Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
To be copied
Manual for the New Strategy Female Genital Mutilation - IP - 1. Introduction
Following the 17th session of the United Nations' Working Group on Indigenous Populations held in Geneva (July 26-30, 1999), where the need for effective measures against female genital mutilation (FGM) was discussed, the aim of this manual is to support the efforts to overcome the problems with an entirely new approach. It is apparent that the fight against so-called "female circumcision", a very cruel removal of the clitoris (clitorydectomy), and, in many cases, of the labiae as well, which is predominantly practised in Africa, did not reach the envisaged targets. It is estimated that the number of young girls subjected to this mutilation each year has doubled between 1982 and 1999. The origin of the cruel ritual remains unknown. It has been practised for a long time in parts of Arabia and East Africa but has only more recently arrived in West Africa. This can be deduced from the fact that slaves transported to the Americas up to the 19th century were obviously not familiar with the concept. The tradition is currently reaching Indonesia. The situation in other regions of the world is unclear. There are reports of a similar ritual in southern Africa as well and there is a possibility that it was still practised in South America until recently. According to older estimations, this mutilation was carried out on approximately two million girls annually. Today this rate could be significantly higher. Their age at the time of the procedure varies, according to the tradition, from babies to grown-ups. We are facing a dilemma of cultural customs on the one hand, and human rights aspects on the other. It seems to be the case that respecting one side automatically leads to neglecting the other.
Intervention can be legitimated on medical and psychological
2. An example
In the Third World, it is the upper social classes who are the first to be europeanised. This usually means the irreversible loss of valuable human culture and tradition; but in some ways, this could also have a positive outcome. It can be presumed that in the few cases in which an eradication of FGM has been achieved – in particular in African urban areas – that europeanisation tendencies were at play and that this tradition would also have been abandoned without the use of targeted intervention, since urbanisation is often accompanied by the end of many traditions. Legislative attempts have been made to ban FGM, however, they have only had limited success, as the examples of Guinea, Niger, and Sudan demonstrate. The case of Egypt, where 95 % of women are mutilated, clearly shows the constellation of the problem in a multi-factor setting. Clitorydectomy was so established that it was even carried out in hospitals. As a result of the campaign against FGM, this procedure became officially prohibited in 1996. But what happened then? Was this the end of FGM in Egypt? Unfortunately, that was not the case. As a result of the ban, the procedure was then carried out in barbershops and similar, non-official places. In effect, rusty razor blades led to an increase in complications, and due to the absence of anaesthesia, the tortures multiplied for the victims. In 1997 the ban was lifted and public hospitals continued to mutilate the girls. 3. Cultural Factors
What can we learn from this? Obviously there are cultural factors which have been neglected:
− tradition has proved to be very stable. − there is a demand for a ritual. − unless this demand is fulfilled, there is no solution to the problem.
From a eurocentric position, it is possible to say - and this has actually been done - "We do not accept your tradition. Erase it and become like us". However, we have seen where such ignorance has led us: The problem was not solved, indeed it has even become worse. Cultural determinants are the major obstacles for effective intervention against FGM. Often, those concerned even want the procedure themselves. And in cases where mothers do not want to carry out the ritual on their daughters, the grandmothers enforce it by means of sly tricks. A strategy in the fight against FGM can apparently only then be promising if it manages to overcome these self-maintaining cultural mechanisms. Efforts to ban FGM by law have failed, indeed the problems have become even worse. This suggests the need for a different strategy which takes the cultural system into account. The motivation for carrying out FGM is fuelled by the thorough conviction in the culture concerned that female maturity and coming of age are inevitably linked with such a ritual. It also has to be considered that the women who carry out the mutilations professionally – often, these are the village midwives – do not want to lose their income and therefore strictly oppose any efforts to abolish FGM.
4. The current situation
After having fought FGM for more then a decade, let us ascertain the current situation: Success has been scarce. Even in cities, girls are still being mutilated. Similar to their mothers, they find themselves in an almost schizophrenic position - either, they have to break tradition entirely and also break down social bridges, or they have to surrender themselves to mutilation. There are two necessities in the current situation: (a) there has to be a ritual; (b) mutilation must be stopped. 4.1 The search for a solution
How can this situation, which at first sight appears contradictory, be solved? Rites of passage and initiation can be found in any human society, they only vary in form. Therefore, to begin with, we must accept that there is a ritual at all. As we have experienced, there is little scope for change here. The chance is left to a variation in the form. This obviously is the only promising strategy. But we must be cautious not to vary the procedure too much. If, for example, we suggested that the ritual be replaced by a mere celebration without genital surgery, we can expect a bad reception. Such a suggestion would also overlook the symbolic meaning of the ritual's actions. If we go deeper into detail, we recognise:
− the ritual must concern the clitoris, − some incision has to take place, − it must involve some bleeding.
Unless we accept these traditional requirements, we can not expect success - this is what we have experienced so far. If we compare the situation to male circumcision, it is quite evident that it would also be
considered as totally unacceptable and even ridiculous if someone were to suggest only having a party without real circumcision. Which choices do we have within the framework of the traditional requirements? In order to answer this, it might be useful to take a look at the range of so-called "female circumcision". The extent of the procedure can be quite different from place to place, from culture to culture. The procedure was minimally invasive in the early Muslim setting. The present variations comprise
• a mild form, only affecting the prepuce, • clitoridectomy, i.e. removal of the gland or the entire clitoris, • excision, the removal of the labiae minorae, • infibulation ("pharaonic circumcision") which even affects the labiae
The rare minimal operations which only remove the prepuce of the clitoris are as harmless as equivalent male circumcision. But these are exceptions, and at the other end of the scale, where the entire vulva is afflicted, the mutilation is extremely cruel. In some African cultures, the resulting wound is sewn or stitched with thorns in a very insterile way. Victims of such a mutilation suffer life-long pain and severe infections which can lead to death. However, only 2.5 % of so-called "female circumcisions" are being carried out in a relatively mild form, affecting only the prepuce or small parts of the clitoris. The other 97.5 % represent millions of women who, as a result of severe forms of FGM, are impaired physically as well as psychically - if they survive the mutilation at all. This suffering urgently requires effective intervention.
1 With regard to the equivalent male operation, it is important to remember that circumcision
of the husband drastically reduces the wives' rate of cervical cancer.
5. The new technique
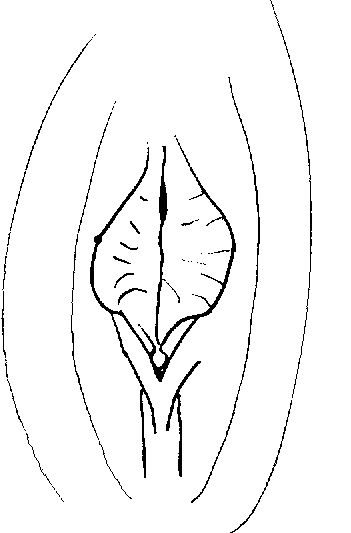
In order to fulfil traditional requirements and yet not to mutilate, the following technique can be expected to offer a solution to the problem. The clitoral hood (praeputium clitoridis) with the gland (glans clitoridis) occasionally showing out of it is situated above the clitoris (fig. 1). This hood is an equivalent to the foreskin of the male penis's gland. The new technique is restricted to this foreskin of the clitoris, nothing is removed, and it leaves the clitoris and labiae unharmed. Figure 1: Schematic view of the female genital with clitoral hood (praeputium clitoridis), gland (glans clitoridis), inner lips (labiae minorae), and outer
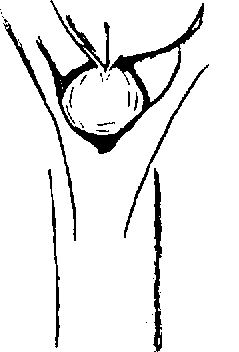
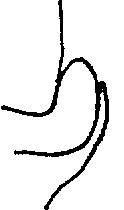
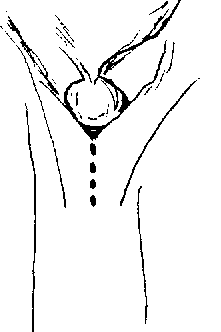
The incision is to be conducted vertically, only opening up the hood, thereby exposing the clitoral gland (fig. 2). To protect the clitoris a suitable blunt instrument can be pushed under the foreskin. The incision can take place after lifting the foreskin from the underside. It is of primary importance to ensure that the clitoris is not damaged itself. In effect, this is neither a circumcision nor a clitoridectomy, but merely an incisio praeputii (incision of the foreskin). Nevertheless, it fulfils the basic traditional requirements of the ritual: There is genital surgery concerning the clitoral region, and there is slight loss of blood. Incidentally, an equivalent procedure in which the upper side of the male foreskin is just slit open can be found in South East Asia.
Figure 2: Alignment of the incision the alignment of the incision (dotted line)
In cases of insistence that tradition strictly requires something be cut off, only the prepuce should be removed. Under no circumstances should the clitoris itself be damaged!
2 Mangyan tradition on the island of Mindoro (Philippines)
There is, however, another aspect which has to be mentioned: The foreskin is frequently so large that the clitoris is even obstructed. When sexually aroused, the clitoris swells and, like the male penis, becomes erect. If the foreskin is large, however, the erect clitoris can disappear behind it. Covered by the hood, the clitoris is less receptive to stimulation. For those many women who are concerned by such predispositions, the new IP (incisio praeputii) method can even be seen as an advantage. Otherwise, they would not be able to fully enjoy clitoral stimulation during sexual intercourse due to the obstruction by a large hood. In effect,
the new method solves a little problem instead of creating a big one.
5.1 Precautions
If available, a local anaesthetic (xylocaine) can be used. However, a cultural-psychological digression is necessary here in order to understand the role of pain. With regard to the meaning of this ritual, the common explanations, such as suppression of women or of their libido, cannot be substantiated. FGM is carried out in regions with religious diversity. Outsiders have difficulties understanding the ritual, and especially since the industrialised world extensively has lost the concept of sacrifice. Sacrifice does not involve something insignificant or superfluous. Sacrifice involves something which is dear and expensive. Incidentally, psychoanalysis attributes the self affliction of pain and injuries to an absence or lack of the father. We might assume that the ritual has a function in the mechanism of the culture concerned. Eliminating the pain completely could therefore probably also block acceptance. The new strategy consists of basically accepting the ritual but reducing it to such an extent that it only involves small skin injuries. However, some points should still be taken into consideration:
• The incision should be carried out with a suitable, clean instrument
• Utmost caution is to be taken not to injure the clitoris itself which is
• Immediately after the cut, the wound is to be disinfected. If no medical
disinfectant is available, alcohol could be used.
• Though healing can be expected within a few days (like for any other
skin injury), fresh air and ventilation must be ensured for the wound.
As there is reason for hope that IP eventually will replace FGM, we cannot afford the risk of infections, especially not during the time of implementation. Those who are suspicious of IP and who thus would rather continue mutilation would use any complications as an argument against the new strategy. 6. Strategic aspects
As we have learned, the mere ban on FGM has not been very successful. Therefore, the implementation of the new IP technique has to follow a different path:
• Instead of prohibiting the ritual, the professionals (these are often old
women and in many cases midwives as well) who are used to carrying out the procedure, thus making their living, shall now be entitled by license - but they are required to carry it out in the NEW way.
• Instead of excluding them from the reformatory process, they shall be
acknowledged and thus embraced to participate in it.
3 The binding together of legs, common practice in some places, should be avoided and
instead fresh air should be guaranteed. It might be worth mentioning that recent modernisation - plastic roofing on the huts instead of traditional leaves - has led to an increase of infections also in male circumcision during the boys' three days of retreat due to insufficient ventilation.
The lesson we have also learned is that if we try to achieve change while ignoring the traditional structures, we risk the mutilations being carried out secretly, "underground", and in non-official places. Making it official means that we keep control over it. The exact diplomacy lies with the local NGOs and activists. They are familiar with details of the respective cultural reality. It might be helpful if the professionals who are to carry out the ritual comply to the new technique publicly in order to bind them by word. Dissemination of the reform is bound to communicative strategies. For that reason, it could also be helpful to demonstrate the new technique in the villages with models of the vulva, or at least with drawings to clarify what is meant and to avoid misunderstanding. Of course, when translated into action, there needs to be some supervision. If possible, it may be beneficial to attend the reformed ritual itself. In discussions with women who are insisting on their tradition, it has proved to be effective to tell them, “God has created woman this way, because that is how He wanted her to be. And now, you destroy what God has created according to His will!” This argument can help to move these people at least not to have their daughters´ (or even their own) clitorises destroyed. In any case, there is a need for control mechanisms:
⇒ It has to be ensured that IP is carried out correctly without any injury
⇒ The girls have to be checked more than once afterwards in order to
intervene in the event of possible infections and the exclude the possibility of mutilation at a later date.
If the reform of the ritual is to succeed, it must be accepted as a full value replacement. In other words: The people concerned must not experience the change as a cultural loss. It has to be made clear - especially to the girls, but also to the other persons involved - that the new, minimally invasive method is a perfect rite of passage and that it achieves the desired initiation completely. 7. Prospects
Carried out officially, the reformed measure would, at least in towns, be shifted into the realm of medicine. Yet, it should be very clear that what is happening in Egypt (see above) is incompatible with medical ethics. Instead of mutilating girls in hospitals, doctors should act responsibly and take the opportunity to put an end to FGM. If official institutions refuse to become involved at all, the mutilations are carried out underground, as we have seen. But if the demand for the ritual is recognised, reform would mean that instead of banning, there would be an offer to carry out the reformed measure officially in hospitals (which would also have a modelling effect on rural areas). As a result, this would mean an end to suffering from mutilation. Instead, there would be positive experiences -
• no damage, but rather a sexual improvement,
• and preservation of cultural identity.
In the long run, this might lead to a complete change in practice.
8. Feedback
In order to optimise this new approach in the fight against FGM, it is very important to implement it in the cultures concerned, to disseminate it, to learn from experience, and to improve details. Therefore, you are very welcome to copy and distribute this manual. Translations into local languages are also urgently needed, as text, as well as audio recordings. Gathering data would be very helpful too, in particular: − about acceptance; − effectiveness of approaching people with the new idea; − diplomacy; − precision of surgery; − conditions of healing; − etc.
If you want to support this reform movement, please send all material (translations, data, photos etc.) to:
Your contribution may then help to improve the next edition of the manual, and to optimise this strategy. Effectively, the aim is to prevent further cruelties. With all the girls who are being mutilated each day in mind, there is no time to waste. Act now!
3rd Edition A. Groh, 1999-2002 This manual may be copied, translated, and distributed, but only as a whole and without changes to the content. If translated, a copy of each translation should be sent to the author’s above address.
BUNDESVERWALTUNGSGERICHT IM NAMEN DES VOLKES hat der 5. Senat des Bundesverwaltungsgerichts auf die mündliche Verhandlung vom 8. November 2012 durch den Vorsitzenden Richter am Bundesverwaltungsgericht Vormeier, die Richterin am Bundesverwaltungsgericht Stengelhofen und die Richter am Bundesverwaltungsgericht Dr. Störmer, Dr. Häußler und Dr. Fleuß für Recht erkannt: Die Revision de
Update on Daubert: What Has It Done to Affect the Right to Jury Trial? Since 1993, when the Supreme Court issued its decision in Daubert v. Merrell Dow Pharmaceuticals, Inc. 1 federal courts have been grappling with how to properly apply the Court’s gatekeeping mandate. Now that many states have adopted Daubert as well, the affect of the Court’s decision has expanded to virtually ev
 5. The new technique
5. The new technique 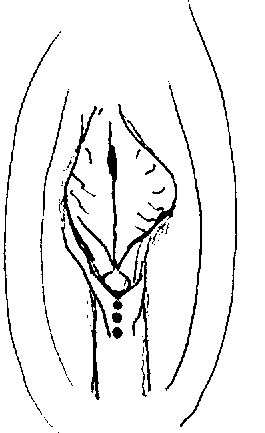
 The incision is to be conducted vertically, only opening up the hood, thereby exposing the clitoral gland (fig. 2). To protect the clitoris a suitable blunt instrument can be pushed under the foreskin. The incision can take place after lifting the foreskin from the underside. It is of primary importance to ensure that the clitoris is not damaged itself. In effect, this is neither a circumcision nor a clitoridectomy, but merely an incisio praeputii (incision of the foreskin). Nevertheless, it fulfils the basic traditional requirements of the ritual: There is genital surgery concerning the clitoral region, and there is slight loss of blood. Incidentally, an equivalent procedure in which the upper side of the male foreskin is just slit open can be found in South East Asia.
Figure 2: Alignment of the incision
the alignment of the incision (dotted line)
In cases of insistence that tradition strictly requires something be cut off, only the prepuce should be removed. Under no circumstances should the clitoris itself be damaged!
2 Mangyan tradition on the island of Mindoro (Philippines)
There is, however, another aspect which has to be mentioned: The foreskin is frequently so large that the clitoris is even obstructed. When sexually aroused, the clitoris swells and, like the male penis, becomes erect. If the foreskin is large, however, the erect clitoris can disappear behind it. Covered by the hood, the clitoris is less receptive to stimulation. For those many women who are concerned by such predispositions, the new IP (incisio praeputii) method can even be seen as an advantage. Otherwise, they would not be able to fully enjoy clitoral stimulation during sexual intercourse due to the obstruction by a large hood. In effect,
the new method solves a little problem instead of creating a big one.
The incision is to be conducted vertically, only opening up the hood, thereby exposing the clitoral gland (fig. 2). To protect the clitoris a suitable blunt instrument can be pushed under the foreskin. The incision can take place after lifting the foreskin from the underside. It is of primary importance to ensure that the clitoris is not damaged itself. In effect, this is neither a circumcision nor a clitoridectomy, but merely an incisio praeputii (incision of the foreskin). Nevertheless, it fulfils the basic traditional requirements of the ritual: There is genital surgery concerning the clitoral region, and there is slight loss of blood. Incidentally, an equivalent procedure in which the upper side of the male foreskin is just slit open can be found in South East Asia.
Figure 2: Alignment of the incision
the alignment of the incision (dotted line)
In cases of insistence that tradition strictly requires something be cut off, only the prepuce should be removed. Under no circumstances should the clitoris itself be damaged!
2 Mangyan tradition on the island of Mindoro (Philippines)
There is, however, another aspect which has to be mentioned: The foreskin is frequently so large that the clitoris is even obstructed. When sexually aroused, the clitoris swells and, like the male penis, becomes erect. If the foreskin is large, however, the erect clitoris can disappear behind it. Covered by the hood, the clitoris is less receptive to stimulation. For those many women who are concerned by such predispositions, the new IP (incisio praeputii) method can even be seen as an advantage. Otherwise, they would not be able to fully enjoy clitoral stimulation during sexual intercourse due to the obstruction by a large hood. In effect,
the new method solves a little problem instead of creating a big one.