Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Om-08-0046 34.37
Termination is not the treatment of choice for severehyperemesis gravidarum: Successful managementusing prednisolone
E Al-Ozairi MBChB MRCP*, J J S Waugh MBBS MRCOG† and R Taylor MD FRCP*
*Directorates of Medicine; †Directorate of Obstetrics, Royal Victoria Infirmary, Queen Victoria Road, Newcastle upon Tyne NE1 4LP, UK
Summary: Severe hyperemesis gravidarum causes profound maternal morbidity. Termination of pregnancy is still offered before
the use of medical therapy. This report describes management of a woman who had undergone two previous terminations for
hyperemesis, and additionally presents the dosage profile of prednisolone used to successfully manage a consecutive series of 33
women with severe hyperemesis gravidarum. The treatment protocol is described. The group had a median weight loss in pregnancy
of 5.5 kg (range 2.0 – 12.5 kg), had been admitted on a median of 3.0 (range 0 – 9) occasions and had spent 7.5 (range 0 – 25) days on
i.v. fluids. Continuing vomiting prevented oral steroid therapy in 14 women and i.v. hydrocortisone (50 mg t.i.d.; two women required
100 mg t.i.d.) was used initially for 24 – 48 h. Nineteen women commenced prednisolone 10 mg t.i.d. and this achieved suppression of
vomiting within 48 h in all but two women who required 15 mg t.i.d. Two distinct subtypes of hyperemesis gravidarum were identified.
Remitting hyperemesis spontaneously ceases between 14 and 22 weeks gestation and accounts for approximately 80% of cases.
In contrast, full-term hyperemesis persists until minutes after delivery. These separate sub-types have not previously been described.
Steroid treatment of hyperemesis should be considered in women who fulfil the criteria of severe disease.
Keywords: hyperemesis, prednisolone, steroid therapy, vomiting, termination of pregnancy
Hyperemesis gravidarum occurs with a range of severity, and
A 28-year-old woman was referred for pre-pregnancy advice
when vomiting is unremitting and unresponsive to standard
about hyperemesis. She had suffered severe hyperemesis
antiemetics, therapeutic termination is sometimes considered.
during her first pregnancy in 2001 with weight loss from
Two small series describing successful therapy using high-dose
72 kg to approximately 58 kg and admission to hospital for
steroids were reported over a decade ago.1,2 A multicentre
i.v. fluids every one to two weeks throughout the pregnancy.
double-blind placebo-controlled one-week trial of prednisolone
Therapeutic termination at eight weeks gestation was advised
therapy in hyperemesis demonstrated significant benefits of
because of severe hyperemesis in both 2003 and 2004. She
steroids with respect to wellbeing, food intake and weight
and her husband were extremely concerned about the prospect
gain at one week, but did not have the power to demonstrate
of frequent hospital admissions and debilitating illness during
effect on readmission.3 Two prospective randomized studies
the planned pregnancy that they very much wanted. She had
have confirmed that steroid treatment is superior to standard
been offered admission during the first 12 weeks of pregnancy
antiemetic therapies.4,5 We have previously reported that
by her local maternity unit. Apart from asthma she was healthy.
steroid therapy is uniformly effective in a consecutive series
Her mother had suffered severe vomiting during pregnancy.
of women with severe hyperemesis as defined by the criterion
She was advised of the high likelihood of occurrence of
of weight loss of .5% of pre-pregnant weight.6 However,
severe hyperemesis in a fourth pregnancy. The effectiveness
knowledge about steroid dosage regimens to achieve control
of high-dose prednisolone in controlling hyperemesis was
of hyperemesis is not widespread. In this report, we describe
described. The potential maternal side-effects of steroids were
successful management of a woman who had undergone two
explained. The lack of clear evidence of side-effects on the
previous terminations for hyperemesis, and document the
baby was discussed. The possibility of requirement for predni-
route and dosage of steroid therapy used in a consecutive five-
solone throughout pregnancy was explained. She wished to
proceed with conception on the basis that prednisolonetherapy would be commenced at the onset of severe nausea. Prednisolone tablets were provided together with writteninstructions to take 10 mg t.i.d. from the time of onset ofsevere vomiting and to telephone for further advice.
She became pregnant within three months and experienced
the onset of nausea and vomiting many times each day at six
Obstetric Medicine 2009; 2: 34 – 37. DOI: 10.1258/om.2008.080046
Al-Ozairi et al. Successful management of hyperemesis using prednisolone
weeks gestation. Prednisolone was commenced as instructed. The vomiting continued and the dose was increased to45 mg, then 55 mg daily over a three-day period. The vomitingthen stopped although nausea continued. By 10 weeks ges-tation, vomiting remained controlled on prednisolone 10 mgt.i.d. Severe nausea persisted and breakthrough vomiting at12 weeks necessitated short-term increase of prednisolone to atotal of 35 mg per day. By 18 weeks gestation she was wellenough to return to work on prednisolone 20 mg daily. Several trials of decreasing the dosage below 15 mg per daywere all followed by return of vomiting and she remained onthis dose for the rest of the pregnancy.
Weight increased from 78.1 kg pre-pregnancy to 82.0 kg at 36
weeks gestation. She did not require hospital admission duringthe pregnancy. There were no obstetric complications and ahealthy baby was delivered at term. Bone densitometry sixmonths post-partum showed a z score in the normal range.
A consecutive series of 33 pregnancies complicated by severehyperemesis were identified in the preceding five years andcase-notes were available for the entire group. Each had beenreferred by her obstetrician to the obstetric medical service
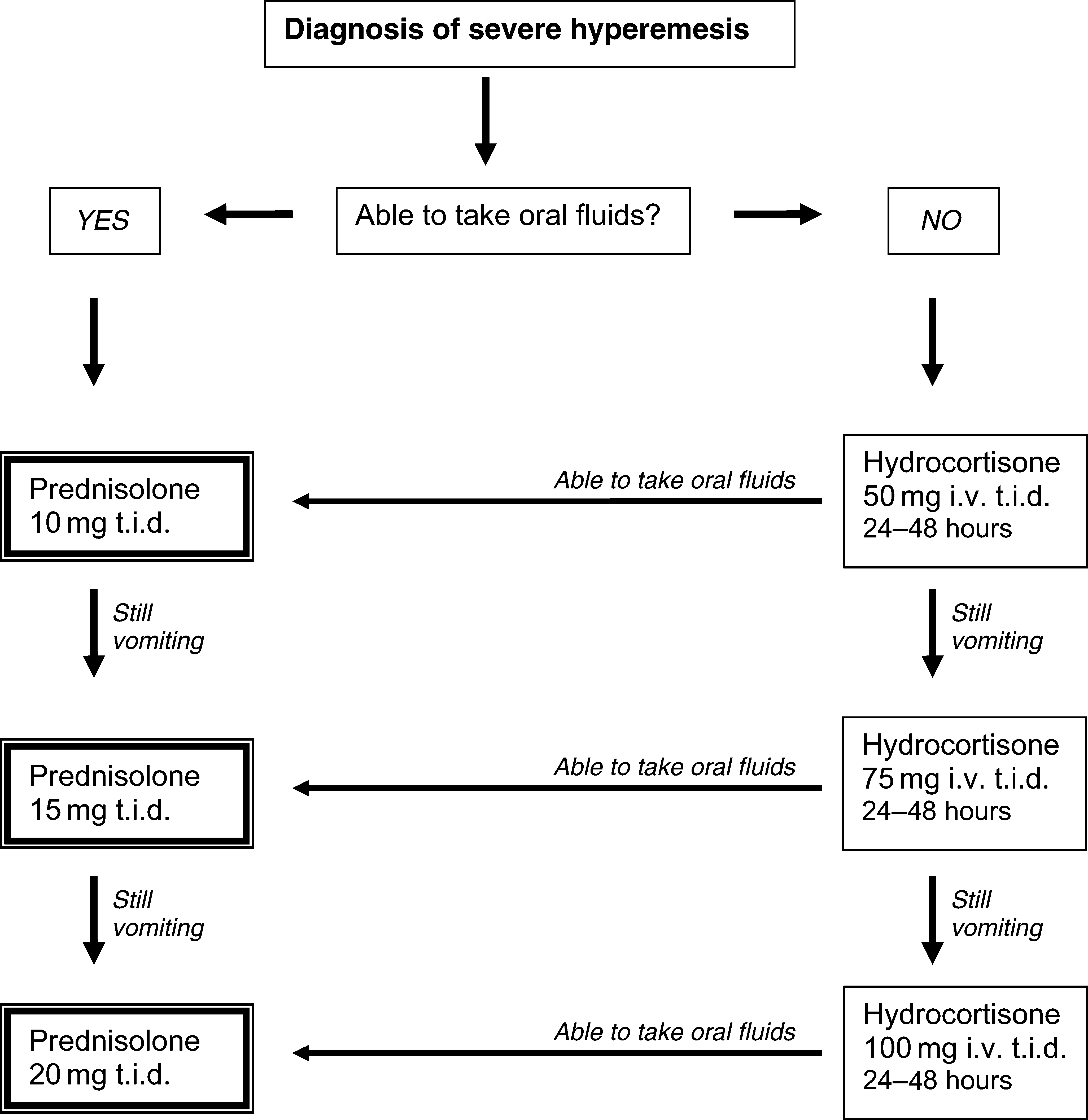
Newcastle guideline for management of hyperemesis.
and was judged to meet the criteria for commencement of
Notes: (1) Initial i.v. fluid should be normal saline with 20 mmol
steroid therapy. The index case is part of the case series. All
potassium. Change to 10% Dextrose with potassium 24 hours
women had received antiemetics without benefit. The severity
after thiamine first given (note that lactate administration usingHartmanns is not optimal and also contraindicated before thia-
of the hyperemesis is reflected by the clinical characteristics.
mine replacement). (2) Vomiting may temporarily settle with
The group had a median weight loss in pregnancy of 5.5 kg
bed rest and i.v. fluids, allowing oral prednisolone to be com-menced. (3) Use ranitidine orally or i.v. if heartburn is present.
(range 2.0–12.5 kg) and had been admitted on a median of
(4) Once vomiting is controlled and food intake has resumed,
3.0 (range 0–9) occasions. The mean duration of i.v. fluid
continue the required dose of prednisolone for 10 days, then
requirement was 7.5 (range 0 –25) days. At the time of referral,
advise decrease every week thereafter by 5 – 10 mg dependingon the degree of wellbeing. If vomiting recurs, go back to
27 of 31 women had marked wasting of leg muscles as shown
immediately previous dose. (5) Prednisolone 1 mg is approxi-
by inability to stand up from a squatting position without use
of arms. There were 28 Caucasian, four Asian and oneAfrican woman. Other clinical features are shown in Table 1.
All women received thiamine prior to use of steroid.
days. Discharge from hospital was usually possible within
Prednisolone or hydrocortisone therapy was administered as
48 hours of oral steroid therapy. Nausea usually persisted to
shown in Figure 1. Continuing vomiting prevented oral
a variable degree and ptyalism, if present, persisted for
steroid therapy in 14 women, and for these women intravenous
several weeks. In one woman ptyalism lasted throughout the
hydrocortisone at a dose of 50 mg t.i.d. was used initially to
pregnancy despite control of vomiting.
control vomiting and this was required for 24 –48 hours. Two
After discharge, the dose of prednisolone was decreased at a
women required hydrocortisone 100 mg t.i.d. to induce remis-
rate of approximately 5 mg per week. Written instructions were
sion of vomiting sufficient to commence oral prednisolone.
provided so that if severe vomiting recurred, a return to the pre-
Nineteen women commenced prednisolone 10 mg t.i.d. and
vious dosage level was undertaken immediately. It was
this achieved suppression of vomiting within 48 hours in all
observed that most women reached a stable dose around
but two women who required 15 mg t.i.d. After control of
15 mg per day and attempts to reduce below this level typically
vomiting, the dose was continued unchanged for seven to 10
led to recurrence of vomiting until the natural history of hyper-emesis had run its course. The nausea remitted with character-istic suddenness between 14 weeks and 22 weeks in mostwomen and, thus, steroid dose could rapidly be decreased
without return of symptoms. This did not occur in six
women who experienced hyperemesis requiring suppression
with prednisolone until term. In the latter women, nausea
remitted within minutes of delivery. There was no difference
in any of the presenting clinical features between those
women whose condition remitted and those with full term
hyperemesis. The dose requirement of prednisolone for each
of these groups of women in relation to gestation is shown in
Figure 2. The median duration of steroid use was eight (4 –20)
weeks in the spontaneously remitting group and 25 (22 –28)weeks in the full-term hyperemesis group.
Steroid therapy has been used for severe asthma and
inflammatory bowel disease for many years, and manystudies have not identified evidence of any harmful effect onthe fetus.12– 17 The transplacental passage of prednisolone islimited to around 10%.18 Some animals are susceptible to orofa-cial clefts after high-dose cortisone.19 Although the study ofRodriguez-Pinilla and Martinez-Frias is often quoted as demon-strating a significant effect of first trimester steroid use and cleftlip and palate, three of the five identified cases appear unlikelyto be relevant.20 One of the three received only two doses of
Change in daily prednisolone dosage (mean + SD) for
the remitting hyperemesis group (n ¼ 27) and for the full-term
prednisolone after eight weeks gestation when lip fusion
hyperemesis group (n ¼ 6). One woman in the remitting group
would have already occurred, another was associated with
required steroids for an unrelated condition in late pregnancy
multiple abnormalities and a third was receiving replacementdoses of hydrocortisone. One of the largest studies (20,820 mal-formed infants) found oral cleft rates to be similar between con-
trols and those taking steroids in the first trimester.21 A recent
Steroid therapy for hyperemesis has been used in Newcastle
study of 1141 babies with cleft lip and/or cleft palate identified
since 1994 and cases prior to the present series have previously
33 cases in which the mother reported use of inhaled, topical or
been reported.2,6 The main purpose of this report is to describe
systemic steroids. Only one case related to use of steroids solely
the expected pattern of prednisolone usage to achieve control of
around the time of lip fusion (5– 7 weeks), although if steroids
symptoms in addition to drawing attention to the possibility of
were reported to have been taken from week one to week eight,
avoiding termination. The case described involving therapeutic
six cases were identified and this was greater than the risk of
terminations for hyperemesis is far from unique and more
orofacial clefts in controls. For women reporting steroid use
widespread recognition of available medical treatment would
only in the four weeks prior to pregnancy there was also an
association. In this study no association was found with iso-
Central to the discussion of management of hyperemesis is
lated cleft palate. The data about use of steroids solely after
the matter of defining severity. The condition manifests a
five weeks duration do not allow clear conclusion about
wide range of intensity, from frequent vomiting but intake of
safety, but any absolute risk of orofacial clefts associated with
some food on most days to life-threatening prostration. We
steroid use must be close to background rates. Using the
have previously suggested that severe hyperemesis is best
same methodology, Carmichael et al.22 have demonstrated
defined by weight loss of .5% of pre-pregnant body weight.6
that stressful events are associated with increased risk of cleft
The present series is based upon this definition, with the excep-
lip and palate, and it has to be considered that the stress of
tion of women who have previously had severe hyperemesis
the underlying illness for which steroids are used may contrib-
and present in a subsequent pregnancy with classical symp-
ute to any excess risk. This clearly indicates that illness itself is a
toms. The definition was chosen as a guide to define a group
potential confounder of any association. Taking all of the pub-
for whom steroid treatment was clearly justified, but should
lished information together, commencing steroid therapy after
be interpreted as part of the overall clinical assessment.
five weeks gestation appears safe. There were no serious maternal
Symptoms are affected by physical movement and the apparent
side-effects of steroid therapy. In particular, no glucose intole-
remission during hospital bed-rest, but recurrence on discharge
rance was observed despite regular postprandial testing and
has reinforced the view quoted in obstetric textbooks that the
no effect on blood pressure was observed. In the present series
condition has a psychological basis.7– 10 Professionals dealing
no women had type 1 diabetes, but we have previously reported
with hyperemesis are sometimes less than sympathetic as
how this may be managed in the context of steroid treatment for
reflected by patient websites (see www.hyperemesis.org.uk;
hyperemesis.23 One woman became acutely depressed on the
initial dose of steriods, but this resolved and maintenance
The characteristic time-course of severe hyperemesis is not
dosage of prednisolone was well tolerated. A degree of steroid
well-recognized. It universally manifests before eight weeks
acne was evident in approximately 20% of women and this
gestation (usually 4– 6 weeks), is at its worst early in pregnancy
and spontaneously remits in over 80% of women between 14
Some exceptions to the general pattern of prednisolone dose
and 22 weeks (remitting hyperemesis). In the remaining
response outside the period of the present case series require
group with full-term hyperemesis, symptoms continue until
mention. Three of approximately 70 women have required pred-
delivery and although symptoms may fluctuate in intensity,
nisolone 60 mg to achieve remission. Very recently, during the
there appear to be no intermediate phenotypes. Remitting
preparation of this report, a single case of hyperemesis failed to
hyperemesis does not relapse in the rest of pregnancy.
respond to high-dose steroid therapy. This is the sole non-
However, full-term hyperemesis requires treatment throughout
responder in our cumulative experience of approximately 100
pregnancy to avoid the return of severe vomiting, dehydration
cases. Subsequently, this woman had a pregnancy with remit-
and weight loss. The two groups were similar in age (median
ting severe hyperemesis, which did respond to steroid
28.9 versus 26.7 years) and gestational age at onset (median
therapy. Hence, although the dose of steroid required to
5.8 versus 5.2 weeks) for remitting and full-term hyperemesis,
induce remission of vomiting does vary, non-response is rare.
respectively; 22/27 and 6/6 women were Caucasian. Previous
The general good care of women with severe hyperemesis
detailed description of the natural history of severe hyperem-
extends beyond the use of steroid therapy. Thiamine replace-
esis is lacking and the present observations allow correction
ment, possibly with other water-soluble vitamins is required
of the textbook definition of hyperemesis as ‘severe vomiting
if vomiting has been prolonged in order to avoid Wernicke’s
encephalopathy.24,25 Deficiency can arise after lack of food
Al-Ozairi et al. Successful management of hyperemesis using prednisolone
intake for several weeks. Thiamine is an essential cofactor for
7 Buckwalter JG, Simpson SW. Psychological factors in the etiology and
critical enzymes of carbohydrate metabolism and it is import-
treatment of severe nausea and vomiting in pregnancy. Am J Obstet Gynecol2002;186:S210 –14
ant that it is replaced before carbohydrate is given. However,
8 Deuchar N. Nausea and vomiting in pregnancy: a review of the problem with
once thiamine has been replaced, provision of calories as i.v.
particular regard to psychological and social aspects. Br J Obstet Gynaecol
10% Dextrose (which provides 400 kcal/L) hastens recovery.
Significant heartburn is frequently caused by the regurgitated
9 Matteson S, Roscoe J, Hickok J, Morrow GR. The role of behavioral
gastric acid and this requires treatment with ranitidine.
conditioning in the development of nausea. Am J Obstet Gynecol2002;186:S239 –43
Finally, mobilization must be gradual as physical movement
10 Uddenberg N, Nilsson A, Almbren PE. Nausea in pregnancy: psychologic and
exacerbates the underlying nausea. Discharge is not wise as
psychosomatic aspects. J Psychosom Res 1971;15:269 –76
soon as i.v. fluids are no longer necessary, as this may be associ-
11 Fagan E. Disorders of the gastrointestinal tract. In: De Swiet M, ed. Medical
ated with loss of control precipitated by the journey home. Full
Disorders in Obstetric Practice. Oxford: Blackwell Science Ltd, 1995:383 –7
12 Fraser FC, Sajoo A. Teratogenic potential of corticosteroids in humans.
and sympathetic explanation of the condition and likely prog-
nosis is also part of routine management.
13 Schaltz M, Patterson R, Zeitz S. Corticosteroid therapy for the pregnant
It has been suggested that total parenteral nutrition or enteral
asthmatic. J Am Med Assoc 1975;233:804 –7
tube feeding can be used in the management of severe hyper-
14 Schatz M, Harden K, Forsythe A, et al. The course of asthma during
emesis.26,27 While these approaches may minimize weight loss
pregnancy, post partum, and with successive pregnancies: a prospectiveanalysis. J Allergy Clin Immunol 1988;81:509–17
and prevent adverse nutritional consequences for the fetus,
15 Schatz M, Harden K, Kagnoff M, Zeiger RS, Chilingar L. Developmental
there are substantial drawbacks. Total parenteral nutrition is
follow-up in 15-month-old infants of asthmatic vs. control mothers. Pediatr
associated with potentially serious hazards including septicae-
mia.28 A naso-gastric tube is uncomfortable and is also associ-
16 Schatz M, Zeiger RS, Harden K, Hoffman CC, Chilingar L, Petitti D. The safety
of asthma and allergy medications during pregnancy. J Allergy Clin Immunol
ated with hazards.29 Both modalities leave the woman in
hospital or at least attached to tubes and are inferior to
17 Vender RJ, Spiro HM. Inflammatory bowel disease and pregnancy. J Clin
steroid therapy in restoring wellbeing.
Steroid therapy achieves remission of vomiting in women
18 Beitins IZ, Bayard F, Ances IG, Kowarski A, Migeon CJ. The transplacental
with hyperemesis severe enough to cause marked muscle
passage of prednisone and prednisolone in pregnancy near term. J Pediatr1972;81:936– 45
wasting and loss of weight. This severity of hyperemesis is
19 Fraser FC, Kalter H, Walker BE, Fainstat TD. The experimental production of
rare, and occurred at a rate of 1.2 per 1000 live-births in our
cleft palate with cortisone and other hormones. J Cell Physiol Suppl
series. The decision to use steroids requires careful discussion
with the individual woman. It is a choice which should be
20 Rodriguez-Pinilla E, Martinez-Frias ML. Corticosteroids during pregnancy
and oral clefts: a case-control study. Teratology 1998;58:2– 5
considered before therapeutic termination of pregnancy.
21 Czeizel AE, Rockenbauer M. Population-based case-control study of
teratogenic potential of corticosteroids. Teratology 1997;56:335 –40
22 Carmichael SL, Shaw GM, Yang W, Abrams B, Lammer EJ. Maternal stressful
life events and risks of birth defects. Epidemiology 2007;18:356 –61
23 Dashora UK, Taylor R. Maintaining glycaemic control during high-dose
None of the authors have any competing interests. This paper
prednisolone administration for hyperemesis gravidarum in Type 1 diabetes.
was presented to the MacDonald Obstetric Medicine Society
24 Lavin PJ, Smith D, Kori SH, Ellenberger Jr C. Wernicke’s encephalopathy:
a predictable complication of hyperemesis gravidarum. Obstet Gynecol1983;62:13s–15s
25 Ohkoshi N, Ishii A, Shoji S. Wernicke’s encephalopathy induced by
hyperemesis gravidarum, associated with bilateral caudate lesions oncomputed tomography and magnetic resonance imaging. Eur Neurol
1 Nelson-Piercy C, de Swiet M. Corticosteroids for the treatment of hyperemesis
gravidarum. Br J Obstet Gynaecol 1994;101:1013–15
26 Christodoulou DK, Katsanos KH, Makrydimas G, Tsanadis G, Tsianos EV.
2 Taylor R. Successful management of hyperemesis gravidarum using steroid
Peripheral parenteral nutrition in protracted hyperemesis gravidarum –report
of two cases and a literature review. Acta Gastroenterol Belg 2008;71:259 –62
3 Nelson-Piercy C, Fayers P, de Swiet M. Randomised, double-blind,
27 Vaisman N, Kaidar R, Levin I, Lessing JB. Nasojejunal feeding in hyperemesis
placebo-controlled trial of corticosteroids for the treatment of hyperemesis
gravidarum – a preliminary study. Clin Nutr 2004;23:53 –7
28 Holmgren C, Aagaard-Tillery KM, Silver RM, Porter TF, Varner M.
4 Bondok RS, El Sharnouby NM, Eid HE, Abd Elmaksoud AM. Pulsed steroid
Hyperemesis in pregnancy: an evaluation of treatment strategies with
therapy is an effective treatment for intractable hyperemesis gravidarum. Crit
maternal and neonatal outcomes. Am J Obstet Gynecol 2008;198:e1 –4
29 Hutchinson R, Ahmed AR, Menzies D. A case of intramural oesophageal
5 Safari HR, Fassett MJ, Souter IC, Alsulyman OM, Goodwin TM. The efficacy
dissection secondary to nasogastric tube insertion. Ann R Coll Surg Engl
of methylprednisolone in the treatment of hyperemesis gravidarum:
a randomized, double-blind, controlled study. Am J Obstet Gynecol1998;179:921 –4
6 Moran P, Taylor R. Management of hyperemesis gravidarum: the importance
of weight loss as a criterion for steroid therapy. Quart J Med 2002;95:153 –8
Printable version: St. Joseph's Church in SoMa will become officesSt. Joseph's Church in SoMa willbecome officesStephanie M. Lee, Chronicle Staff WriterWednesday, February 1, 2012Built nearly a century ago, St. Joseph's Church hasdeteriorated from a stately place of worship into avacant and boarded-up eyesore. In its next incarnation, it could be the hotdestination for technology startu
SOBRE RICARDO GONZALEZ: Nació en Lima, Perú, el 21 de abril de 1974. A raíz de la contundente observación de un ovni en 1988, se interesó profundamente en el fenómeno de los ‘no identificados’. Cinco años más tarde, en 1993, afronta una experiencia de conexión telepática al recibir un ‘mensaje mental’ de supuestas inteligencias extraterrestres. Esta comunicación, que se dio de f
 Al-Ozairi et al. Successful management of hyperemesis using prednisolone
weeks gestation. Prednisolone was commenced as instructed.
Al-Ozairi et al. Successful management of hyperemesis using prednisolone
weeks gestation. Prednisolone was commenced as instructed.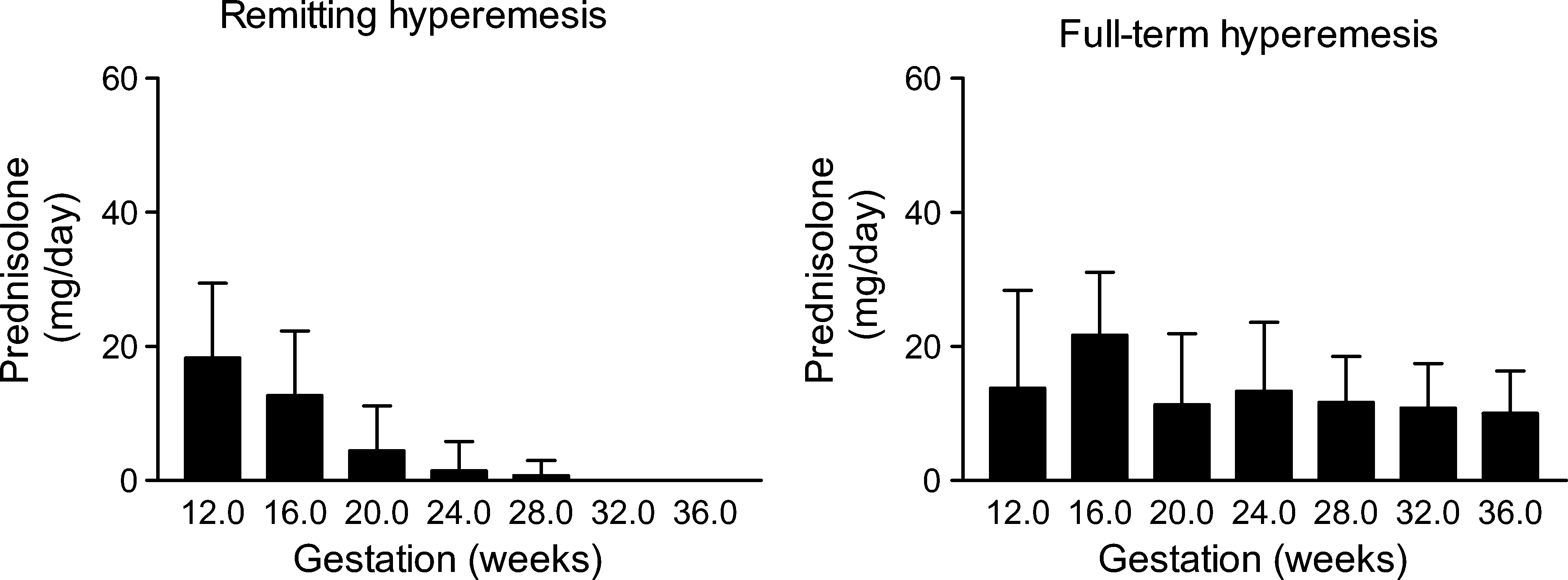 Steroid therapy has been used for severe asthma and
inflammatory bowel disease for many years, and manystudies have not identified evidence of any harmful effect onthe fetus.12– 17 The transplacental passage of prednisolone islimited to around 10%.18 Some animals are susceptible to orofa-cial clefts after high-dose cortisone.19 Although the study ofRodriguez-Pinilla and Martinez-Frias is often quoted as demon-strating a significant effect of first trimester steroid use and cleftlip and palate, three of the five identified cases appear unlikelyto be relevant.20 One of the three received only two doses of
Change in daily prednisolone dosage (mean + SD) for
the remitting hyperemesis group (n ¼ 27) and for the full-term
prednisolone after eight weeks gestation when lip fusion
hyperemesis group (n ¼ 6). One woman in the remitting group
would have already occurred, another was associated with
required steroids for an unrelated condition in late pregnancy
multiple abnormalities and a third was receiving replacementdoses of hydrocortisone. One of the largest studies (20,820 mal-formed infants) found oral cleft rates to be similar between con-
trols and those taking steroids in the first trimester.21 A recent
Steroid therapy for hyperemesis has been used in Newcastle
study of 1141 babies with cleft lip and/or cleft palate identified
since 1994 and cases prior to the present series have previously
33 cases in which the mother reported use of inhaled, topical or
been reported.2,6 The main purpose of this report is to describe
systemic steroids. Only one case related to use of steroids solely
the expected pattern of prednisolone usage to achieve control of
around the time of lip fusion (5– 7 weeks), although if steroids
symptoms in addition to drawing attention to the possibility of
were reported to have been taken from week one to week eight,
avoiding termination. The case described involving therapeutic
six cases were identified and this was greater than the risk of
terminations for hyperemesis is far from unique and more
orofacial clefts in controls. For women reporting steroid use
widespread recognition of available medical treatment would
only in the four weeks prior to pregnancy there was also an
association. In this study no association was found with iso-
Central to the discussion of management of hyperemesis is
lated cleft palate. The data about use of steroids solely after
the matter of defining severity. The condition manifests a
five weeks duration do not allow clear conclusion about
wide range of intensity, from frequent vomiting but intake of
safety, but any absolute risk of orofacial clefts associated with
some food on most days to life-threatening prostration. We
steroid use must be close to background rates. Using the
have previously suggested that severe hyperemesis is best
same methodology, Carmichael et al.22 have demonstrated
defined by weight loss of .5% of pre-pregnant body weight.6
that stressful events are associated with increased risk of cleft
The present series is based upon this definition, with the excep-
lip and palate, and it has to be considered that the stress of
tion of women who have previously had severe hyperemesis
the underlying illness for which steroids are used may contrib-
and present in a subsequent pregnancy with classical symp-
ute to any excess risk. This clearly indicates that illness itself is a
toms. The definition was chosen as a guide to define a group
potential confounder of any association. Taking all of the pub-
for whom steroid treatment was clearly justified, but should
lished information together, commencing steroid therapy after
be interpreted as part of the overall clinical assessment.
Steroid therapy has been used for severe asthma and
inflammatory bowel disease for many years, and manystudies have not identified evidence of any harmful effect onthe fetus.12– 17 The transplacental passage of prednisolone islimited to around 10%.18 Some animals are susceptible to orofa-cial clefts after high-dose cortisone.19 Although the study ofRodriguez-Pinilla and Martinez-Frias is often quoted as demon-strating a significant effect of first trimester steroid use and cleftlip and palate, three of the five identified cases appear unlikelyto be relevant.20 One of the three received only two doses of
Change in daily prednisolone dosage (mean + SD) for
the remitting hyperemesis group (n ¼ 27) and for the full-term
prednisolone after eight weeks gestation when lip fusion
hyperemesis group (n ¼ 6). One woman in the remitting group
would have already occurred, another was associated with
required steroids for an unrelated condition in late pregnancy
multiple abnormalities and a third was receiving replacementdoses of hydrocortisone. One of the largest studies (20,820 mal-formed infants) found oral cleft rates to be similar between con-
trols and those taking steroids in the first trimester.21 A recent
Steroid therapy for hyperemesis has been used in Newcastle
study of 1141 babies with cleft lip and/or cleft palate identified
since 1994 and cases prior to the present series have previously
33 cases in which the mother reported use of inhaled, topical or
been reported.2,6 The main purpose of this report is to describe
systemic steroids. Only one case related to use of steroids solely
the expected pattern of prednisolone usage to achieve control of
around the time of lip fusion (5– 7 weeks), although if steroids
symptoms in addition to drawing attention to the possibility of
were reported to have been taken from week one to week eight,
avoiding termination. The case described involving therapeutic
six cases were identified and this was greater than the risk of
terminations for hyperemesis is far from unique and more
orofacial clefts in controls. For women reporting steroid use
widespread recognition of available medical treatment would
only in the four weeks prior to pregnancy there was also an
association. In this study no association was found with iso-
Central to the discussion of management of hyperemesis is
lated cleft palate. The data about use of steroids solely after
the matter of defining severity. The condition manifests a
five weeks duration do not allow clear conclusion about
wide range of intensity, from frequent vomiting but intake of
safety, but any absolute risk of orofacial clefts associated with
some food on most days to life-threatening prostration. We
steroid use must be close to background rates. Using the
have previously suggested that severe hyperemesis is best
same methodology, Carmichael et al.22 have demonstrated
defined by weight loss of .5% of pre-pregnant body weight.6
that stressful events are associated with increased risk of cleft
The present series is based upon this definition, with the excep-
lip and palate, and it has to be considered that the stress of
tion of women who have previously had severe hyperemesis
the underlying illness for which steroids are used may contrib-
and present in a subsequent pregnancy with classical symp-
ute to any excess risk. This clearly indicates that illness itself is a
toms. The definition was chosen as a guide to define a group
potential confounder of any association. Taking all of the pub-
for whom steroid treatment was clearly justified, but should
lished information together, commencing steroid therapy after
be interpreted as part of the overall clinical assessment.