Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Microsoft word - 1981-v10n01-p007.doc
Hyperventilation Syndrome, Treatment With L-Tryptophan and Pyridoxine; Predictive Values of Xanthurenic Acid Excretion. M.J.A.J.M. Hoes, M.D.1, P. Colla2, H. Folgering, M.D., Ph.D.3 Abstract Introduction A case is made for the pathophysiological
The hyperventilation syndrome (HVS) is a
importance of the cerebral serotonergic functional syndrome (van Dis, 1978) caused by neurons in the hyperventilation syndrome
stress (Hermann et al., 1978). Important
(HVS). Their function depends on the systemic
features of the HVS are the increased respir-
ation, the anxiety, and an often occipitocervical
The role of L-tryptophan metabolism is
headache and muscular hypertonia (Hardonk
studied in 13 HVS patients, by administration of pyridoxine 125 mg t.i.d. and L-tryptophan two
The cerebral serotonergic neurotransmission
grams for four weeks. The xanthurenic acid
(CST) is important to these symptoms on the
excretion (XA) is measured as an index of the
basis of the following evidence from animal
peripheral L-tryptophan metabolism, before
experiments: CST activates the inhibition of
treatment. The treatment resulted in freedom of
respiration that is found during an acute alcohol
hyperventilation attacks in nine patients. The
intoxication (Smith et al., 1975) or during
XA was elevated or low in eight and normal in one of the nine responders and normal in the
experimental models of anxiety (Ellison, 1975).
The extremes in the XA excretion had dis-
CST is important in the inhibition of pain
appeared after treatment. Treatment results and
(DeSousa and Wallace, 1977; Hoes, 1979-c).
XA data indicate that the L-tryptophan CST inhibits muscle tone as a result of an metabolism is important in the pathophysiology
inhibition of afferent input (Hoes, 1979-c), a
of the HVS, and that the XA discriminates
stimulation of Ren-shaw interneurons (Meyers-
responders from non-responders to pyridoxine,
monosynaptic reflexes (Clineschmidt and Andersen, 1970). Because of this evidence, underactivity of the CST is proposed as a pathophysiological model for HVS. As a matter
1 Lecturer for Biological Psychiatry, University of
of fact, the effectiveness of clomipramine in
Nijmegen, The Netherlands; Dept. of Psychiatry, Bethesda Hospital, Tiel, The Netherlands. 2 Psychologist, Dept. of
Social Psychiatry, University of Nijmegen. 3 Dept of Physiology, University of Nijmegen.
ORTHOMOLECULAR PSYCHIATRY, VOLUME 10, NUMBER 1,1981, Pp. 7-15
enhancement of the CST (Hoes et al., 1980-
plasma (Fernstrom and Lytle, 1976). The plasma
concentration of L-tryptophan is lowered by a
The CST is dependent on the cerebral syn-
diet short of L-tryptophan, or by increased
thesis of serotonin from L-tryptophan. The
rate-limiting step in this process is the cerebral
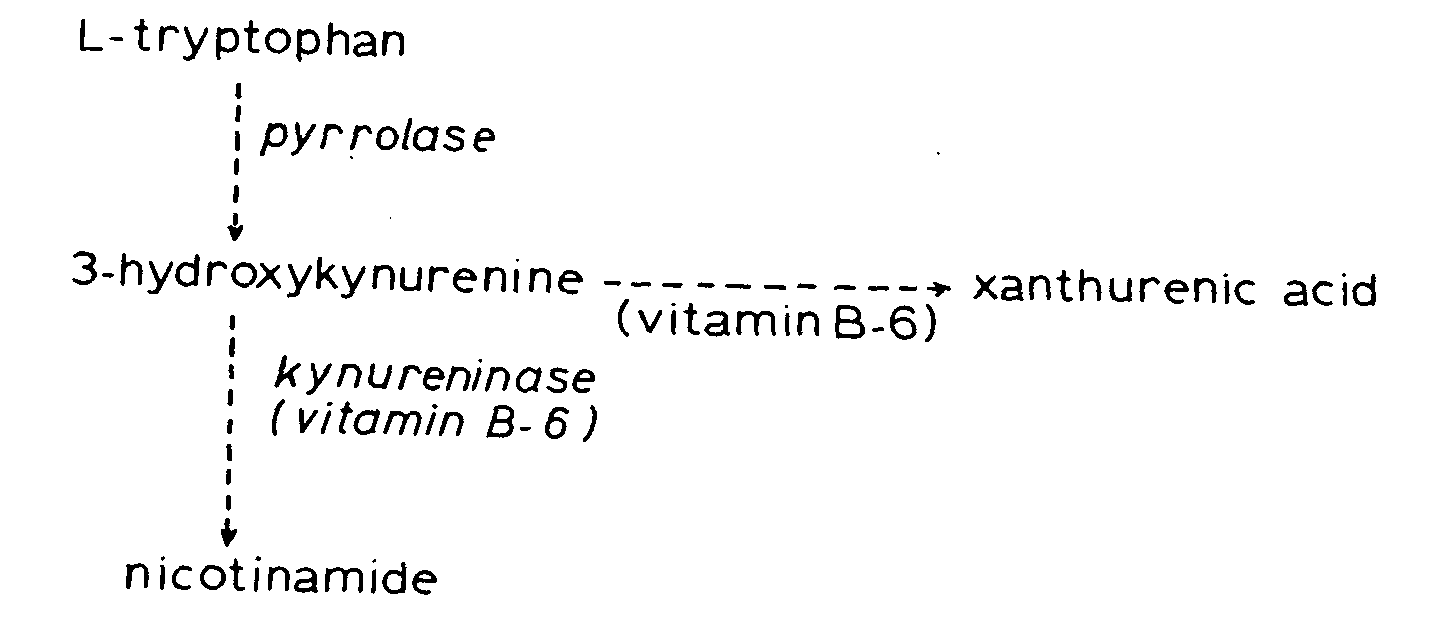
biosynthesis of nicotinamide (NiA) (Figure 1).
L-TRYPTOPHAN-NICOTINAMIDE BIOSYNTHESIS A shorthand version of the nicotinamide biosynthesis. Hypercorticism induces the pyrrolase; enhanced pyrrolase activity will pull more L-tryptophan in this synthesis, activating the pyridoxal-5-phosphate containing enzymes (vitamin B6). This activation by substrate and the induction of other pyridoxal-containing enzymes by hypercorticism, leads to a relative pyridoxal-deficiency. To this pyridoxal-deficiency the kynureninase is the most sensitive enzyme in the nicotinamide biosynthesis. The xanthurenic acid excretion will rise by the enhanced pyrrolase and diminished kynureninase activity. The xanthurenic acid excretion may eventually diminish, only when not enough pyridoxal is available for the mitochondrial transaminase in the xanthurenic acid side-chain, this enzyme being less sensitive to a pyridoxal-deficiency.
A good diet supplies about one gram of L-
pyrrolase; this is notably caused by gluco-
tryptophan a day. Man synthesizes about 12-15
corticosteroids (Green, 1978). This induction of
mg NiA a day. For the synthesis of one mg of
the pyrrolase may engender a considerable loss
NiA, 60 mg L-tryptophan are needed. So, man
of L-tryptophan from the systemic circulation,
needs 720-900 mg of L-tryptophan a day for his
and thus deprive the cerebral serotonin synthesis
NiA synthesis. Two thirds of his daily NiA-
of its mother-substance (Curzon, 1969; Hoes,
requirements are covered by his own synthesis;
the remaining one third is covered by uptake
The functional state of the NiA biosynthesis is
from the food. Thus, the NiA synthesis is the
studied by measuring the urinary excretion of
major metabolic pathway for L-tryptophan in
intermediates such as 3-hydroxyky-nurenine, or
side-chain products such as xanthurenic acid
Increased utilization of L-tryptophan in the
(XA), after oral intake of a loading dose of L-
NiA synthesis is caused by induction of the
XANTHURENIC ACID IN HYPERVENTILATION
1980-b). The excretion of XA in this loading test,
positive feedback in the HVS pathophysiology as
is elevated in anxiety, and this is explained by
long as the anxiety persists. As a matter of fact,
effects of elevated glucocorticoid plasma Lewis (1959) proposed on clinical evidence in his concentrations on the NiA synthesis (Hoes, 1979-
model of sequence of events characterizing the
a). HVS patients are anxious in general, and so
HVS, that apprehension reinforces the HVS
one expects that HVS patients will have an
(Figure 2). The HVS provokes a hypocapnia, the
elevated XA excretion in the L-tryptophan hypocapnia aggravates the HVS symptomatology, loading test.
the perception of these symptoms leads to
When the HVS patients have an elevated XA
apprehension and this apprehension reinforces the
excretion, this indicates that they derive L-
tryptophan from the cerebral serotonin synthesis.
If the peripheral metabolism is that important to
Since underactivity of the CST is proposed as
the pathophysiology of the HVS, then two
pathophysiological mechanism of HVS, an predictions should be investigated: elevated XA excretion indicates a
SEQUENCE OF EVENTS CHARACTERIZING HYPERVENTILATION SYNDROME (after Lewis, 1959). The disorders in the L-tryptophan metabolism facilitate the different steps in the sequence, inducing a positive feedback in the development of the disorder. (See text, under discussion.)
1) In HVS patients the excretion of XA in a
Patients and Methods
Thirteen patients (4f, 9m; age: 34.5+9.2 yrs,
range 22-56 yrs) were selected according to the
HVS criteria specified elsewhere (Folgering and
Colla, 1978). Patients with another psychiatric
a) Correction of the XA-excretion. Pyrid-
diagnosis but anxiety neurosis according to the
oxine 125 mg t.i.d. during four weeks will
Feighner criteria (Feigh-her et al., 1972) were
b) Supplementation of L-tryptophan to contraceptives or other hormones. First, the XA
correct any L-tryptophan-deficiency state. Two
grams of L-tryptophan are sufficient (Hoes, 1979-b). 9
ORTHOMOLECULAR PSYCHIATRY, VOLUME 10, NUMBER 1, 1981, Pp. 7-15
in urine, collected during 24 hours after oral
(28.8±2.2 years) (Table 2). The L-tryptophan
intake of 5 grams of L-tryptophan at 22.00
loading test had to be repeated just in the
hours, as described previously (Hoes, 1979-a;
responders whereas the non-responders excreted
Hoes et al, 1980-b). Then the patients received
normal amounts of XA (Table 3). All checks for
pyridoxine 125 t.i.d. + L-tryptophan 2 g vesp.,
diabetes mellitus were normal in all 13 patients.
both for four weeks, as described previously
The XA-excretion in the responders is high
(Hoes, 1979-a). During the fifth week they were
interviewed about their frequency of attacks and
treatment one high excretor (nr.3) is still high,
HVS symptoms (Folgering and Colla, 1978).
while one low excretor (nr.7) excretes a high
The L-tryptophan loading test was repeated if
amount XA. Because a parametric approach like
abnormal at the first time or if the treatment had
the the t-test, addressed at differences in central
resulted in an absence of attacks for at least the
pathological extreme low and high values, the
At the time of these experiments the only
available reference values of the XA excretion
appropriate (Siegel, 1956). Furthermore the t-test
were those of 648 neurologic and psychiatric
is not permissible be cause the distribution of the
patients. Many of these persons may not have
XA-values of the patient group is evidently non-
suffered any condition influencing the XA normal and there is too great a difference excretion. The XA values are however between the variances of the treatment positively skewed, with a modus of 50 umol/24
responders and the reference group (coefficient
hours and a median 78 umol/24 hours. On the
of variance 1.01 vs 0.25). The pre-treatment val-
basis of the distribution curve, 40-120 umol/24
ues of XA differ significantly from the reference
hours (n=347) was considered normal. Recently
values (p(sh< nc-2h+g)=0.00003). The properly
the XA excretion could be investigated in
different values are exclusively found in the
healthy volunteers, 68.8±19.0 umol/24 hours
responder group. The XA excretion values of the
(n=31), median 70 umol/24 hours, range 82
nine responders after the treatment differ
umol/24 hours (Hoes et al, 1980-b). The significantly from the pre-treatment values determination method of XA by (Moses test: p=0.025), i.e. extreme low and spectrophotometry is accurate (Hoes et al, extreme high values tend to disappear. The post-1980-b).
treatment values do not differ significantly from
During their first visit to the out-patient de-
the reference values, viz. in extreme reactions
partment, all patients were checked for diabetes
mellitus by determination of the fasting plasma-
The nine treatment responders received no
glucose concentration and of glucose and further medication after the four trial weeks; they ketone bodies in the morning urine.
remained symptom-free during a three months
Statistical analysis was performed by Student
t-test and the Moses test of extreme reactions.
Discussion
The patients included in this study suffered
patients studied is small. The data are however
0.5-3 years from HVS, and had at least two
attacks/week during the last two months before
The XA-excretion shows two types of disorder;
it is either too high or too low. Since either
Of the 13 patients, nine were symptom-free
disorder is corrected by the pyrid-oxine-L-
after three weeks of treatment (3f, 6m) and four
tryptophan treatment, the supply of the substrate
were not so (1f, 3m) (Table 1). The mean age of
L-tryptophan is not important to this normalizing
the responders (37.1 ±10.1 years) does not
effect, but the pyridoxine is. Two enzymes are
differ significantly by t-test (p=0.069) from the
relevant, both containing the active principle of
XANTHURENIC ACID IN HYPERVENTILATION
oxal-5-phosphate (PAL), as co-factor (Figure
containing enzymes is induced directly by e.g.
1). These two are the supernatant enzyme
hormones (Schepartz, 1973). In HVS, both
kynureninase and the mitochondrial trans-
mechanisms can occur by enhanced secretion of
glucocorticosteroids. These hormones induce the
enzyme-cofactor (PAL) binding-constant is pyrrolase (Figure 1), the rate-limiting enzyme of weaker for the kynureninase than for the the NiA synthesis; thus more L-tryptophan is transaminase (Adams et al., 1976; Green et al.,
pulled into this synthesis, activating PAL
1978). So, in any PAL disorder, corrected by
containing enzymes (Curzon, 1969; Green,
pyridoxine supplementation, the excretion of
1978), and lowering the PAL levels in serum
XA in a L-tryptophan loading test will first rise
and then fall, compared to the reference values,
glucocorticosteroids induce the synthesis of PAL-
and during more pronounced PAL disorders it
containing enzymes, such as the tyrosine
will fall. The low XA-ex-cretion thus is the
transaminase, tryptophan transaminase, alanine
most pathological of the two XA disorders.
Each disorder in the XA-excretion is caused
decarboxylase. The kynureninase is not induced.
either by competitive inhibition of the PAL
Thus the total body supply of PAL will be
binding sites of the enzymes, or by a PAL de-
lowered. To such PAL consuming activities the
ficiency. Competitive inhibition of PAL bind-
dietary intake will soon yield, because the
ing sites has been described for steroid hor-
required 2 mg a day are just supplied by a regular
mones (Mason et al., 1969). Because the HVS
diet (Bogert et al, 1973). In pyridoxine loading
is a stress disorder, glucocorticoster-oids will
studies 60 percent of a physiological dose of
be hypersecreted (Selye, 1976), intermittently
pyridoxine is recovered in the subsequent 24
during attacks or chronically; however, they
hours urine (Wozenski et al., 1980) and 35
were not measured in this study. But for
percent of a megadose of 750 mg (O'Reilly et
glucocorticosteroids no competitive inhibition
al., 1980). The initial distribution phase of
of the kynureninase has been described in the
pyridoxine and PAL has a t1/2 of two hours; the t
literature. The transaminase has even a more
/2of the elimination phase could not exactly be
stable apo-enzyme-cofactor binding and is computed (O'Reilly et al, 1980). One can better protected in the mitochondrion against
conclude that the body does not have any
competitive inhibition than the supernatant pyridoxine pools of any importance. Thus, a kynureninase. So, in any case, the relative (to the adequate diet) pyridoxine and mitochondrial transaminase will be better PAL deficiency is to be considered the causative protected against the influence of factor for the disordered XA-excretion. The glucocorticosteroids than the kynureninase. plasma concentration of L-tryptophan will be Competitive inhibition in general can also be
lowered as soon as the pyrrolase is induced by the
exerted by metabolic products; thus, the NiA
glucocorticosteroids because thus L-tryptophan
inhibits the pyr-rolase by endproduct inhibition.
will be pulled into the NiA synthesis from the
No inhibition of enzymes by substrate has been
systemic circulation (Curzon, 1969; Hoes, 1980;
described for PAL-containing enzymes in the
Moussaoui, 1978). This is illustrated by the
NiA synthesis, neither by the endproduct NiA
elevated XA-excretion in a L-tryptophan loading
test in women using oral contraceptives (o.c).
The disorder in the XA-excretion must be
They had no confirmative signs of a pyridoxine
deficiency (Adams et al., 1976), and the XA elevation had to be explained by induction of the
The PAL deficiency has not a dietary source,
because the diet of the patients was adequate, supplying the required 2 mg pyridoxine a day
However, Green et al., (1978) measured the
(Bogert et al., 1973). A PAL deficiency occurs
plasma concentrations of L-tryptophan and the
also when PAL-containing enzymes are XA excretion during the same L-tryptophan activated by augmented supply of substrate
(Wynne, 1975), or if the synthesis of PAL-
ORTHOMOLECULAR PSYCHIATRY, VOLUME 10, NUMBER 1, 1981, Pp. 7-15
found an elevated XA excretion but refute an
balance. Patients with an elevated XA excretion can
induction of the pyrrolase as explanation, because
show a diabetes mellitus-like state. This is
they found a comparably large area under plasma
explained either by complex forming of the elevated
tryptophan versus time curve in their patients
XA with insulin, thus inactivating the latter (Rose et
than in controls. But there are two contra-
al., 1975); or by diminished production of
arguments: First, any deficiency of L-tryptophan
quinolinic acid, an intermediary product in the NiA
in the diet can be counteracted by increased
synthesis from below the kynureninase step. Quino-
mobilisation of L-tryptophan from body-protein
linic acid is an inhibitor of the hepatic phos-
(Niskanen et al., 1976). Secondly, in the figure of
phoenolpyruyatecarboxykinase, an important
Green et al., the curve of plasma concentrations
enzyme in the gluconeogenesis (Adams et al.,
of L-tryptophan in the o.c. users stays under that
1976). These hyperglycemic patients can develop a
of the controls! More important is that the plasma
ketosis. A ketosis facilitates the hyperventilation
concentration of L-tryptophan at the end of the
and neuromuscular irritability symptoms. The
absorption phase is in the figure significantly
experience of this reinforcement can evoke
(p<-0.05) lower for the o.c. users than for the
apprehension. The disorder in L-tryptophan and
controls, although Green et al. claim that the area
glucose metabolism is completely restored by pyrid-
under the curve is the same. The difference in
oxine suppletion (Adams et al., 1976; Rose et al.,
the absorption peaks cannot be explained by
1975). This derangement can however induce a
altered elimination kinetics, because the positive feedback, because in animal experiments it descending parts of the curves of controls and
was shown that hyperglycemia induces the
o.c. users run strictly parallel. So, the absorption
described disorder in the NiA metabolism, with
peak differs because L-tryptophan reaches the
enhanced XA excretion (Akarte and Shastri, 1974)!
systemic circulation more slowly in the o.c. users
3) The apprehension can be reinforced by
than in the controls. Altered gut movements or
diminished production of NiA, the ketosis aside.
gut absorption kinetics are not described in o.c.
NiA was shown in recent experiments to possess
users, to account for the difference in L-
benzodiazepine-like action and benzodiazepines are
tryptophan kinetics. The second possibility is the
antianxiety drugs (Mohler et al., 1979). The HVS
first pass effect through the liver. If in o.c. users
patients studied did not show signs of a fullblown
more L-tryptophan is pulled into the liver than in
clinical (Bogert et al., 1973) or subclinical (Green,
controls, this means that the pyrrolase activity in
1973) pellagra. Yet when the patients have a PAL
the o.c. users has been enhanced. Definite separa-
disorder, as proved by the therapeutic effect of the
tion of a pyrrolase-and a PAL effect require the
pyridoxine (and L-tryptophan) suppletion in this
execution of a L-tryptophan and kyn-urenine
study, the production of endogenous NiA (2/3 of the
total requirements) is diminished. Besides, anxiety
The described disorders of the L-trypto-phan-
is a prominent feature of HVS and of subclinical
NiA metabolism can sustain the HVS pellagra. symtomatology in several ways. This is best understood according to the sequential steps in
SEX OF THE HVS PATIENTS
deractive CST is reinforced by the loss of L-
tryptophan from the systemic circulation into the
liver by the pyrrolase pull. When besides the plasma concentrations of kynurenine rise, the
RESPONDERS NON – RESPONDERS
kynurenine may inhibit the cerebral uptake of L-
tryptophan, although this effect probably is small in man (Green, 1978). 2) The next mechanism concerns the acid-base
There is no significant difference by t-test in sex between the patients who responded and who did not respond to treatment. XANTHURENIC ACID IN HYPERVENTILATION
4) As long as the apprehension (and anxiety)
the orthomolecular treatment by pyridoxine and
persist, the elevated glucocorticoster1 oid
secretion will keep the pyrrolase activity underactive CST in the HVS is considerably induced, deriving more L-tryptophan in the
Further study along this line should include L-
substrate keeps the PAL containing enzymes
tryptophan and kynurenine loading tests (Wolf et
hyperactivated, thus further emptying the PAL
al., 1980), determinations of plasma Cortisol
(Selye, 1976) and quantification of respiration
positive feedback is introduced in the L-tryp-
tophan derivation, because the brain is deprived
of steadily more L-tryptophan and the anti-
AGE OF THE HVS PATIENTS
anxiety substances serotonin (Ellison, 1975)
RESPONDERS (9)
In the patients studied, the possibilities two
37.1 10.0
and three are excluded as a reinforcement of the
28.8 2.2 34.5 9.2
HVS, because the fasting glucose levels in
RESPONDERS (4)
plasma were normal and the fasting morning
TOTAL (13)
urine was negative for glucose and ketone bodies. The possibilities one and four reserve however serious consideration in the treatment
There is no significant difference by t-test in age between the patients responded and who did not respond to treatment. The age-range for all patients (N=13) is 22-56
The treatment responder with a normal years.
preteatment excretion of XA, probably has had a disturbed CST in view of his therapeutic response. His normal excretion of XA is either
XANTHURENIC ACID EXCRETION OF HVS PATIENTS
an accidental finding, or the turning point in
XANTHURENIC ACID (XA)
XA excretion from a high to a low excretor of
( umol/24 hrs) RESPONDERS
In the four non-responders to treatment, the
XA excretion was normal. Both findings argue
against a disorder in the L-tryptophan 4
metabolism and the CST. In these patients the
CST was functionally deranged during the HVS
Summarizing, this study shows that there is a
RESPONDERS
peripheral L-tryptophan metabolism. This i
disorder measured by the XA excretion in a L-
tryptophan loading test is however not specific
for HVS patients (Hoes, 1979-a, 1979-b); a low
XA excretion is more pathological than a high
one. Any XA disorder is perfectly correlated
with a favorable response to the pyridoxine + L-tryptophan treatment.
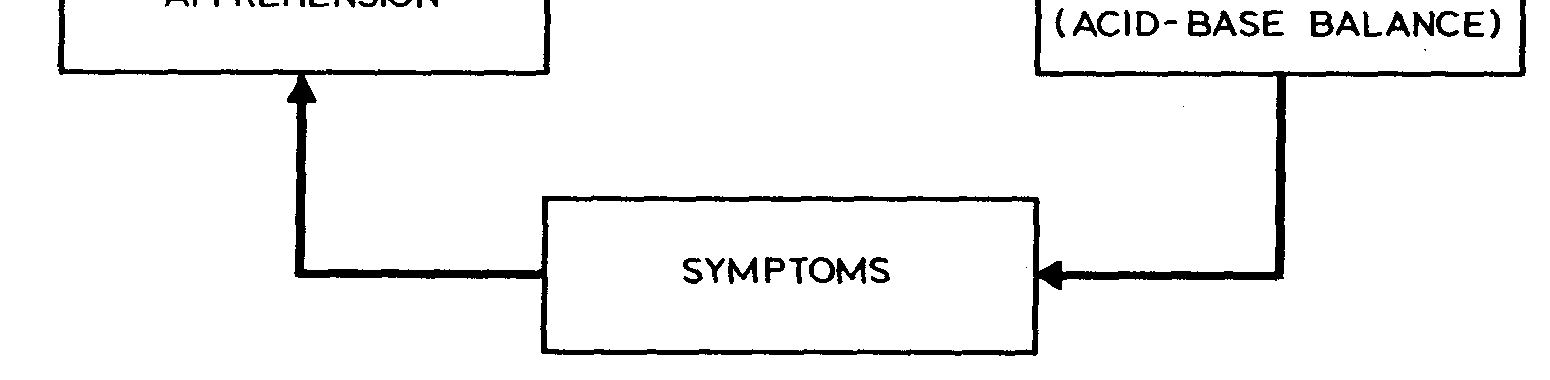
The excretion of XA in 24 hours urine after oral intake of 5 grams of L-tryp- tophan was measured. This was done in all patients before (1) treatment; it was
So, one can conclude that because there are
repeated after (2) treatment, only if it had been abnormal the first time or if the therapeutic response had been favorable. At the time of these experiments the range
HVS patients with a disturbed XA excretion,
of XA excretion considered normal was 40-120 umol/24 hrs. So, the first 5 values in the responder group are elevated, the 6th is normal and the last 3 are low. The non-
and because the XA disorder accurately responders show just normal values. predicts the therapeutic response of the HVS to 13 ORTHOMOLECULAR PSYCHIATRY, VOLUME 10, NUMBER 1, 1981, Pp. 7-15 Statistics:
chosomatischen Medizin, 485-492. Urban und Schwarzenberg, Mun-chen, 1978.
The statistical analysis was performed by P.
Colla and N. Sijben, research psychologist, HOES, M.J.A.J.M.: Pyridoxine, L-Tryptophaan en Zinksulfaat voor Dep-
ressieve Patienten. Tijdschr. Psychiat. 21,301-321,1979-a.
HOES, M.J.A.J.M.: The Clinical Significance of an Elevated Excretion of
Xanthurenic Acid in Psychiatric Patients. Acta Psychiat. Belg. 79, 648-
This paper is an adaption of a lecture delivered
HOES, M.J.A.J.M.: Tolerance and Dependence on Psychoactive Drugs.
at the symposium of the Dutch Hyperventilation
Study Croup, Utrecht, 19 October, 1979, by
HOES, M.J.A.J.M.: L-Tryptophaan en Pyridoxine Huishouding in Depres-
sieve Patienten: Een Serotonine Hypothese voor Corticosteroid Regu-latie en Adaptatie. TGO/J. Drug Res. 5,685-694,1980.
References
HOES, M.J.A.J.M., COLLA, P. and FOLGERING, H.: Clomipramine Treat-
ment for Hyperventilation Syndrome. Pharmakopsychiat.-Neuropsy-
ADAMS, P.W., WYNN. V., FOLKARD, J. and SEED, M.: Influence of
Oral Contraceptives. Pyridoxine (vitamin B6), and Tryptophan on Carbohydrate Metabolism. Lancet 1,759-764,1976.
HOES, M.J.A.J.M., KREUTZEN, E. and SIJBEN, N.: Xanthurenic Acid Ex-
cretion in Urine After Oral Intake of 5 grams of L-Tryptophan by Healthy
AKARTE, N.R. and SHASTRI, N.V.: Studies on Tryptophan-niacin Metab-
Volunteers: Standardization of the Reference Values. Accepted by J. Clin.
olism in Streptozotocin Diabetic Rats. Diabetes 23,977-981,1974.
BOGERT, L.J., BRIGGS. G.M. and CALLOWAY, D.H.: Nutrition and
HOFFMAN, W.S.: The Biochemistry of Clinical Medicine, 787-789 (niacin);
Physical Fitness. 133-142 (niacin), 142-146 (vitamin B6), Saunders,
789-790 (pyridoxine). Year Book, Chicago, 1970.
JOUVET, M.: The Role of Monoamines and Acetylcholine-Containing
CLINESCHMIDT, B.V. and ANDERSEN, E.G.: The Blockade of
Neurons in the Regulation of the Sleep-waking Cycle. Ergeb.z. Physiol.
Bulbospinal Inhibition by 5-Hydroxytryptamine Antagonist. Exp. Brain
LEWIS, B.I.: Hyperventilation Syndrome. A Clinical and Psysiological Eval-
CURZON, G.: Tryptophan Pyrrolase — A Biochemical Factor in Depres-
sive Illness? Brit. J. Psychiat. 115,1367-1374,1969.
MASON, M., FORD, J. and WU, H.L.C.: Effects of Steroid and Nonsteroid
DeSOUSA, C. and WALLACE, R.B.: Pain: A Review and Interpretation.
Metabolites on Enzyme Configuration and Pyridoxal Phosphate Binding.
ELLISON, G.D.: Behavior and the Balance Between Norepinephrine and
MEYER-LOHMAN, J.: Renshaw Cell Activity and Monaoamine Liberation.
Serotonin. Acta Neurobiol. Exp. 35,499-515,1975.
Proc. Int. Union Physiol. Sci. IX, 389,1971.
FEIGHNER, J.P., ROBINS, E., GUZE, S.B., WOODRUF, R.A.,
MOHLER, H., POLC, P., CUMIN, R., PIERI, L. and KETTLER. R.:
WINOKUR. G. and MUNOZ, R.: Diagnostic Criteria for Use in
Nicotinamide is a Brain Constituent with Benzodiazepine-like Actions.
Psychiatric Research. Arch. Gen. Psychiat. 26,57-63,1972.
FERNSTROM, J.D. and LYTLE, L.D.: The Interaction of Diet and Drugs
MOUSSAOUI, D.: Biochimie de la Depression. Analyse de la Literature.
in the Modification of Brain Monoamine Metabolism. In: Usdin, E. and
Forrest, I.S., Eds. Psychotherapeutic Drugs, Volume II, 359-387. Marcel Dekker. New York, 1976.
NISKANEN. P., HUTTUNEN, M., TAMMINEN. T. and JAASKELAINEN,
J.: The Daily Rhythm of Plasma Tryptophan and Tyrosine in Depression.
FOLGERING, H. and COLLA, P.: Some Anomalies in the Control of PA
Co2 in Patients With a Hyperventilation Syndrome. Bull. Europ. Physio-path. Resp. 14, 503-512,1978.
O'REILLY, W.J., GUELEN. P.J.M. HOES, M.J.A.J.M. and VAN DER
KLEYN, E.: HPLC Determination of Pyridoxine and Congeners in Bio-
GREEN, R.G.: Subclinical Pellagra. In: Hawkins, D. and Pauling, L., Eds.
logical Fluids of Man After High Dose Therapy. Biomed. Appl. 183,492-
Orthomolecular Psychiatry, 411 -434. Freeman, San Francisco, 1973.
GREEN, A.R.: The Effects of Dietary Tryptophan and its Peripheral Metab-
ROSE, D.P., LEKLEM, J.E., BROWN, R.R. and LINKSWILLER, H.M.: Ef-
olism on Brain 5-Hydroxytryptamine Synthesis and Function. In:
fect of Oral Contraceptives and Vitamin B6 Deficiency on Carbohydrate
Youdim. M.B.H., Lovenberg, W., Sbarman, D.F. and Lagnado. J.R., Eds.
Metabolism. A. J. Clin. Nutr. 28, 872-878,1975.
Neurochemistry and Neuropharmacology, Volume 3, 103-129, Wiley, New York, 1978.
SCHEPARTZ, B.: Regulation of Amino Acid Metabolism in Mammals.
GREEN, A.R., BLOOMFIELD, M.R., WOODS, H.F. and SEED, M.:
Metabolism of an Oral Tryptophan Load by Women and Evidence
SCHULZ, M., GRIMM, W., SCHMITZ. W. and KNAPP, A.: Tryptophan-
Against the Induction of Tryptophan Pyrrolase by Oral Contraceptives.
stofwechsel-untersuchungen Bei Oligofrenen Kindern. 1 Mitteilung:
Ergebnisse der Kynurenin - und Zanthurensaureausscheidung nach Try-ptophanbelastung und deren Abhangigkeit von der Vitamin B6 Zufuhr.
HARDONK, H.J. and BEUMER, H.M.: Hyperventilation Syndrome. In:
Psychiat. Neurol. Med. Psychol. 25, 98-106.1973.
Vin-ken, P. and Bruyn, G.W., Eds. Handbook of Clinical Neurology, Volume 38,309-360. North-Holland, Amsterdam, 1979.
SIEGEL, S.: Nonparametric Statistics for the Behavioral Sciences. McGraw-
HERMANN, J.M., SCHONECKE, O.W. and VON UEXKULL. TH.: Das
Hyperventilation Syndrome. In: Von Uexkull, Th., Ed. Lehrbuch der Psy-
XANTHURENIC ACID IN HYPERVENTILATION
SMITH, A.A., ENGELSHER, C. and CROFFORD, M.: Modulation of the
Respiratory Depressant Effect of Ethanol by 5-Hydorxytryptamine. J. Phar, Pharmacol. 27, 60-61,1975.
VAN DIS, H.: Hyperventilation in Phobic Patients. In: Spielberger, Ch.D.
and Sarason, I.G., Eds. Stress and Anxiety, Volume 5, 371-373,1978.
WOLF, H., BROWN, R.R. and AREND, R.A.: The Kynurenine Loading
Test, an Adjunct to the Tryptophan Loading Test. Scand. J. Clin. Lab. Invest. 40, 9-14,1980-a.
WOLF, H., WALTER. S., BROWN, R.R. and AREND, R.A.: Effect of
Natural Oestrogens on Tryptophan Metabolism: Evidence for Interference of Oestrogens with Kynureninase. Scand. J. Clin. Lab. Invest. 40,15-22, 1980-b.
WOZENSKI, J.R., LEKLEM, J.E. and MILLER, L.T.: The Metabolism of
Small Doses of Vitamin B6 in Men. J. Nutr. 110,275-285.1980.
WYNN. V.: Vitamins and Oral Contraceptive Use. Lancet 1,561-564,1975.
PHARMACY Max. Marks 100 Attempt all 50 questions, each question carries 02 marks. There is no negative marking. Please mark the correct answer as A/B/C/D at appropriate place, on the right hand side of the question, in blue or black ink. Q.1 Genetically modified species of papaver namely papaver braceatum and papaver oriental Q.2. A β- lactamase inhibitor which contain an 1- Oxopenam s
Antineoplastic drugs - recent developments by John Hammond Cancer is worldwide a healthcare problem affecting one in three people in the developed world, and killing one in four. Worldwide, 12.5 million new cases are diagnosed each year, and this is predicted to reach 15 million by 2020. As a result, the total market for cancer therapies is predicted to reach $55-70 billion by 2010. Comparis
 ORTHOMOLECULAR PSYCHIATRY, VOLUME 10, NUMBER 1,1981, Pp. 7-15
ORTHOMOLECULAR PSYCHIATRY, VOLUME 10, NUMBER 1,1981, Pp. 7-15 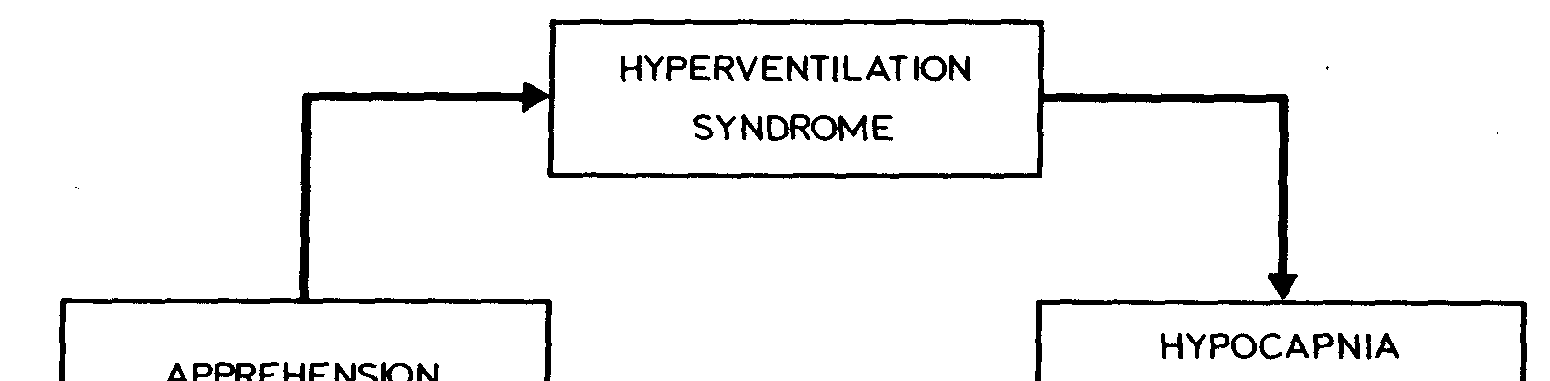
 XANTHURENIC ACID IN HYPERVENTILATION
XANTHURENIC ACID IN HYPERVENTILATION