Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Pool-108-6-4-185.nycmny.fios.verizon.net
MEDCO BY MAIL ORDER FORM Member Information Please verify or provide member information below.
❏ Please send me e-mail notices about the status of the
Member ID:
enclosed prescription(s) and online ordering at:
Group:
(Medco will keep this address on file for all orders from
this membership until another shipping address isprovided by any person in this membership.)
Daytime phone: Evening phone: Patient/doctor Information Fill out a separate section for each person requesting a prescription fill. If
he/she has more than one prescription from the same doctor, complete just one section but include allprescriptions in the envelope provided. If a person has prescriptions from more than one doctor, complete a newsection for each doctor and include all prescriptions. Additional patient/doctor space is provided on the next page.
❏Spouse ❏Dependent ❏Domestic partner
❏Spouse ❏Dependent ❏Domestic partner
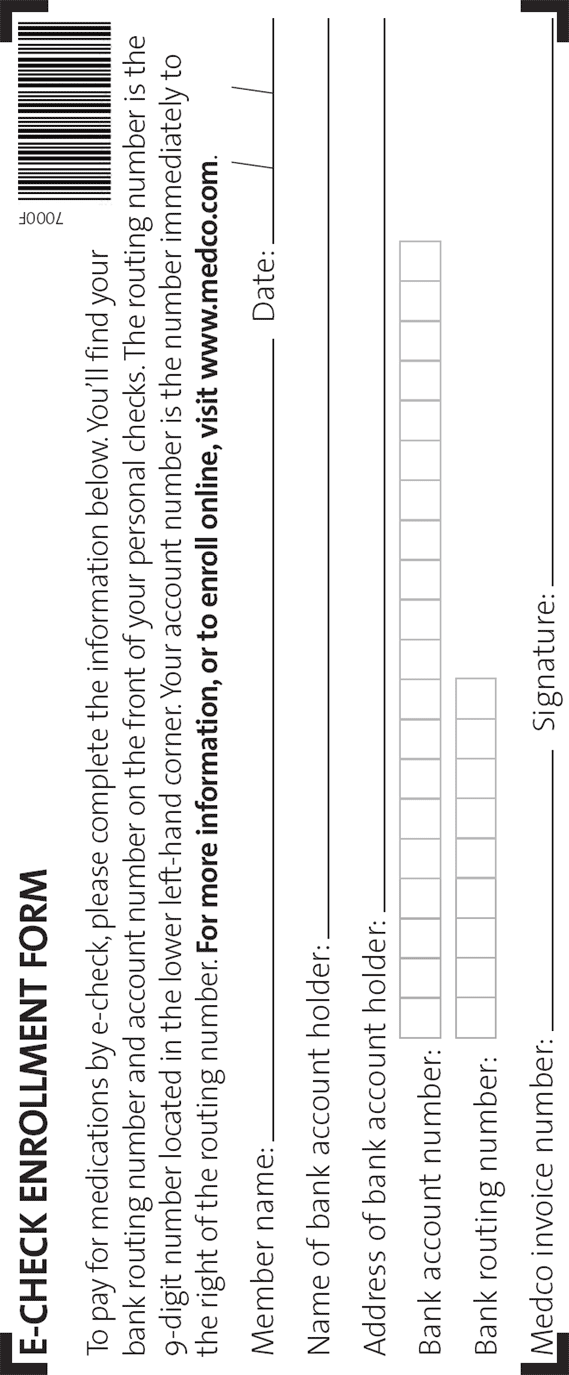
Complete your order You can pay by e-check, check, money order, or credit card. Make checks and
money orders payable to Medco Health Solutions, Inc., and write your member ID number on the front. To enroll for e-check payments, complete and return the e-check form (fifth page printed) with your order. Number of prescriptions sent with this order: Payment options: ❏e-check ❏Payment enclosed For credit card payments:
❏Visa ❏MC ❏Discover ❏AmEx ❏Diners
❏I authorize Medco to charge this card for all
orders from any person in this membership.
❏Rush this shipment ($15, subject to change). Note: This will not rush prescription processing. (Street address required; P.O. box not allowed.) Mailing instructions are provided on the next page Patient/doctor Information continued
❏Spouse ❏Dependent ❏Domestic partner
❏Spouse ❏Dependent ❏Domestic partner
Important reminders and other information Check that your doctor has prescribed the
Medco at the number on your member ID card and
maximum days' supply allowed by your plan, plus
ask to speak with a pharmacist. Pharmacists are
refills for up to 1 year, if appropriate (not a 30-day
available 24 hours a day, 7 days a week, to answer
questions concerning your prescription. Complete a patient/doctor section for each person
❏ If you live in Texas, you have a right to refuse
generic substitution. In many cases, choosing abrand-name product will result in a higher
Be sure you have filled out the Health & Medication
co-payment. Check the box if you do not want a less expensive, generic version of your Unpaid balances medication. Please note that this only applies to
If your plan limits the balance that you can carry on
this prescription and future refills of this
your account and you exceed that limit with this
order, payment must be included. To price a
If you have Medicare Part B coverage
medication, visit us online at www.medco.com and
Medco does not submit prescription drug claims to
click "Price a medication." To avoid processing
Medicare Part B. Check your Medicare Part B
delays, call Member Services to enroll in our
coverage to determine whether Medicare Part B
e-check program or provide a credit card number in
covers your prescription(s) and whether it will cost
the "Complete your order" section on side 1.
you less to use a Medicare Part B participating
Generic substitution
Texas, Florida and Ohio laws allow a generic
participating pharmacies, call your local Medicare
equivalent drug to be substituted for certain
carrier or call 1 800 MEDICARE (1 800 633-4227).
brand-name drugs, unless you or your physician
For questions about your Medco-administered
specifically directs otherwise. Ask your doctor or
coverage, please call Member Services.
pharmacist whether safe, effective and less
If you need additional information or
expensive generic drugs are right for you. Or, call
assistance, visit us online at www.medco.com or call Medco Member Services. Mailing instructions Medco Health Solutions of Fairfield P.O. Box 747050 Cincinnati, OH 45274-7050 Do not use staples or paper NMSFNP1W REV 12/07 X00000-00000-000-0000 12/07 Health, Allergy & Medication Questionnaire (HMQ) Your answers to the following questions will help us provide your prescription drug benefit services including, for example, filling prescriptions and alerting your doctor about possible medication problems. To best serve you, we need to know if you have any known allergies, conditions or diseases. ●
Please complete the questionnaire for each person in the household eligible for prescription drug benefits with Medco By Mail.
If you need additional forms you may copy this form or call your toll-free Member Services number. Please remember to print your group and member number on both pages. Return this questionnaire with your prescription or refill order form. Section 1 : Member Identification and Contact(Group and Member number required on all pages) Group Number Member Number(Located on your pharmacy Daytime Telephone Number benefit card and/or in your benefit information)Member/Subscriber First Name Last Name Street Address/Apt No. Section 2 : Drug Allergy Conditions For each covered family member, include their first name, date of birth, and gender. For each family member, fill in the circle ONLY if an allergy or bad reaction happened anytime in the past. If your allergy is not listed, please print only the name of the medication allergy in the bottom section of this chart. Correct way to mark circles: • Please use blue or black ink. Please add last name if different than member Dependent Dependent Dependent First name : Date of Birth (MM/DD/CCYY) :
Penicillin/cephalosporin Antibiotics (e.g.
(NSAIDs) (e.g. ibuprofen, Advil®,Motrin®)
If there is a drug allergy to report and not listed above, please print only the name of the drug in the space. Example : Morphine —————————> Please continue on next page to tell us about any medical conditions. Medco is a registered trademark of Medco Health Solutions. Inc. ™ 2008 Medco Health Solutions, Inc. All rights reserved Group Number Member Number Section 3 : Medical Conditions Please list names of each family member enrolled in the appropriate column. Then for each family member, fill in the circle next to each condition if a doctor ever said that particular family member has any of the following conditions. Spouse/SSDP Dependent Dependent Dependent First name :
High blood pressure (hypertension)
High cholesterol (hypercholesterolemia)
Chronic bronchitis or emphysema (COPD)
Allergies, runny nose, hay fever (allergic rhinitis)
High blood sugar (diabetes) (GERD)
Inflammatory bowel disease (colitis, Crohn's disease)
High pressure in the eyes (glaucoma)
Poor circulation in legs (peripheral vascular
hyperplasia, BPH)
Print other medical conditionsExample : Glaucoma ➺
For more information about Medco, please visit us online
at www.medco.com. Please complete both pages and staple together.Please return the questionnaire with your Medco Delivery form or refill order form. Pay for medications with e-check. It's easy, convenient, and secure!
Medco now offers e-check to easily andconveniently pay for medications.
With e-check, one of the most securepayment methods available today, theco-payment or coinsurance is automaticallydeducted from your checking account. Andyou have a 10-day grace period between thetime we send the order and the day theamount is deducted from your checkingaccount.*
To enroll and authorize Medco, just completethe form on the back and return it with yournext order!
Authorization I authorize Medco to initiate a debit entry to the checking account provided on the back of this form. This authorization permits Medco to charge unpaid balances and future orders made by all covered dependents to my account, based on my authorization provided by mail, phone, or web. On future orders, Medco will include the amount to be charged to my checking account with the order. I acknowledge that the origination of ACH transactions to the account must comply with the provisions of U.S. law. This authorization will remain in effect until I have canceled it.
*Please note that if there are insufficient funds at thetime Medco submits the funds transfer request, Medcowill charge a $10 fee. Your bank also may charge anonsufficient funds fee.
Is Caffeine Addictive?—A Review of the Literature The American Journal of Drug and Alcohol Abuse, 32:493-502, 2006 Informa Healthcare ISSN: 0095-2990 print /1097-9891 online DOI: 10.1080/00952990600918965 Is Caffeine Addictive?—A Review of the Literature Sally Satel, M.D.*1 1Oasis Clinic, American Enterprise Institute. *Correspondence: Sally Satel, M.D., 1150 17th St. NW, Washington, D
STUDENT NAME: ____________________________ 2013-2014 Medications Agreement Each family is required to fill out this form , even if your student is not taking any medications during trips (if this is the case, please read through the below information and see reverse). In the spirit of establishing a system that works for each family, we would like you to choose how you want medications handled




 MEDCO BY MAIL
MEDCO BY MAIL


 Patient/doctor Information continued
Patient/doctor Information continued Health, Allergy & Medication Questionnaire (HMQ)
Health, Allergy & Medication Questionnaire (HMQ)
 Pay for medications with
Pay for medications with