuhl, 2003), placebo caffeine effects would comprise coherence perception whilst caffeine effects, which primarily affect relatively simple cognitive processes (Lorist and Topsa, 2003; Ruijter et al., 2000), would not. Hence, when studying (placebo) caffeine effects implicit coherence performance would be enhanced in individuals expecting caffeine to improve coherence perception. Furthermore, if the activation of extension memory is constitutive for the placebo effect, there should be correlations with self-regulatory mechanisms (e.g., affect regulation). This, in turn, would make placebo effects predictable by self-regulatory mechanisms, which, according to PSI theory, are exerted effortlessly and implicitly. Such a relationship should not hold for pharmacological effects because they are, to a much lesser degree, mediated by psychological mechanisms (i.e. self-relevant expectations).
Following this line of reasoning, I suggest the following definition for placebo effects including functional psychological boundary conditions. Placebo effects are unspecific intervention effects depending on the individulal’s implicit competency to construe meaning in the psychosocial context, and to respond to this meaning by means of self-regulation. Conclusion
The effects caffeine exerts on health cannot be reduced to pharmacological pathways but
comprise psychological mechanisms also. The findings on placebo caffeine effects suggest that so called unspecific effects substantially contribute to caffeine effects. The mind in fact may overrule the body when specific expectations with a certain meaning are held. Whether psychological factors exert a significant influence over and above pharmacologic effects is determined by the context in which caffeine is ingested. Disentangling the mediating role of self-regulatory factors in caffeine effects may benefit the understanding of when and how health effects may be expected. To do so, traditional ways of testing caffeine (e.g., employing RCTs) should be complemented with those which allow testing of caffeine and placebo under different conditions (extended balanced placebo design). To better understand psychological factors, functional approaches and methods should be employed (e.g., PSI theory and the diagnostic tools derived from it). Although from a pragmatic point of view a separation of specific and unspecific effects is not necessary (in most cases even disadvantageous),
Unspecific Effects of Caffeine Consumption
understanding the underlying mechanisms and boundary conditions of the context is important in determining health-related caffeine effects.
References
Ader, R. (1993). Conditioned responses in pharmacotherapy research. Psychological
Amanzio, M. and Benedetti, F. (1999). Neuropharmacological dissection of placebo
analgesia: Expectation-activated opioid systems versus conditioning-activated specific subsystems. Journal of Neuroscience, 19, 484-494.
American Gastroenterological Association (2005). Coffee and tea can reduce the risk of
chronic liver disease. http://www.gastro.org/wmspage.cfm?parm1=1833 [Online].
Anderson, C., and Horne, J. A. (in press). Placebo response to caffeine improves reaction
time performance in sleepy people. Human Psychopharmacology: Clinical and Experimental. Baumann, N., Kuhl, J., and Kazén, M. (2005). Left-hemispheric activation and self-
infiltration: Testing a neuropsychological model of internalization. Motivation and Emotion, 29, 135-163.
Baumann, N. and Kuhl, J. (2002). Intuition, affect, and personality: Unconscious coherence
judgments and self-regulation of negative affect. Journal of Personality and Social Psychology, 83, 1213-1223.
Beecher, H. K. (1955). The powerful placebo. Journal of the American Medical Association,
Beeman, M. J., Friedman, R. B., Perez, E., Diamond, S., and Lindsay, M. B. (1994).
Summation priming and coarse coding in the right hemisphere. Journal of Cognitive Neuroscience, 6, 26-45.
Beeman, M. J. and Bowden, E. M. (2000). The right hemisphere maintains solution-related
activation for yet-to-be solved problems. Memory and Cognition, 28, 1231-1241.
Benedetti, F. (2006). Placebo analgesia. Neurological Sciences, 27, S100-S102. Benedetti, F., Mayberg, H. S., Wager, T. D., Stohler, C. S., and Zubieta, J.-K. (2006).
Neurobiological mechanisms of the placebo effect. Journal of Neuroscience, 25, 10390-10402.
Biller-Andorno, N. (2004). The use of the placebo effect in clinical medicine - ethical blunder
or ethical imperative? Science and Engineering Ethics, 10, 43-50.
British Medical Journal (1998). The randomised controlled trial at 50. British Medical
Bolte, A., Goschke, T., and Kuhl, J. (2003). Emotions and intuition: Effects of positive and
negative mood on implicit judgments of semantic coherence. Psychological Science, 14, 416-421.
Borod, J. C., and Madigan, N. K. (2000). Neuropsychology of emotion and emotional
disorder: An overview and research directions. In J. C. Borod (Ed.), The neuropsychology of emotion (pp. 3-28). New York: Oxford University Press.
Bowden, E. M. and Beeman, M. J. (1998). Getting the right idea: Semantic activation in the
right hemisphere. Psychological Science, 9, 435-440.
Bowers, K. S., Regehr, G., Balthazard, C., and Parker, K. (1990). Intuition in the context of
discovery. Cognitive Psychology, 22, 72-110.
Colloca, L. and Benedetti, F. (2006). How prior experience shapes placebo analgesia. Pain,
Craik, F. I. M., Moroz, T. M., Moscovitch, M., Stuss, D. T., Wincour, G., Tulving, E. et al.
(1999). In search of the self: A positron emission tomography study. Psychological Science, 10, 26-34.
Dinnerstein, A. L. and Halm, J. (1970). Modification of placebo effects by means of drugs:
Effects of aspirin and placebos on self-related moods. Journal of Abnormal Psychology, 75, 303-314.
Ernst, E. and Resch, K. L. (2003). Concept of true and perceived placebo effects. British
Fillmore, M., Mulvihill, L. E., and Vogel-Sprott, M. (1994). The expected drug and its
expected effect interact to determine placebo responses to alcohol and caffeine. Psychopharmacology, 115, 383-388.
Fillmore, M., Roach, E., and Rice, J. (2002). Does caffeine counteract alcohol-induced
impairment? The ironic effects of expectancy. Journal of Studies on Alcohol, 63, 745-754.
Fillmore, M. and Vogel-Sprott, M. (1992). Expected effect of caffeine on motor performance
predicts the type of response to placebo. Psychopharmacology, 106, 209-214.
Flaten, M. A. and Blumenthal, T. D. (1999). Caffeine-associated stimuli elicit conditioned
responses: An experimental model of the placebo effect. Psychopharmacology, 145, 105-112.
Fredholm, B. B., Bättig, K., Holmén, J., Nehlig, A., and Zvartau, E. E. (1999). Actions of
caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacological Reviews, 51, 83-133.
Fuster, J. M. (2000). Executive frontal functions. Experimental Brain Research, 133, 66-70. Garavan, H., Ross, T. J., and Stein, E. A. (1999). Right hemispheric dominance of inhibitory
control: An event-related functional FMRI study. Proceedings of the National Academy of Sciences USA, 96, 8301-8306.
Hróbjartsson, A. and Gøtzsche, P. C. (2004). Is the placebo powerless? Update of a
systematic review with 52 new randomized trials comparing placebo with no treatment. Journal of Internal Medicine, 256, 91-100.
James, J. E. (1994). Does caffeine enhance or merely restore degraded psychomotor
performance? Neuropsychobiology, 30, 124-125.
James, J. E. (1998). Acute and chronic effects of caffeine on performance, mood, headache,
and sleep. Neuropsychobiology, 38, 32-41.
James, J. E. and Gregg, M. E. (2004). Effects of dietary caffeine on mood when rested and
sleep restricted. Human Psychopharmacology: Clinical and Experimental, 19, 333-341.
James, J. E., Gregg, M. E., Kane, M., and Harte, F. (2005). Dietary caffeine, performance and
mood: Enhancing and restorative effects after controlling for withdrawal reversal. Neuropsychology, 52, 1-10.
Unspecific Effects of Caffeine Consumption
Juliano, L. M., and Brandon, T. H. (2002). Effects of nicotine dose, instructional set, and
outcome expectancies on the subjective effects of smoking in the presence of a
stressor. Journal of Abnormal Psychology,111, 88-97. Kapur, S., Craik, F. I. M., Jones, C., Brown, G. M., Houle, S., and Tulving, E. (1995).
Functional role of the prefrontal cortex in retrieval of memories: A PET study. NeuroReport, 6, 1880-1884.
Keenan, J. P., Nelson, A., O'Connor, M., and Pascual-Leone, A. (2001). Self-recognition and
the right hemisphere. Nature, 409, 305.
Kienle, G. S. and Kiene, H. (1997). The powerful placebo effect: Fact or fiction? Journal of Clinical Epidemiology, 50, 1311-1318.
Kirsch, I. (1999). How expectancies shape experience. Washington, DC: American
Kirsch, I., Scoboria, A., and Moore, T. J. (2002). Antidepressants and placebos: secrets,
revelations, and unanswered questions. Prevention and Treatment [Online]. Available: http://www.journals.apa.org/prevention/volume5/pre0050033r.html.
Kirsch, I., and Sapirstein, G. (1999). Listening to Prozac but hearing placebo: A meta-
analysis of antidepressant medications. In: I. Kirsch (Ed.). How expectancies shape experience (pp. 303-320), Washington, DC: American Psychological Association.
Kirsch, I. and Weixel, L. J. (1988). Double-blind versus deceptive administration of a
placebo. Behavioral Neuroscience, 102, 319-323.
Koch, C. and Laurent, G. (1999). Complexity and the nervous system. Science, 284, 96-98. Kuhl, J. (2000). A functional-design approach to motivation and self-regulation: The
dynamics of personality systems interaction. In M. Boekaerts, P. R. Pintrich, and M. Zeidner (Eds.), Handbook of self-regulation (pp. 111-169). New York: Academic Press.
Kuhl, J. (2001). Motivation und Persönlichkeit. Interaktionen psychischer Systeme.
Kuhl, J. and Kazén, M. (1994). Self-discrimination and memory: State orientation and false
self-ascription of assigned activities. Journal of Personality and Social Psychology, 66, 1103-1115.
Lee, S., Walker, J. R., Jakul, L., and Sexton, K. (2004). Does elimination of placebo
responders in a placebo run-in increase the treatment effect in randomized clinical trials? A meta-analytical evaluation. Depression and Anxiety, 19, 10-19.
Lorist, M. M. and Topsa, M. (2003). Caffeine, fatigue, and cognition. Brain and Cognition,
Lyerly, S. B., Krugman, A. D., and Clyde, D. J. (1964). Drugs and placebos: The effects of
instructions upon performance and mood under amphetamine sulphate and chloral hydrate. Journal of Abnormal and Social Psychology, 68, 321-327.
Marlatt, G. A. and Rohsenow, D. J. (1980). Cognitive processes in alcohol use: Expectancy
and the balanced placebo design. In N. Mello (Ed.), Advances in Substance Abuse (pp. 159-199). Greenwich: JAI Press.
McClelland, D. C., Koestner, R., and Weinberger, J. (1989). How do self-attributed and
implicit motives differ? Psychological Review, 96, 690-702.
Mikalsen, A., Bertelsen, B., and Flaten, M. A. (2001). Effects of caffeine, caffeine-associated
stimuli, and caffeine-related information on physiological and psychological arousal. Psychopharmacology, 157, 373-380.
Moerman, D. E. and Jonas, W. B. (2002). Deconstructing the placebo effect and finding the
meaning response. Annals of Internal Medicine, 136, 471-476.
Nadel, L. and Moscovitch, M. (1997). Memory consolidation, retrograde amnesia and the
hippocampal complex. Current Opinion in Neurobiology, 7, 217-227.
Nyberg, L., Cabeza, R., and Tulving, E. (1996). PET studies of encoding and retrieval: The
HERA model. Psychonomic Bulletin and Review, 3, 135-148.
Perkins, K. A., Jacobs, L., Ciccocioppo, M., Conklin, C. A., Sayette, M., and Caggiula, A.
(2004). The influence of instructions and nicotine dose on the subjective and reinforcing effects of smoking. Experimental and Clinical Psychopharmacology, 12, 91-101. Perkins, K. A., Ciccocioppo, M., Conklin, C. A., Milanak, M. E., Grottenthaler, A., and Sayette, M. (2008). Mood influences on acute smoking responses are independent of nicotine intake and dose expectancy. Journal of Abnormal Psychology, 117, 79-93.
Pacheco-Lopez ,G., Engler, H., Niemi, M.-B., and Schedlowski, M. (2006). Expectations and
associations that heal: Immunomodulatory placebo effects and its neurobiology. Brain, Behavior, and Immunity, 20, 430-446.
Phillips-Bute, B. G. and Lane, J. D. (1998). Caffeine withdrawal symptoms following brief
caffeine deprivation. Physiology and Behavior, 63, 35-39.
Pollo, A., Vighetti, S., Rainero, I., and Benedetti, F. (2003). Placebo analgesia and the heart.
Quirin, M., Kazén, M., Rohrmann, S., and Kuhl, J. (in press).
Quirin, M., Koole, S. L., Baumann, N., Kazén, M., and Kuhl, J. (2007). You can't always
remember what you want: The role of cortisol in self-ascription of assigned goals. Submitted manuscript.
Rogers, P. J., Martin, J., Smith, C., Heatherley, S. V., and Smit, H. J. (2003). Absence of
reinforcing, mood and psychomotor performance effects of caffeine in habitual non-consumers of caffeine. Psychopharmacology, 167, 54-62.
Rotenberg, V. S. (2004). The peculiarity of the right-hemisphere function in depression:
Solving the paradoxes. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 28, 1-13.
Rotenberg, V. S. and Weinberg, I. (1999). Human memory, cerebral hemispheres, and the
limbic system: A new approach. Genetic, Social, and General Psychology Monographs, 125, 526-532.
Ruijter, J., De Ruiter, M., Snel, J., and Lorist, M. M. (2000). The influence of caffeine on
spatial-selective attention: an event-related potential study. Clinical Neurophysiology, 111, 2223-2233.
Ruijter, J., Lorist, M. M., and Snel, J. (1999). The influence of different doses of caffeine on
visual task performance. Journal of Psychophysiology, 13, 37-48.
Ruijter, J., Lorist, M. M., and Snel, J. (2000). The effects of caffeine on visual selective
attention to color: An ERP study. Psychophysiology, 37, 427-439.
Ruijter, J., Lorist, M. M., Snel, J., and Ruiter, M. B. (2000). The influence of caffeine on
sustained attention: An ERP study. Pharmacology, Biochemistry and Behaviour, 6, 29-37.
Unspecific Effects of Caffeine Consumption
Rumelhart, D. E. and McClelland, J. L. (1986). Parallel distributed processing: Explorations in the microstructure of cognition. Cambridge, MA: MIT Press.
Sauro, M. D. and Greenberg, R. P. (2005). Endogenous opiates and the placebo effect. A
meta-analytic review. Journal of Psychosomatic Research, 58, 115-120.
Scheibel, A. B., Freid, I., Paul, L., Forsythe, A., Tomiyasu, U., Wechsler, A. et al. (1985).
Differentiating characteristics of the human speech cortex: A quantitative Golgi study. In D. F. Benson and E. Zaidel (Eds.), The dual brain. New York: Guilford Press.
Schneider, R. (2007). The psychology of the placebo effect: Exploring meaning from a
functional account. Journal of Mind and Behavior, 18, 1-17.
Schneider, R. and Walach, H. (in preparation). Classical and non-classical placebo effect:
Schneider, R., Grüner, M., Heiland, A., Keller, M., Kujanová, Z., Peper, M. et al. (2006).
Effects of expectation and caffeine on arousal, well-being, and reaction time. International Journal of Behavioral Medicine, 13, 330-339.
Smit, H. J. and Rogers, P. J. (2000). Effects of low doses of caffeine on cognitive
performance, mood and thirst in low and higher caffeine consumers. Psychopharmacology, 152, 167-173.
Smith, A., Sutherland, D., and Christopher, G. (2005). Effects of repeated doses of caffeine
on mood and performance of alert and fatigued volunteers. Journal of Pharmacology, 19, 620-626.
Stolk, P., ten Berg, M. J., Hemels, M. E. H., and Einarson, T. R. (2003). Meta-analysis of
placebo rates in major depressive disorder trials. The Annals of Psychotherapy, 37, 1891-1899.
Svenningsson, P., Nomikos, G. G., Ongini, E., and Fredholm, B. B. (1997). Antagonism of
adenosine A2A receptors underlies the behavioural activating effect of caffeine and is associated with reduced expression of messenger RNA for NGFI-A and NGFI-B in caudate-putamen and nucleus accumbens. Neuroscience, 79, 753-764.
ter Riet, G., de Craen, A. J. M., de Boer, A., and Kessels, A. G. H. (1998). Is placebo
analgesia mediated by endogenous opioids? A systematic review. Pain, 76, 273-275.
Thase, M. E. (1999). Randomized clinical trials of treatments for depression? Journal of
Turner, J. A., Deyo, R. A., Loeser, J. D., von Korff, M., and Fordyce, W. E. (1994). The
importance of placebo effects in pain treatment and research. Journal of the American Medical Association, 271, 1609-1614.
Turner, J. A., Jensen, M. P., Warms, C. A., and Cardenas, D. D. (2002). Blinding
effectiveness and association of pretreatment expectations with pain improvement in a double-blind randomized controlled trial. Pain, 99, 91-99.
Ungerleider, L. G. and Mishkin, M. (1982). Two visual systems. In D. J .Ingle, M. A.
Goodale, and R. J. W. Mansfield (Eds.), Analysis of visual behavior (pp. 549-586). Cambridge, MA: MIT Press.
Vase, L., Riley, J. L., and Price, D. D. (2002). A comparison of placebo effects in clinical
analgesic trials versus studies of placebo analgesia. Pain, 99, 443-452.
Vase, L., Robinson, M. E., and Price, D. D. (2005). Increased placebo analgesia over time in
irritable bowel syndrome (IBS) patients is associated with desire and expectation but endogenous opioid mechanisms. Pain, 115, 338-347.
Vase, L., Robinson, M. E., Verne, G. N., and Price, D. D. (2003). The contributions of
suggestion, desire, and expectation to placebo effects in irritable bowel syndrome patients. An empirical investigation. Pain, 105, 17-25.
Wager, T. D., Rilling, J.K., Smith, E.E., Sokolik, A., Casey, K. L., et al. (2004). Placebo-
induced changes in fMRI in the anticipation and experience of pain. Science, 303, 1162-1167.
Wager, T. D. (2005). The neural bases of placebo effects in anticipation and pain. Seminars
Walach, H., Schmidt, S., Bihr, Y.-M., and Wiesch, S. (2001). The effects of a caffeine
placebo and experimenter expectation on blood pressure, heart rate, well-being, and cognitive performance. European Psychologist, 6, 15-25.
Walach, H., Schmidt, S., Dirhold, T., and Nosch, S. (2002). The effects of a caffeine placebo
and suggestion on blood pressure, heart rate, well-being and cognitive performance. International Journal of Psychophysiology, 43, 247-260.
Wheeler, M. A., Stuss, D. T., and Tulving, E. (1997). Toward a theory of episodic memory:
The frontal lobes and autonoetic consciousness. Psychological Bulletin, 121, 331-354.
Wickrameskera, I. (1980). A conditioned response model of the placebo effect: Predictions
from the model. Biofeedback and Self Regulation, 5, 5-18.
Yeomans, M. R., Ripley, T., Davies, L. H., Rusted, J. M., and Rogers, P. J. (2002). Effects of
caffeine on performance and mood depend on the level of caffeine abstinence. Psychopharmacology, 164, 241-249.
Zubieta, J.-K., Yau, W. Y., Scott, D. J., and Stohler, C. S. (2006). Belief or need? Accounting
for individual varitions in the neurochemistry of the placebo effect. Brain, Behavior, and Immunity, 20, 15-26.
Page 1 of 3 WARFARIN Why is this medication prescribed? Warfarin is used to prevent blood clots (thrombosis) from forming or growing larger in the arteries or veins. Warfarin has an anticoagulant effect on the blood. It slows down the clotting process helping to prevent thrombosis from occurring or reoccurring. Blood clots can lead to stroke, heart attack o
 Unspecific Effects of Caffeine Consumption
Figure 1. The caffeine placebo effect as a result of conditioned learning.
It should be noted that both approaches are not necessarily mutually exclusive. In fact,
they are often synergistic. Unfortunately, unlike other placebo effect phenomena, the neurobiological mechanisms of the caffeine placebo effect have not yet been subjected to investigation. Placebo analgesia, for example, has been found to be maximal when expectation and conditioning are combined (Amanzio and Benedetti, 1999; Colloca and Benedetti, 2006). Yet, expectancy effects have shown to be associated with a different neurological pathway than conditioning effects: Placebo analgesic effects bearing on expectation can be blocked with the opioid antagonist naloxone. Placebo effects brought about by a conditioned treatment (i.e. the injection) with a non-steroid anti-inflammatory drug (ketorolac), have a different pathway because they can’t be inhibited. Furthermore, a number of several studies have demonstrated that placebo effects involve different brain areas than pharmacologic effects. These involve subcortical processes (e.g., in pain sensitive neuroanatomical areas via opioid release) and cortical ones (via cognitive appraisal), with the latter occurring after some latency and mostly affecting pain experience (Wager, et. al, 2004; Wager, 2005). Similar findings on the mediating role of the prefrontal cortex in placebo effects have been reported on a broad range of symptoms like depression, irritable bowl syndrome, or chronic pain (cf. Pacheco-Lopez, Engler, Niemi, and Schedlowski, 2006; Schneider, 2007) Consequently, when expectations are engaged, the prefrontal cortex, which maintains evaluative information for control and self-knowledge (Craik et al., 1999; Fuster, 2000), exerts a top-down control modulating experience and physiological processes. It is important to note that expectations need not necessarily be conscious in order to exert a placebo effect (Turner, Jensen, Warms, and Cardenas, 2002). As shown above, from the many effects observed for caffeine ingestion, it may be assumed that in addition to the specific (pharmacologic) effects of caffeine, unspecific (psychological) mechanisms exert an influential role over and above specific ones. This requires a somewhat different methodological approach to fully understand the impact of caffeine on health.
4. Methodological Approaches
Unspecific Effects of Caffeine Consumption
Figure 1. The caffeine placebo effect as a result of conditioned learning.
It should be noted that both approaches are not necessarily mutually exclusive. In fact,
they are often synergistic. Unfortunately, unlike other placebo effect phenomena, the neurobiological mechanisms of the caffeine placebo effect have not yet been subjected to investigation. Placebo analgesia, for example, has been found to be maximal when expectation and conditioning are combined (Amanzio and Benedetti, 1999; Colloca and Benedetti, 2006). Yet, expectancy effects have shown to be associated with a different neurological pathway than conditioning effects: Placebo analgesic effects bearing on expectation can be blocked with the opioid antagonist naloxone. Placebo effects brought about by a conditioned treatment (i.e. the injection) with a non-steroid anti-inflammatory drug (ketorolac), have a different pathway because they can’t be inhibited. Furthermore, a number of several studies have demonstrated that placebo effects involve different brain areas than pharmacologic effects. These involve subcortical processes (e.g., in pain sensitive neuroanatomical areas via opioid release) and cortical ones (via cognitive appraisal), with the latter occurring after some latency and mostly affecting pain experience (Wager, et. al, 2004; Wager, 2005). Similar findings on the mediating role of the prefrontal cortex in placebo effects have been reported on a broad range of symptoms like depression, irritable bowl syndrome, or chronic pain (cf. Pacheco-Lopez, Engler, Niemi, and Schedlowski, 2006; Schneider, 2007) Consequently, when expectations are engaged, the prefrontal cortex, which maintains evaluative information for control and self-knowledge (Craik et al., 1999; Fuster, 2000), exerts a top-down control modulating experience and physiological processes. It is important to note that expectations need not necessarily be conscious in order to exert a placebo effect (Turner, Jensen, Warms, and Cardenas, 2002). As shown above, from the many effects observed for caffeine ingestion, it may be assumed that in addition to the specific (pharmacologic) effects of caffeine, unspecific (psychological) mechanisms exert an influential role over and above specific ones. This requires a somewhat different methodological approach to fully understand the impact of caffeine on health.
4. Methodological Approaches 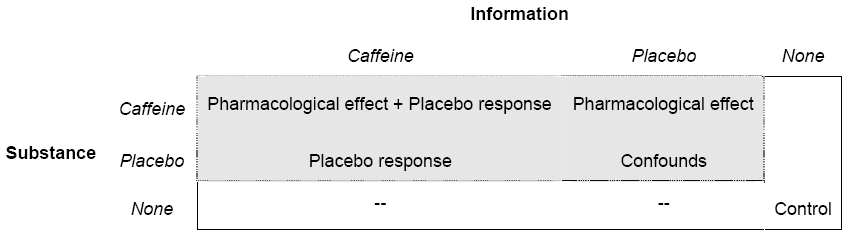 proportion of the placebo effect can be determined when open and hidden administrations are compared. Although this is a straightforward methodology, it may be questioned whether its ecological validity is sound. For example, to determine bio-availability, absorption rate and pharmacodynamics of caffeine, hidden administration of the agent is likely to have different effects than oral ingestion. Therefore, to study the effects of caffeine under real life conditions this experimental paradigm is not viable.
Another way of studying pharmacologic and psychological factors of caffeine
consumption is suggested by the so called balanced placebo design (Marlatt and Rohsenow, 1980). It combines the usual placebo design with an “antiplacebo” design resulting in a 2(drug, placebo) x 2(expectation, no expectation) arrangement. By administering placebo and drug under conditions in which the participants expect to receive an inert substance, independent effects of psychological and pharmacologic effects can be parceled out. As can be seen in Figure 2 (dotted line), a “true” pharmacologic effect would be obtained in an experimental condition were participants are given caffeine but are told to have received placebo.
Figure 2. The extended balanced placebo design; Placebo effect: Placebo response minus control.
Likewise, when placebo is given but participants are told they ingested caffeine, placebo
responses are discernable. It is, however, important to note that the balanced placebo design is only able to unravel placebo responses but not placebo effects. This is because placebo responses comprise both placebo effects and confounds like artifacts, spontaneous remission, regression effects and the like (Ernst and Resch, 2003; Kirsch and Sapirstein, 1999). Hence, to determine placebo effects the balanced placebo design must be “extended” by including a zero control group with which placebo responses are compared (solid line).
The balanced placebo design has been primarily used in alcohol research with
expectancy effects comparable to drug effects (for an overview see Marlatt and Rohsenow, 1980). Since then, it has only seldom been fully employed and somewhat fell into oblivion (for a few exceptions, cf. Juliano and Brandon, 2002; Perkins et al., 2004; Perkins et al., 2008). In placebo caffeine research, this is partly due to the fact that placebo response effects showed as main effects having subsequent researchers focus on comparisons of placebo and control group.
Research on the effects of caffeine on health would benefit greatly from employing the
extended balanced placebo design to study the relationship between specific and unspecific effects. However, to understand unspecific effects from a psychological point of view, it may not suffice to primarily focus on conscious thought contents in determining expectations or
Unspecific Effects of Caffeine Consumption
meaning. This is because people only have limited access to mental processes and cannot fully or adequately explicate (verbalize) them. This is suggested by neurobiological findings showing implicit and parallel-holistic processes of the brain (Beeman, Friedman, Perez, Diamond, and Lindsay, 1994; Beeman and Bowden, 2000; Bowden and Beeman, 1998; Bowers, Regehr, Balthazard, and Parker, 1990; Rumelhart and McClelland, 1986) and that these processes also comprise functional properties like self-regulation, motivation, or affect (Craik et al., 1999; Keenan, Nelson, O'Connor, and Pascual-Leone, 2001; Nadel and Moscovitch, 1997; Quirin, Kazén, Rohrmann, and Kuhl, in press; Quirin, Koole, Baumann, Kazén, and Kuhl, 2007; Rotenberg and Weinberg, 1999; Wheeler, Stuss, and Tulving, 1997). Thus, in placebo research, simply asking people about their cognitions may not suffice when meaning and expectations are assessed. Yet, functional approaches, uncovering subsystems describable in terms of classes of functions, have not been employed in placebo research. In the following, a functionally oriented theory is introduced according to which psychologically important subsystems can be evaluated for their significance of placebo effects.
5. Dynamics of Psychological Functions:
proportion of the placebo effect can be determined when open and hidden administrations are compared. Although this is a straightforward methodology, it may be questioned whether its ecological validity is sound. For example, to determine bio-availability, absorption rate and pharmacodynamics of caffeine, hidden administration of the agent is likely to have different effects than oral ingestion. Therefore, to study the effects of caffeine under real life conditions this experimental paradigm is not viable.
Another way of studying pharmacologic and psychological factors of caffeine
consumption is suggested by the so called balanced placebo design (Marlatt and Rohsenow, 1980). It combines the usual placebo design with an “antiplacebo” design resulting in a 2(drug, placebo) x 2(expectation, no expectation) arrangement. By administering placebo and drug under conditions in which the participants expect to receive an inert substance, independent effects of psychological and pharmacologic effects can be parceled out. As can be seen in Figure 2 (dotted line), a “true” pharmacologic effect would be obtained in an experimental condition were participants are given caffeine but are told to have received placebo.
Figure 2. The extended balanced placebo design; Placebo effect: Placebo response minus control.
Likewise, when placebo is given but participants are told they ingested caffeine, placebo
responses are discernable. It is, however, important to note that the balanced placebo design is only able to unravel placebo responses but not placebo effects. This is because placebo responses comprise both placebo effects and confounds like artifacts, spontaneous remission, regression effects and the like (Ernst and Resch, 2003; Kirsch and Sapirstein, 1999). Hence, to determine placebo effects the balanced placebo design must be “extended” by including a zero control group with which placebo responses are compared (solid line).
The balanced placebo design has been primarily used in alcohol research with
expectancy effects comparable to drug effects (for an overview see Marlatt and Rohsenow, 1980). Since then, it has only seldom been fully employed and somewhat fell into oblivion (for a few exceptions, cf. Juliano and Brandon, 2002; Perkins et al., 2004; Perkins et al., 2008). In placebo caffeine research, this is partly due to the fact that placebo response effects showed as main effects having subsequent researchers focus on comparisons of placebo and control group.
Research on the effects of caffeine on health would benefit greatly from employing the
extended balanced placebo design to study the relationship between specific and unspecific effects. However, to understand unspecific effects from a psychological point of view, it may not suffice to primarily focus on conscious thought contents in determining expectations or
Unspecific Effects of Caffeine Consumption
meaning. This is because people only have limited access to mental processes and cannot fully or adequately explicate (verbalize) them. This is suggested by neurobiological findings showing implicit and parallel-holistic processes of the brain (Beeman, Friedman, Perez, Diamond, and Lindsay, 1994; Beeman and Bowden, 2000; Bowden and Beeman, 1998; Bowers, Regehr, Balthazard, and Parker, 1990; Rumelhart and McClelland, 1986) and that these processes also comprise functional properties like self-regulation, motivation, or affect (Craik et al., 1999; Keenan, Nelson, O'Connor, and Pascual-Leone, 2001; Nadel and Moscovitch, 1997; Quirin, Kazén, Rohrmann, and Kuhl, in press; Quirin, Koole, Baumann, Kazén, and Kuhl, 2007; Rotenberg and Weinberg, 1999; Wheeler, Stuss, and Tulving, 1997). Thus, in placebo research, simply asking people about their cognitions may not suffice when meaning and expectations are assessed. Yet, functional approaches, uncovering subsystems describable in terms of classes of functions, have not been employed in placebo research. In the following, a functionally oriented theory is introduced according to which psychologically important subsystems can be evaluated for their significance of placebo effects.
5. Dynamics of Psychological Functions: 



 Cabeza, and Tulving, 1996; Wheeler et al., 1997). Moreover, functions of extension memory also encompass attention processes (vigilance) and enhance those perceptual contents which match actual relevant and implicit networks of needs, expectations, and other self-structures. Due to this characteristic, processes of extension memory are not fully conscious. One of the typical functions of extension memory is down-regulation of negative affect elicited by aversive, threatening or unpredictable experiences because extension memory is tightly linked with vegetative and somatosensory processes (Borod and Madigan, 2000; Garavan, Ross, and Stein, 1999; Kapur et al., 1995; Rotenberg, 2004). This is shown as self-relaxation in Figure 3.
Left Hemisphere
Cabeza, and Tulving, 1996; Wheeler et al., 1997). Moreover, functions of extension memory also encompass attention processes (vigilance) and enhance those perceptual contents which match actual relevant and implicit networks of needs, expectations, and other self-structures. Due to this characteristic, processes of extension memory are not fully conscious. One of the typical functions of extension memory is down-regulation of negative affect elicited by aversive, threatening or unpredictable experiences because extension memory is tightly linked with vegetative and somatosensory processes (Borod and Madigan, 2000; Garavan, Ross, and Stein, 1999; Kapur et al., 1995; Rotenberg, 2004). This is shown as self-relaxation in Figure 3.
Left Hemisphere