Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Pii: s0360-3016(99)00063-2
Int. J. Radiation Oncology Biol. Phys., Vol. 44, No. 3, pp. 569 –577, 1999
Copyright 1999 Elsevier Science Inc. PII S0360-3016(99)00063-2 RADIATION THERAPY FOR CONSOLIDATION OF METASTATIC OR RECURRENT SARCOMAS IN CHILDREN TREATED WITH INTENSIVE CHEMOTHERAPY AND STEM CELL RESCUE. A FEASIBILITY STUDY
E. ANN DUNPHY CZYZEWSKI, M.D.,* STEWART GOLDMAN, M.D.,† ARNO J. MUNDT, M.D.,‡
JAMES NACHMAN, M.D.,† CHARLES RUBIN, M.D.,† AND DENNIS E. HALLAHAN, M.D.§
*Department of Cancer Biology, University of Chicago, Chicago, IL; †Department of Pediatric Hematology/Oncology, University of
Chicago, Chicago, IL; ‡Department of Radiation and Cellular Oncology, University of Chicago,Chicago, IL; and §Vanderbilt University
Purpose: To assess the role of consolidative radiation therapy (CRT) in conjunction with myeloablative therapy with or without total body irradiation (TBI) in children and young adults with metastatic or recurrent sarcoma. Methods and Materials: Twenty-one pediatric sarcoma patients with metastatic (10) or recurrent (11) disease were entered on a prospective feasibility study of intensive myeloablative therapy with or without TBI. Median patient age was 17.8 years (range, 9.4 –24.7 years). Primary histologies included Ewing’s (12), PNET (3), and other soft tissue sarcomas (6). Twenty patients received induction chemotherapy. Myeloablative therapy con- sisted of TBI in 11 patients with either high dose melphalan/etoposide (9) or high dose cytoxan/thiotepa (2). TBI consisted of 12 Gy in 2 Gy fractions delivered twice daily over 3 days. Ten patients received high dose chemotherapy alone, either with thiotepa/carboplatinum/etoposide (8) or cytoxan/carboplatinum (2). Myeloab- lative therapy was followed by autologous stem cell rescue (ASCR) 24 to 48 hours after completing chemother- apy. Fourteen patients (67%) received CRT either prior to (5) or following (9) myeloablative therapy. Median CRT dose was 37.2 Gy (range, 20 – 60). Fifty-one disease sites were present prior to myeloablative therapy. Twelve (24%) were bulky (> 8 cm) and 18 (35%) underwent surgical debulking. The median follow-up of surviving patients was 15 months (range, 8 –20) with 25% of patients having been followed for more than 20 months. Results: The 3-year actuarial disease-free (DFS) and overall survival (OS) rates for the entire group were 36% and 27%, respectively. Following myeloablative treatment, responses were: 11 complete, 6 partial, 1 stable, and 3 progressive disease. Sixteen patients (71%) have relapsed. The most common site of relapse was the lung (13). Of the 51 disease sites present prior to myeloablative therapy, 36 sites (71%) were amenable to CRT. Non- amenable sites were: multiple lung metastases (13) and bone marrow (2). Twenty-six amenable sites (51%) received CRT either prior to (14) or following (12) ASCR. Amenable sites treated with CRT had a better 3-year actuarial local control (80 vs 37%) (p ؍ 0.0065) than amenable sites not treated with CRT. Factors associated with improved disease-free survival (DFS) in univariate analysis were induction chemotherapy response (p ؍ 0.002) and extent of surgical resection (p ؍ 0.045). There was a trend toward improved DFS on univariate analysis with the use of TBI as part of myeloablative therapy (p ؍ 0.07). The one factor associated with improved OS on univariate analysis was induction chemotherapy response (p ؍ 0.007). Multivariate analysis revealed that induction chemotherapy response is the only factor that remains significant for DFS (p ؍ 0.032) as well as for OS (p ؍ 0.017). Patients with complete response to induction therapy had 40% probability of survival versus all other patients who had 10% survival (p ؍ 0.05). Conclusion: Consolidative radiotherapy is feasible in primary metastatic or recurrent pediatric sarcoma patients treated with myeloablative therapy with or without TBI. CRT to sites amenable to irradiation provided an improved 3-year actuarial local control than that seen in sites amenable to CRT that did not undergo radiotherapy. There was a trend for improved DFS with the use of TBI. Improved DFS and OS can be predicted by response to induction therapy. This intensive regimen may improve the cure rate of advanced pediatric sarcomas in select patients. 1999 Elsevier Science Inc. Sarcoma, Autologous bone marrow transplant, Radiation therapy.
Reprint requests to: Dennis Hallahan, M.D., Chairman, Depart-
Lane, Ann Hosewitz, Sharon Bolster, RN, for data management
ment of Radiation Oncology, 1301 22nd Avenue South, B-902,
Vanderbilt Clinic, Nashville, TN 37232-5671. Tel 615-343-9244;
Accepted for publication 2 February 1999.
Fax 615-343-3075; Email: [email protected].
Presented at the 40th Annual Meeting of the American Society
for Therapeutic Radiology and Oncology, Phoenix, AZ, October,
Acknowledgments—We thank Carmalita Chotipradit, RN, Debra
I. J. Radiation Oncology ● Biology ● Physics
INTRODUCTION
chemotherapy response. In addition, 13 patients had lungmetastases on initial presentation. Despite this, the 3-year
Large single or multi-institution studies for high-risk or
DFS was 36% and OS was 27%, comparable to the outcome
metastatic Ewing’s sarcoma report 3-year event-free surviv-
of large prospective, randomized trials reported in the liter-
als of approximately 30% whether treated with myeloabla-
ature. The presence of bulky disease did not have an impact
tive regimens (1– 4) or conventional multimodality therapy
on local control. This may be due to the use of CRT for
(4 – 6). Similar poor results have been reported for meta-
amenable sites, which was found to have a significant im-
static peripheral primitive neuroectodermal (PPNET) tu-
pact on DFS. The response to induction chemotherapy pre-
mors (7,8) and other metastatic pediatric sarcomas (3,8 –
dicted for improved DFS and OS in those with a complete
13). A poor prognosis is also expected for recurrent
response compared to those with other responses. The pres-
pediatric sarcoma when presenting early (within 2 years
ence of pulmonary metastases did not predict outcome and
from initial treatment), or if multiple bony or pulmonary
6 of the 13 patients who had lung disease at initial presen-
sites are involved (14 –16). It is uncertain whether either
tation are alive: 3 who are relapse-free and another 3 who
local radiotherapy or total body irradiation (TBI) is tolerable
are alive following lung relapse. The fact that the presence
or effective in the treatment of metastatic sarcoma. The
of pulmonary mestastases on initial presentation did not
purpose of the present study was to determine the feasibility
predict for a worse outcome may indicate that these patients
and efficacy of using radiation therapy as consolidation
benefit from this aggressive treatment regimen.
treatment in pediatric patients with metastatic sarcomas
In addition, we compared the outcome of patients receiv-
treated with myeloablative chemoradiotherapy.
ing TBI to those receiving myeloablative chemotherapy
Myeloablative therapy may benefit select patients with
alone. We found that there was a trend for improved DFS
metastatic or recurrent disease. These include patients with
with the use of TBI, but TBI did not significantly impact on
low tumor burden or high tumor burden, which is amenable
overall survival (OS). Likewise, although CRT did have a
to consolidative radiation therapy (CRT). For example, an
significant impact on DFS, CRT also had no impact on
improved 6-year event-free survival (EFS) of 45% was
overall survival. However, only an appropriately designed
achieved in select metastatic or recurrent Ewing’s sarcoma
prospective, randomized trial would be able to determine
patients who received high dose chemotherapy (HDC) and
the true impact of TBI and CRT. But this may not be
12 Gy TBI compared to 2% EFS in a historic control group
possible as a large number of patients and a long follow-up
treated with conventional therapy (17). These select poor
period would be required, which has been shown to be
risk patients could not have bulky disease or progression
needed to detect any survival advantage when radiation
during induction chemotherapy. One study that reported
provides local control (24,25). Also, we still do not have a
superior results for bulk disease with myeloablative therapy
prospective, randomized trial that compares conventional
and CRT was a retrospective review by the University of
multimodality therapy to myeloablative regimens in pediat-
Florida (18). Patients had primarily localized disease and
ric patients with poor-risk disease.
2-year disease-free survival (DFS) was 80%.
The present study analyzes the feasibility and efficacy of
The University of Florida report supports the use of CRT
using CRT in pediatric/young adult patients with poor-risk
to reduce bulky disease such that HDC would also be as
disease treated with myeloablative therapy with or without
successful in patients with high tumor burden; however,
TBI. The impact of both tumor and treatment factors on
these were patients with primarily localized disease. Pa-
prognosis were also retrospectively assessed.
tients with metastasis have been shown to have a worseoutcome (5,15). In a study conducted at the National Cancer
METHODS AND MATERIALS
Institute (1), 31 patients with metastatic Ewing’s sarcomaand rhabdomyosarcoma who had a complete response (CR)
Eligibility criteria for patients entered into this high dose
to induction therapy and irradiation to the primary and
chemoradiotherapy protocol included children and young
metastatic sites received high dose chemotherapy and TBI
adults with metastatic or recurrent sarcomas referred to the
with autologous bone marrow infusion. Patients with met-
University of Chicago Children’s Hospital. Patients that
astatic disease had a 19% 6-year EFS, significantly worse
were excluded from the study included adults and all pa-
compared to the 45% 6-year EFS reported by Burdach et al.
tients with osteosarcomas. Twenty-three patients were eli-
gible for this study and 21 patients with a median age of
The most common site of metastatic disease on initial
17.8 years (9.4 –24.7 years) were treated with myeloablative
presentation is the lung (1,5,19) and this site is not amenable
therapy with ASCR between June 1987 and April 1997.
to curative irradiation. Aggressive multimodality therapy to
Two of the 23 original patients had rapidly progressive
the lung is limited by our inability to resect all disease
disease during induction chemotherapy and did not undergo
and/or irradiate to a high enough dose due to risk of organ
myeloablative therapy or consolidative radiation therapy
injury. Likewise, the lung is the most common site of failure
and were not involved in this analysis. Patients were staged
both in other studies and in the present study (13 of 21 total
with plain films of the primary site, a bone scan, CXR,
patients relapsed in the lung). In this study, patients were
computed tomography (CT) of the lungs, CT or magnetic
eligible despite presence of bulky diseases or induction
resonance imaging (MRI) scan of the primary site and bone
Radiation therapy for metastatic pediatric sarcomas ● E. A. DUNPHY CZYZEWSKI et al.
Table 1. Patient and tumor characteristics
tients all had individualized chemotherapy according toprevious chemotherapy treatment.
Surgical resections included resection of the primary and
thoracotomy for resection of lung metastases. Primary tu-
mor resections included the tumor and surrounding com-
partment. The adjacent bone was resected when local inva-
sion into bone was noted on the MRI scan. Metastatic
lesions to the lung were resected by thoracotomy if residual
lesions were found after chemotherapy induction. In one
patient who underwent thoracotomy for lung metastases,
resection of pericardial disease was also performed.
Fifteen patients underwent surgical resection to a total of
17 sites; 7 of these sites were diffuse lung disease. The
procedure used in the treatment of 7 diffuse lung sites
included thoracotomies with wedge resections and all nod-
ules were completely resected in 3 (patients 3, 14, and 15),
but incompletely resected in 4 patients (patients 12, 16, 20,
and 21). Patients 3, 12, and 15 received whole lung CRT
following myeloablative therapy (details to follow). The 11
remaining sites underwent surgical resection with CRT (4
patients) or surgery alone (7 patients). The 6 sites that
rib, scapula, chest wall/lung, flank, breast, spine,
underwent surgery alone had complete resection in 4 (pari-
etal bone, breast, pericardium, humerus), microscopic resid-
ual in 1 (breast/axilla) and gross residual in 1 (breast). The
4 sites that underwent surgery and CRT consisted of pleura
(2), pelvis/thigh (1), and thigh (1) masses; these were all
completely resected after induction therapy but prior to
myeloablative therapy and CRT except in one patient who
had a complete resection of pubic ramus 6 weeks after CRT
and stem cell reinfusion (patient 8).
Surgical resection was performed prior to myeloablative
therapy in all patients except one; this patient had resectionof pubic ramus 6 weeks after stem cell reinfusion.
marrow biopsy. The clinical characteristics are shown in
Table 1. In the 10 patients with primary metastatic disease,
Stem cells were obtained by bone marrow aspiration (11
the metastatic sites were: lung only (5 patients), a solitary
patients) or peripheral stem cell harvesting (10 patients).
bone (1 patient), and multiple sites (4 patients). In the 11
High dose cytoxan was used to mobilize peripheral stem
patients with recurrent disease, the relapse sites were: pri-
cells. Myeloablative therapy consisted of high dose chemo-
mary site only (2 patients), lung only (6 patients), multiple
therapy alone in 10 patients, either with thiotepa/carboplati-
bones (2 patients), and multiple sites (1 patient).
num/etoposide (8 patients) or cytoxan/carboplatinum (2 pa-tients). Eleven patients underwent TBI with either high dose
melphalan/etoposide (9 patients) or high dose cytoxan/thio-
Twenty patients were treated with induction chemother-
tepa (2 patients). TBI consisted of 12 Gy in 2 Gy fractions
apy. The one patient who was not treated with induction
delivered twice daily over 3 days using techniques as de-
chemotherapy presented with lung relapse and was treated
scribed below and previously (20,21). These fractions were
with thoracotomy alone prior to high dose chemotherapy
given a minimum of 4 h apart. One patient received an
and ASCR. All 11 recurrent disease patients had been
alternate regimen of 15 Gy in 1.25 Gy fractions delivered
treated with previous chemotherapy regimens prior to re-
three times daily over 4 days. TBI was delivered with 24
mV photons, right and left lateral opposed fields, at an
Induction chemotherapy regimens consisted of ifospha-
extended source to patient midplane distance of 410 cm at a
mide and etoposide in 5 patients; vincristine, adriamycin
dose rate of approximately 0.12 to 0.15 Gy/min. Dose
and cytoxan (VAC) in 2 patients; VAC and MESNA in 4
homogeneity was 97 to 105% along the patient midplane.
patients, VAC and ifosphamide in 1 patient; VAC and
The dose to the lung was kept below 12 Gy with use of
ifosphamide/etoposide in 2 patients. The remaining 6 pa-
customized partial transmission lung blocks. Patients were
I. J. Radiation Oncology ● Biology ● Physics
treated in the supine position with head and extremity bolusand a 1.2 cm polycarbonate beam spoiler as previouslydescribed (18). Myeloablative therapy was followed bybone marrow or autologous stem cell rescue 24 to 48 hoursafter completing high dose chemotherapy.
Two patients had consecutive transplants; one patient due
to progressive disease during initial transplant and the sec-ond due to extensive disease at presentation consisting ofmultiple sites including bone marrow involvement.
Consolidative radiation therapy (CRT) was used to treat
the original site of the primary tumor (6 patients) and/ormetastatic lesions (12 patients). The median dose to the
Fig. 1. Survival of 21 patients receiving myeloablative chemora-
primary was 50 Gy (range 42.8 to 60 Gy) in patients with
diotherapy and consolidation radiotherapy for metastatic and re-
Ewing’s sarcoma or PPNET. One patient with rhabdomyo-
current sarcomas. Kaplan-Meyer analysis was used to generatesurvival these data.
sarcoma received 47 Gy and one patient with synovialsarcoma received 60 Gy to the primary site. The radiationtherapy dose for metastatic lesions other than whole lung
was given to liver metastases and in patient 18 there were
ranged from 20 to 50 Gy (median dose 31.5 Gy) for a total
diffuse bony metastases and not all rib metastases could
of 19 sites. Lung metastases treated with whole lung irra-
feasibly be irradiated or resected. The sites that received
diation consisted of 12.8 in 1.6 Gy fractions twice daily
CRT, 26 of 36 amenable sites and 3 unamenable (whole
(bid) (1 patient) and 15 Gy in 1.5 Gy fractions delivered 1.5
lung) sites, were chosen for CRT based on the discretion of
Gy daily (2 patients). In 6 patients with multiple lung
the treating physician. The 11 amenable sites, which under-
metastases with Ewing’s sarcoma or PPNET, the lungs
went surgery, as described in “Surgical Resection.”
received irradiation via TBI consisting of 12 Gy in 2 Gy
On completion of curative therapy, patients were fol-
fractions bid (not considered CRT). For twice daily irradi-
lowed initially at 2 to 3 month intervals and subsequently
ation, the interfraction interval was at least 4 hours apart.
biannually, then yearly. Follow-up studies included clinical
None of these CRT doses include the TBI dose.
examination, CXR or CT scan of the chest and CT or MRI
The radiation volume included the primary tumor, tumor
scans of the primary site. The median follow-up of surviv-
bed (including the scar) or metastatic site with a margin of
ing patients was 15 months (range, 8 –20) with 25% of
2 cm. Complete circumferential irradiation of extremities
patients having been followed for more than 20 months.
was not done to prevent development of lymphedema. Treated sites received external beam radiation with mega-
voltage in 1.8 to 2.0 Gy fractions. Exceptions consisted of
All statistical analyses were performed using statistical
2.5 Gy to 31.5 Gy to a paraspinal mass and use of 9 MeV
software. Local control, DFS and OS actuarial analyses
electrons to frontal bone and to a thigh scar (both in 2 Gy
were plotted according to the method of Kaplan-Meier and
fractions to 50 Gy). The majority of sites were treated with
compared by the log rank test. Comparison of proportions
opposed fields, usually AP/PA. Abdominal sites usually
was performed using the Chi-square test. All intervals were
were treated with 3 fields, which were individualized, to
determined from the date of the bone marrow transplant or
spare critical structures. Patients received appropriate im-
mobilization and customized blocking.
Fourteen patients (67%) underwent CRT either prior to (5
patients) or following (9 patients) myeloablative therapy. Sites were divided into amenable and unamenable sites. An
amenable site was defined as metastasis in an organ or tissue
Twenty-three patients were eligible for myeloablative
that could be treated to a curative dose without exceeding
therapy for metastatic or recurrent pediatric sarcoma. Two
the dose or volume that is tolerated by that tissue. The 51
of these patients had rapidly progressive disease during
disease sites consisted of 36 amenable and 15 unamenable
induction chemotherapy and were not treated with myeloa-
to CRT sites (13 diffuse lung and 2 bone marrow sites). Of
blative therapy or consolidative radiation therapy and were
the 36 amenable sites, 3 received no local therapy, 22
not involved in this analysis. Of the 21 patients analyzed, 6
received CRT, 4 received surgery and CRT, and 7 received
are disease-free and 3 are alive with disease; 11 patients
surgery alone. Three amenable sites did not receive any
have died from progressive disease and 1 patient died from
local therapy under the discretion of the treating physician:
a pulmonary embolus 2 months after ASCR. The 3-year
in patient 11 it was not feasible to irradiate all 6 involved
actuarial and OS rates are 36% and 27%, respectively (Figs.
sites, therefore, an L3/L4 was not irradiated and surgical
resection was not feasible; in patient 13 no local therapy
Of the 21 patients treated with myeloablative therapy, 20
Radiation therapy for metastatic pediatric sarcomas ● E. A. DUNPHY CZYZEWSKI et al.
Stem cell engraftment was defined as ANC Ͼ1000 and
platelets Ͼ100,000. The average time to engraftment was16 days for neutrophils (21 patients) and 43 days for plate-lets (14 patients who attained engraftment). Three patientscontinued to have thrombocytopenia Ͼ 3 months followingbone marrow or stem cell reinfusion. Two of these threepatients received TBI and 2 had CRT to Ͼ 2 bone sites. Twopatients died before there was sufficient time for plateletengraftment.
Toxicities following autologous bone marrow or stem
Fig. 2. Disease-free survival 21 patients receiving myeloablative
cell reinfusion included grade 2 mucositis (4 patients), grade
chemoradiotherapy and consolidation radiotherapy for metastatic
2 esophagitis (2 patients), prolonged thrombocytopenia with
and recurrent sarcomas. Kaplan-Meyer analysis was used to gen-
platelet dependence (5 patients), neutropenic fever (5 pa-
tients), sepsis (1 patients), infectious diarrhea (3 patients),pneumonia (3 patients), skin infection (4 patients), andpulmonary embolus (1 patients). Treatment related fatalities
were treated with induction chemotherapy and 1 patient
occurred in one patient with pulmonary embolus. A partial
underwent thoracotomy alone for lung relapse prior to my-
sagittal sinus thrombosis developed in one patient following
eloablative therapy. The response to induction therapy is
surgery. Diminished range of motion occurred in one pa-
shown in Table 2: 8 complete, 6 partial, 2 stable, and 4
tient who required a prosthesis after surgical resection of the
progressive disease. Induction therapy included surgical
proximal femur. One patient developed chronic enteritis
debulking in 11 patients and CRT in 5 patients. Following
requiring donnatal following abdominal irradiation.
engraftment, 9 patients underwent CRT and surgical exci-sion was performed in one patient resulting in a CR.
Responses following myeloablative treatment were: 11
The following tumor and treatment factors were analyzed
complete, 6 partial, 1 stable, and 3 progressive disease. Six
for their impact on DFS and OS: induction chemotherapy
patients are disease-free (NED) and all had either a PR/CR
response, TBI, CRT, extent of surgical resection, histology,
with induction therapy and a CR with myeloablative ther-
age at diagnosis, stage, presence of pulmonary metastases,
apy. Table 2 lists the disease sites and type of local therapy
and prior treatment. Factors associated with improved DFS
if given. In the 6 NED patients, 5 unamenable sites were
in univariate analysis were induction chemotherapy re-
controlled, consisting of 4 lung and 1 bone marrow. All of
sponse (p ϭ 0.002) and extent of surgical resection (p ϭ
these patients had TBI. When comparing myeloablative
0.045). There was a trend for improved DFS on univariate
regimens, we found that 5 of 10 patients treated with TBI
analysis with the use of TBI as part of myeloablative ther-
and 1 of 11 patients treated with high dose chemotherapy
apy (p ϭ 0.07). The one factor associated with improved OS
alone are presently free of disease (p Ͻ 0.07).
on univariate analysis was induction chemotherapy re-sponse (p ϭ 0.007). There was a trend for improved OS on
univariate analysis if there was a complete surgical resec-
Fifty-one disease sites were present prior to myeloabla-
tion (p ϭ 0.07). Multivariate analysis with respect to DFS
tive therapy. Twelve sites (24%) were bulky, defined as Ͼ
and OS revealed that induction chemotherapy response is
8 cm in size. Eighteen (35%) underwent surgical debulking.
the only factor that remains significant (p ϭ 0.032 for DFS
Of the 51 disease sites present prior to myeloablative ther-
and p ϭ 0.017 for OS). Patients with complete response to
apy, 36 sites (71%) were amenable to CRT. Non-amenable
induction therapy had 40% probability of survival versus all
sites were: multiple lung metastases (13) and bone marrow
other patients who had 10% survival (p ϭ 0.05).
(2). Twenty-six amenable sites (51%) received CRT eitherprior to (14) or following (12) ASCR. Amenable sites
treated with CRT had a better 3-year actuarial local control
Fifteen patients (71%) have relapsed. The most common
(80 vs. 37%) (p ϭ 0.0065) than amenable sites not treated
sites of relapse were lung (13) and/or bone marrow (2).
with CRT. Median CRT dose was 37.2 Gy (range, 20 – 60).
Recurrence within the field of CRT occurred in 6 patients:
A higher rate of local control was achieved with the dose
in 3 unamenable sites consisting of all 3 patients who
range 31 to 60 Gy compared to 20 to 30 Gy. There were 4
received whole lung CRT, and in 3 amenable sites consist-
bulky disease sites in the NED group, all were controlled
ing of 1 patient who received 27 Gy to a femur lesion, 1
with CRT. The 5 other amenable sites were controlled with
patient with a frontal bone lesion treated with electrons to
either surgery or CRT and one site was controlled with no
50 Gy and in 1 patient with extensive vertebral disease from
T3 to S1 treated to 43.2 Gy. There were no recurrences at
I. J. Radiation Oncology ● Biology ● Physics
A, amenable; UL, unamenable/lung; UB, unamenable/bone marrow; B, bulky; S, surgery; R, CRT; 0, no local therapy.
the margin of irradiation. Recurrence outside the field of
therapy in four patients. The three salvaged patients who
consolidation therapy occurred in eight patients. Out of field
remain alive were salvaged with lung resections.
CRT recurrences included the lung in 6 patients, lung andbone marrow in 1 patient, and lung, liver, and sacrum in 1patient. DISCUSSION
We retrospectively analyzed the impact of local irradia-
tion for consolidation with respect to local control in pedi-
Ten patients were treated with salvage therapy. Seven of
atric patients with metastatic or recurrent sarcomas treated
these patients did not survive and their salvage therapy
with high dose chemo/radiotherapy and stem cell rescue as
consisted of a second course of myeloablative therapy in
part of a feasibility study. The patients in this study received
one patient who had progressive disease during high dose
myeloablative therapy regardless of their response to induc-
chemotherapy; etoposide followed by tumor vaccine with
tion chemotherapy unless they were rapidly progressing and
interleukin-2 in one patient; high dose methotrexate fol-
regardless of the initial extent of disease. The present study
lowed by alpha interferon in one patient; palliative radiation
included 2 patients with no response and 3 patients who
Radiation therapy for metastatic pediatric sarcomas ● E. A. DUNPHY CZYZEWSKI et al.
progressed during induction chemotherapy, 10 patients with
(3). Those without TBI achieved a better EFS rate at 34%
bulky disease (Ͼ 8 cm), and 8 patients with multiple sites
compared to 19% in the group with TBI. Also, 8 Gy TBI (two
(Ͼ 3 sites). Consolidative radiation therapy was able to
4 Gy fractions) and HDC did not improve outcome in the 31
provide 80% 3-year actuarial local control to those sites
patients treated at the NCI with metastatic Ewing’s sarcoma
irradiated. This is significantly improved compared to the
and rhabdomyosarcoma who had a complete response (CR) to
other amenable sites of disease that did not receive radiation
induction therapy and CRT (1). Seventy percent of patients
which had a 37% 3-year actuarial local control (p ϭ
with metastatic disease at diagnosis failed distantly and 70% of
these distant failures were either in the lung and/or bone
The use of CRT may have contributed to our comparable
marrow. It was concluded that either the induction therapy
results despite many patients with poor induction chemother-
delivered 4 to 6 months prior to TBI caused radioresistance or
apy response and bulk disease. CRT is useful in additionally
that the amount of cell kill from 2 fractions of 4 Gy was
reducing local tumor that is not eradicated by induction che-
insufficient to eliminate occult disease. The Austrian/German
motherapy either due to (a) tumor bulk or (b) chemoresistance.
experience found that after 8 Gy fractionated TBI in patients
CRT could potentially convert patients into a “select” category
with multifocal Ewing’s sarcoma, the lung was the predomi-
by eliminating disease at bulky sites and at sites of progression
nant site of relapse after BMT (19). We propose that 8 Gy TBI
during induction chemotherapy. In the present study, it is
is an insufficient dose and we are continuing to accrue patients
difficult to determine the CRT dose that is required to achieve
to a regimen consisting of 12 Gy given as 2 Gy twice daily.
tumor control. There were a total of 26 amenable sites treated
The presence of pulmonary metastases on initial presen-
with CRT and only 3 of these sites failed following treatment.
tation did not predict outcome and 6 of the 13 patients who
These sites were a femur treated to 27 Gy, spine T3-S1 treated
had lung disease at initial presentation are alive: 3 who are
to 43.2 Gy, and a frontal bone treated to 50 Gy. All other sites
relapse-free and another 3 who are alive following lung
of disease were controlled, consisting of 7 sites that received
relapse. The 3 patients who are relapse-free all had TBI and
20 –30 Gy and 16 sites that received 31– 60 Gy. The NCI
1 had lung wedge resections; in those 3 patients who are
reported a 19% EFS in 31 patients with metastatic Ewing’s
alive following lung relapse, 2 patients had both whole lung
sarcoma or rhabdomyosarcoma who received induction che-
irradiation and lung wedge resections at time of myeloabla-
motherapy and CRT (50 to 60 Gy) to local disease (1). In
tive therapy. There were a total of 3 patients who received
another study, a median CRT dose of 35 Gy achieved excellent
whole lung irradiation, all have relapsed in the lung. The 2
local control (6). Patients received chemotherapy followed by
patients who had bone marrow disease at initial presentation
surgery and/or CRT. At almost 4 years, 10 patients were
remain relapse-free. Both of these patients received TBI. It
is difficult to make any definite conclusions with regards to
In the present study, bulky disease was not associated
the impact of lung irradiation/TBI in these patients present-
with a worse prognosis. Local control was achieved in 10 of
ing with pulmonary metastases and/or bone marrow in-
the 12 bulky sites: 7 with CRT alone, 2 with surgery and
volvement on initial presentation. However, it is promising
CRT, and in 1 site with surgery alone. The two bulky sites
that TBI did show a trend for improved disease-free survival
that failed consisted of chest/axilla (patient 14) treated with
on univariate analysis. Likewise, the fact that the presence
surgery alone and spine T3-S1 (patient 18) treated with
of pulmonary metastases on initial presentation did not
CRT to a dose of 43.2 Gy. Bulky disease has been shown to
predict for a worse outcome may indicate that these patients
be a poor prognostic factor in previous studies (15,22). The
benefit from this aggressive treatment regimen.
NCI reported on their experience from 1968 –1980 for both
Certain patients with lung metastases or bone marrow dis-
local and primary metastatic disease for Ewing’s sarcoma of
ease can be cured. It appears that our present myeloablative
the bone. Poor prognostic factors were found to be meta-
chemotherapy regimens and TBI radiation doses are most
static disease at presentation, high LDH (Ͼ350 IU) in
effective if lung or bone marrow tumor burden is below a
localized disease patients and central primary tumors in
certain threshold and if the tumor has demonstrated a response
localized disease patients (15). All of these factors were
to chemotherapy. This rationale would support giving myeloa-
considered to be associated with tumor bulk. At the Uni-
blative therapy only to those patients who have had a CR or PR
versity of Florida between 1966 and 1981, Ewing’s sarcoma
from induction chemotherapy. Those patients who had only a
patients with metastatic or primary tumor size of Ͼ 8 cm
PR would benefit from myeloablative therapy if they could be
who were treated for cure had a worse outcome (22).
rendered a CR with CRT or surgery prior to myeloablative
Therefore, patients with bulky and or metastatic disease are
therapy. The role of myeloblative therapy and TBI would then
often treated more aggressively with myeloablative therapy.
be to eliminate any residual micrometastases. The above treat-
We found that patients receiving 12 Gy TBI had an im-
ment rationale is supported by the fact that in the 6 patients
proved disease-free survival as compared to patients receiving
who remain NED in the present study, all had either a CR or
chemotherapy alone for myeloablation. This finding was sup-
PR from induction chemotherapy and all amenable sites except
ported by the study by Burdach et al. (17) that showed superior
one (a lumbar spine metastasis) had local therapy with either
results using TBI. In contrast, the European BMT Tumor
Registry experience with myeloablative therapy in Ewing’s
Another concern these patients are the high relapse rate in
sarcoma patients compared regimens with and without TBI
the lungs, illustrated by the fact that in the present study, 13
I. J. Radiation Oncology ● Biology ● Physics
patients failed in the lung. Another approach to possibly
In conclusion, consolidative radiotherapy is feasible in
improve outcome would be increasing the radiation dose to
patients with metastatic or recurrent pediatric sarcomas
the lungs. A retrospective analysis by Dunst et al. (23)
treated with myeloablative therapy with or without TBI.
showed a dose-response relationship in 22 Ewing’s sarcoma
Overall, this aggressive treatment regimen was tolerable
patients with pulmonary metastases at diagnosis treated
with the primary toxicity from myeloablative therapy
with bilateral lung irradiation.Four of 10 patients treated
being prolonged thrombocytopenia. Only one patient de-
with 12 to 16 Gy vs. 5 of 6 patients receiving 18 to 21 Gy
veloped a long-term complication from CRT consisting
lung irradiation were in remission. The results suggested
of chronic enteritis. DFS is improved with CRT and there
that 18 to 21 Gy might control 75% of pulmonary disease in
is a trend for improved DFS with TBI. Both DFS and OS
patients with a complete radiographic remission following
are improved in those with a CR following induction
chemotherapy. No severe late lung toxicities were reported.
chemotherapy compared to those with other responses.
We are presently treating the lungs with a total dose of 18
The 3-year DFS of 36% and OS of 27% are comparable
Gy in patients with biopsy-proven lung metastases.
to the outcome of large prospective, randomized trials
The toxicity associated with CRT was acceptable consisting
reported in the literature, including trials that did not use
of a single patient with chronic enteritis requiring donnatal
myeloablative therapy. It is not known whether myeloa-
following treatment to the abdomen. Myeloablative therapy
blative therapy adds any additional benefit in patients
consisted of the expected severe acute toxicities to the marrow,
who have already achieved a CR prior to myeloablative
mucosa, and gastrointestinal tract. There was one death from a
therapy. Only a prospective, randomized trial would be
pulmonary embolus soon after myeloablative therapy. REFERENCES
1. Horowitz ME, Kinsella TJ, Wexler LH, Belasco J, Triche T,
10. Crist W, Gehan EA, Ragab AH, et al. The Third Intergroup
Tsokos M, Steinberg SM, McClure L, Longo DL, Steis RG,
Rhabdomyosarcoma study. J Clin Oncol 1995;13:610 – 630.
Glatstein E, Pizzo P, Miser JS. Total-body irradiation and
11. Emminger W, Emminger-Schmidmeier W, Hawliczek R, Pe-
autologous bone marrow transplant in the treatment of high-
ters C, Hocker P, Gadner H. High-dose melphalan, etopo-
risk Ewing’s sarcoma and rhabdomyosarcoma. J Clin Oncol
side Ϯ carboplatin (MEC) combined with 12-gray fractionated
total-body irradiation in children with generalized solid tu-
2. Ladenstein R, Gadner H, Hartmann O, Pico J, Biron P, Thierry
mors. Pediatr Hematol Oncol 1991;8:13–22.
P. The European experience with megadose therapy and au-
12. Koscielniak E, Rodary C, Flamant F, Carli M, Treuner J,
tologous bone marrow transplantation in solid tumors with
Pinkerton CR, Grotto P. Metastatic rhabdomyosarcoma and
poor prognosis Ewing sarcoma, germ cell tumors and brain
histologically similar tumors in childhood: A retrospective
tumors. Wiener Medizinische Wochenschrift 1995;145:55–
European multi-center analysis. Med Pediatr Oncol 1992;20:
3. Ladenstein R, Hartmann O, Pinkerton CR. The role of mega-
13. Seeger RC, Reynolds CP. Treatment of high-risk solid
therapy with autologous bone marrow rescue in solid tumours
tumors of childhood with intensive therapy and autologous
of childhood. Ann Oncol 1993;1:45–58.
bone marrow transplantation. Pediatr Clin N Am 1991;38:
4. Miser JS, Kinsella TJ, Triche TJ, Tsokos M, Forquer R,
Wesley R, Horvath K, Belasco J, Longo DL, Steis R, Glatstein
14. Hayes FA, Thompson EI, Kumar M, Hustu HO. Long-term
E, Pizzo PA. Preliminary results of treatment of Ewing’s
survival in patients with Ewing’s sarcoma relapsing after
sarcoma of bone in children and young adults: Six months of
completing therapy. Med Pediatr Oncol 1987;15:254 –256.
intensive combined modality therapy without maintenance.
15. Kinsella TJ, Miser JS, Waller B, Venzon D, Glatstein E,
Weaver-McClure L, Horowitz ME. Long-term follow-up of
5. Cangir A, Vietti TJ, Gehan EA, Burgert E Jr, Thomas P,
Ewing’s sarcoma of bone treated with combined modality
Tefft M, Nesbit ME, Kissane J, Pritchard D. Ewing’s sar-
therapy. Int J Radiat Oncol Biol Phys 1991;20:389 –395.
coma metastatic at diagnosis. Results and comparisons of
16. Klingebiel TH, Bode U, et al. Treatment of relapse in soft
two intergroup Ewing’s sarcoma studies. Cancer 1990;66:
tissue and Ewing’s sarcoma patients. A phase II trial (CESS/
CWS REZ 91). Med Pediatr Oncol 1993;21:573 (Abst.).
6. Hayes FA, Thompson EI, Parvey L, Rao B, Kun L, Parham D,
17. Burdach S, Jurgens H, Peters C, Nurnberger W, Mauz-Kor-
Hustu HO. Metastatic Ewing’s sarcoma: Remission induction
holz C, Korholz D, Paulussen M, Pape H, Dilloo D, Ko-
and survival. J Clin Oncol 1987;5:1199 –1204.
scielniak E, Gadner H, Goebel U. Myeloablative radiochemo-
7. Bader JL, Horowitz ME, Dewan R, Watkins E, Triche TJ,
therapy and hematopoietic stem-cell rescue in poor-prognosis
Tsokos M, Kinsella TJ, Miser JS, Steinberg SM, Glatstein E.
Ewing’s sarcoma. J Clin Oncol 1993; 11:1482–1488.
Intensive combined modality therapy of small round cell and
18. Marcus RB, Graham-Pole JR, Springfield DS, Fort JA, Gross
undifferentiated sarcomas in children and young adults: local
S, Mendenhall NP, Elfenbein GJ, Weiner RS, Enneking WF,
control and patterns of failure. Radiother Oncol 1989;16:189 –
Million RR. High-risk Ewing’s sarcoma: End-intensification
using autologous bone marrow transplantation. Int J Radiat
8. Jurgens H, Bier V, Harms D, et al. Malignant peripheral
neuroectodermal tumors. A retrospective analysis of 42 pa-
19. Pape H, Wurm R, Burdach S, Nuernberger W, Bannach B,
Schmitt G. Die lunge als hauptort der rezidive nach knochen-
9. Carli M, Pinkerton R, et al. Risk group analysis in metastatic
mark-transplantation multifokaler Ewing-Sarkome: Sollte die ra-
soft tissue sarcomas in children. European Intergroup Study
diotherapie intensiviert werden? Zbl Radiol 1993;147:948 –949.
20. Bradley J, Reft C, Goldman S, Rubin C, Nachman J, Larson R,
Radiation therapy for metastatic pediatric sarcomas ● E. A. DUNPHY CZYZEWSKI et al.
Hallahan DE. High energy total body irradiation in the prep-
sults of the CESS-studies. Strahlentherapie und Onkologie
aration for bone marrow transplantation in leukemia patients.
Int J Radiat Oncol Biol Phys 1998;40:391–396.
24. Ragaz J, Jackson SM, Le N, Plenderleith IH, Spinelli JJ,
21. Sibley G, Mundt A, Hallahan D, Goldman S, Nachman J, Reft
BascoVE, Wilson KS, Knowling MA, Coppin CM, Paradis M,
C, Weichselbaum R, Hallahan D, Johnson L. Pattern of fail-
Coldman AJ, Olivotto IA. Adjuvant radiotherapy and chemo-
ures following total body irradiation and bone marrow trans-
therapy in node-positive premenopausal women with breast
plantation Ϯ local boost for advanced Neuroblastoma. Int J
cancer. N Engl J Med 1997; 337(14):956 –962.
Radiat Oncol Biol Phys 1995;32:1127–1135.
25. Overgaard M, Hansen PS, Overgaard J, Rose C, Andersson
22. Marcus RB Jr, Million RR. The effect of primary tumor size
M, Bach F, Kjaer M, Gadeberg CC, Mouridsen HT, Jensen
on the prognosis of Ewing’s sarcoma. Int J Radiat Oncol Biol
MB, Zedeler K. Postoperative radiotherapy in high-risk
premenopausal women with breast cancer who receive ad-
23. Dunst J, Paulussen M, Jurgens H. Lung irradiation for Ew-
juvant chemotherapy. Danish Breast Cancer Cooperative
ing’s sarcoma with pulmonary metastases at diagnosis: Re-
Group 82b Trial. N Engl J Med 1997;337(14):949 –955.
Rycoben SC for Sheep Introduction Frimley Business Park Frimley Camberley Surrey GU16 7SR 01276 694402 01276 694403 Presentation A creamy pink coloured aqueous suspension containing 2.5% w/v ricobendazole (albendazole oxide) for the treatment of sheep. Contains 1.8% w/v hydrated cobalt sulphate (equivalent to 3.77 mg of elemental cobalt/ml) and 0.19% w/v hydrated sodi
PHYSICIAN’S ORDERS ADDRESSOGRAPH COMPLETE OR REVIEW ALLERGY STATUS PRIOR TO WRITING ORDERS (items with check boxes must be selected to be ordered) (Page 1 of 5) Date: ________________ Time: ____________ Weight: ______ Kg Actual Estimate Admission Diagnosis:_____________________________________ Admitting Physician:______________________________________ Code status:____
 Int. J. Radiation Oncology Biol. Phys., Vol. 44, No. 3, pp. 569 –577, 1999
Copyright 1999 Elsevier Science Inc.
Int. J. Radiation Oncology Biol. Phys., Vol. 44, No. 3, pp. 569 –577, 1999
Copyright 1999 Elsevier Science Inc.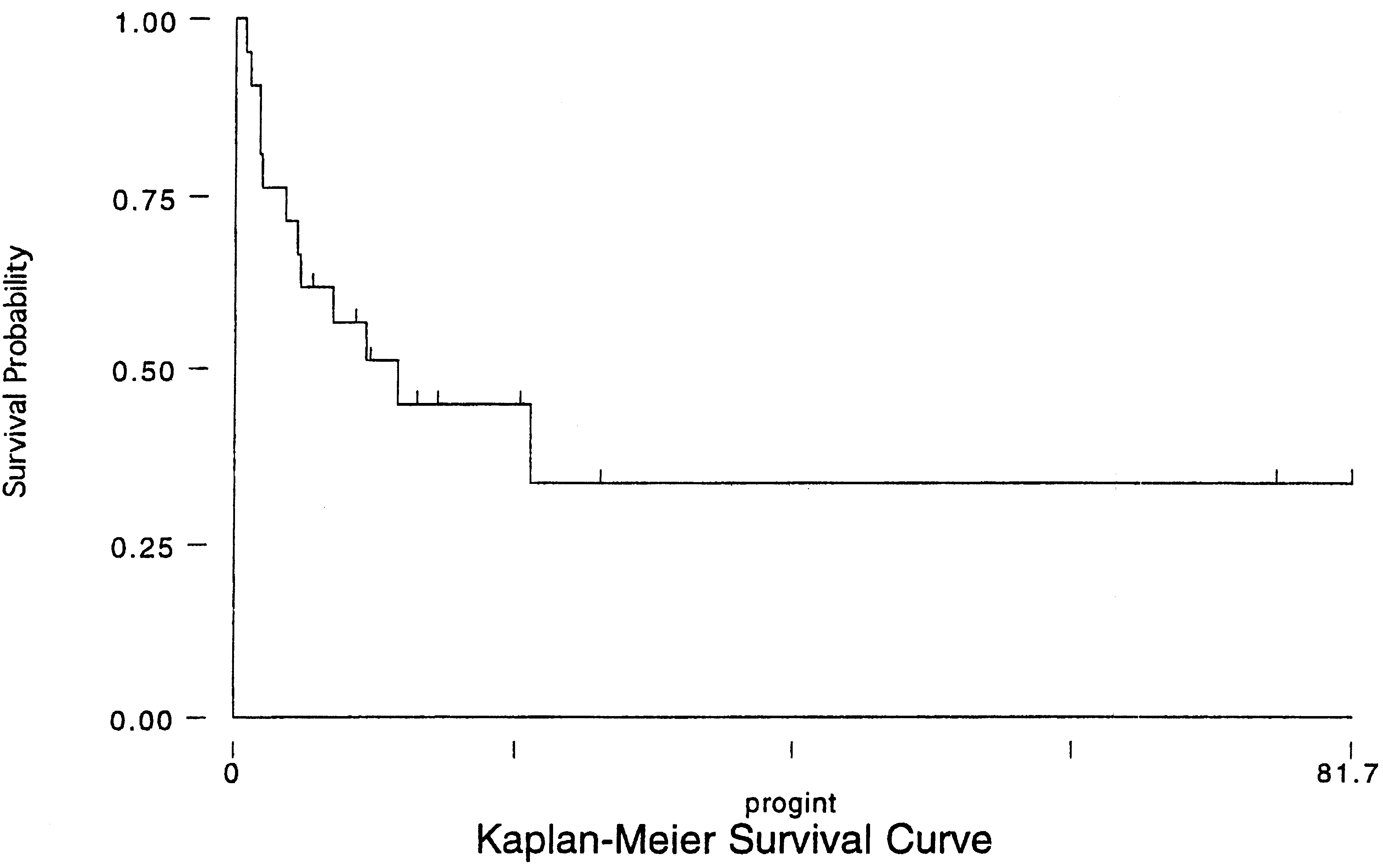 I. J. Radiation Oncology ● Biology ● Physics
treated in the supine position with head and extremity bolusand a 1.2 cm polycarbonate beam spoiler as previouslydescribed (18). Myeloablative therapy was followed bybone marrow or autologous stem cell rescue 24 to 48 hoursafter completing high dose chemotherapy.
I. J. Radiation Oncology ● Biology ● Physics
treated in the supine position with head and extremity bolusand a 1.2 cm polycarbonate beam spoiler as previouslydescribed (18). Myeloablative therapy was followed bybone marrow or autologous stem cell rescue 24 to 48 hoursafter completing high dose chemotherapy.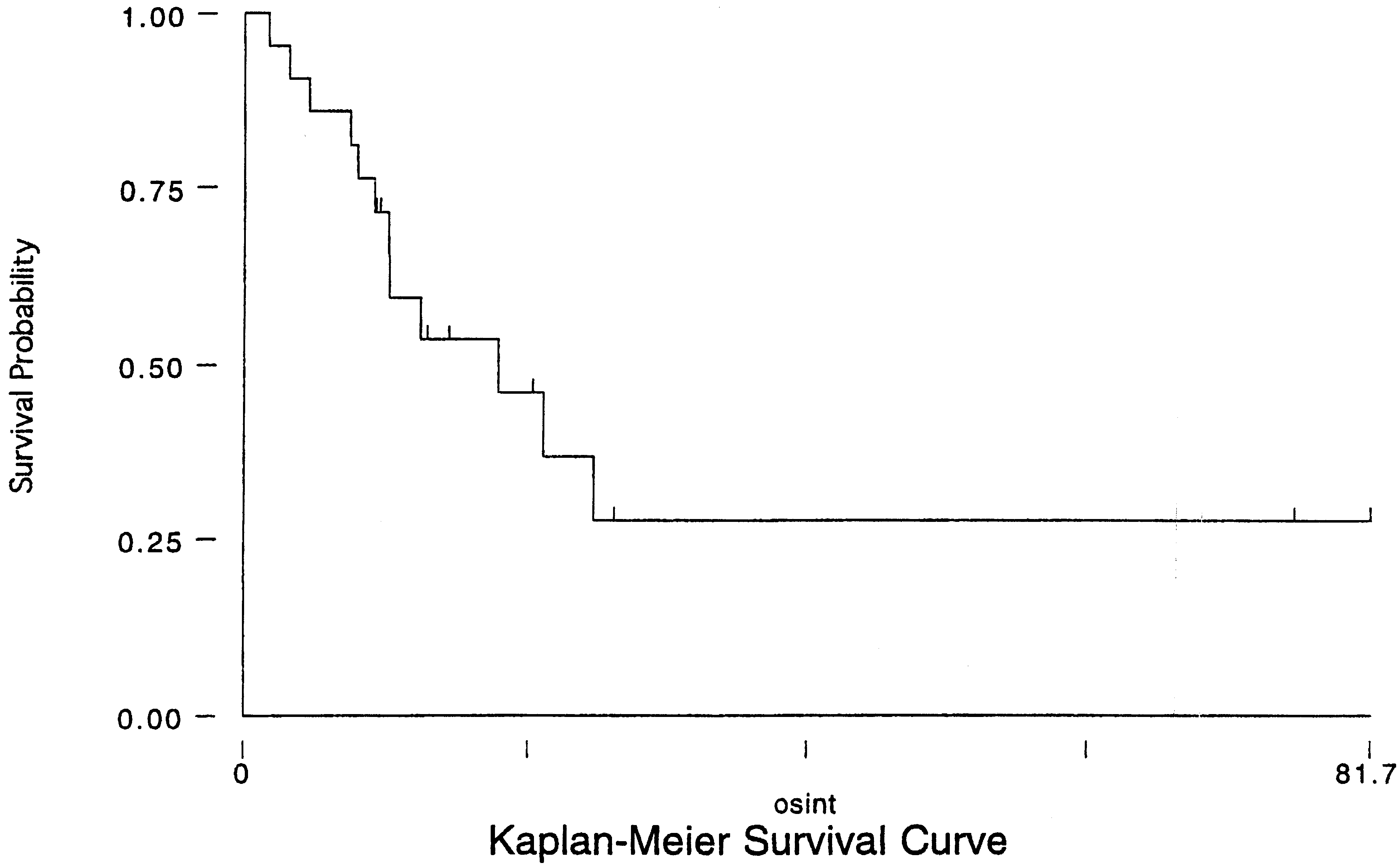 Radiation therapy for metastatic pediatric sarcomas ● E. A. DUNPHY CZYZEWSKI et al.
Stem cell engraftment was defined as ANC Ͼ1000 and
platelets Ͼ100,000. The average time to engraftment was16 days for neutrophils (21 patients) and 43 days for plate-lets (14 patients who attained engraftment). Three patientscontinued to have thrombocytopenia Ͼ 3 months followingbone marrow or stem cell reinfusion. Two of these threepatients received TBI and 2 had CRT to Ͼ 2 bone sites. Twopatients died before there was sufficient time for plateletengraftment.
Radiation therapy for metastatic pediatric sarcomas ● E. A. DUNPHY CZYZEWSKI et al.
Stem cell engraftment was defined as ANC Ͼ1000 and
platelets Ͼ100,000. The average time to engraftment was16 days for neutrophils (21 patients) and 43 days for plate-lets (14 patients who attained engraftment). Three patientscontinued to have thrombocytopenia Ͼ 3 months followingbone marrow or stem cell reinfusion. Two of these threepatients received TBI and 2 had CRT to Ͼ 2 bone sites. Twopatients died before there was sufficient time for plateletengraftment.