Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Microsoft word - 077p 9a951749ad1bf0eb8efc3f93e8bb261b.doc
Concept Maps: Theory, Methodology, Technology
Proc. of the First Int. Conference on Concept Mapping
A. J. Cañas, J. D. Novak, F. M. González, Eds.
USING VISUAL CONCEPT MAPPING TO COMMUNICATE MEDICATION INFORMATION TO CHRONIC DISEASE PATIENTS WITH LOW HEALTH LITERACY Lilian H. Hill and Mary M. Roslan, Virginia Commonwealth University, United States
This paper describes the development of an exploratory research project in which medication concept maps are being developed to assist low literate patients to better understand how to take their medications. The correlation between inadequate health literacy and poor health outcomes has been well documented. Research that has explored the use of visual learning for communicating medication information has focused on images such as pictograms that communicate a single idea. It is suggested that individualized medication concept maps, used in conjunction with patient counseling, may be useful to communicate critical medication information and thereby improve low literate patients’ health outcomes.
Introduction
Low functional health literacy has been found to be an independent predictor of medication nonadherence, meaning that patients do not take their medications as prescribed thereby leading to poor health outcomes. There are many reasons why a patient may choose not to follow medication instructions (DiMateo, 2004), but some patients do not understand how to take their medications because they are unable to read the instructions, or in the case of multiple medications, remember them (Baker et al., 1996; Gazmararian et al., 2003; Williams et al., 1995; Youmans & Schillinger, 2003). It is suggested that the use of an individualized medication concept map, in conjunction with patient counseling, may be a tool that could be used to communicate critical medication information to low literate patients.
Background
The prevalence of inadequate functional literacy has been well documented, and it is estimated that as many as 44 million people in the United States have only rudimentary literacy skills and another 50 million have marginal literacy skills (Kirsch et al., 1992; National Work Group on Literacy and Health, 1998). The percentage of the U.K. population with low literacy is similar to that of the U.S., closely followed by Canada, while two European countries, the Netherlands and Sweden, have recorded lower numbers (Houts et al., 2001). Health literacy is commonly defined as the ability to read, understand, and act on health care information, or more formally as “the ability to obtain, process, and understand health information and services to make appropriate health decisions” (Healthy People 2010). People with low health literacy will have difficulty learning information from many written patient education materials because these tend to require higher reading proficiency than many patients possess. They may have difficulty reading medical forms and medication labels, and difficulty with taking their medications correctly. Although health literacy can affect all social classes, it more commonly affects elderly, low income, and minority patients. Low literate patients with chronic physical and mental diseases have been found to be less likely to improve their health (Youmans & Schillinger, 2003).
Research has demonstrated that patients with low health literacy have difficulty with basic medication
instructions. One study found that of 2,659 hospital patients, most of whom had low health literacy, one third gave incorrect explanations regarding “how to take a medication on an empty stomach,” “how many pills of a prescription should be taken,” and “how many times a prescription can be refilled” (William et al., 1995). Low literate patients with asthma were found to have inadequate asthma knowledge and to have poor technique using a metered dose inhaler . Patients with inadequate health literacy have also been found to know significantly less about their disease than patients with adequate literacy (Gazmararian et al., 2003). Baker et al. (1996) found that patients with poor reading ability have problems “accessing the health care system, understanding recommended treatments, and following the instructions of providers.” Among 60 hospital patients determined to have marginal reading skills, many reported having made serious medication errors because they could not read the label on a prescription bottle (Youmans & Schillinger, 2003). Baker et al. (1996) reported that a sense of shame prevents patients with low literacy from disclosing their problem to a health care provider.
In order to navigate the healthcare system and take medications appropriately, “patients are required to read
medical information and comprehend what to do and when to do it. Patients may be required to perform numeric tasks in”cluding calculating the number of tablets for a single dose of medicine. Patients are expected to monitor themselves for both beneficial and adverse effects, know what to do if they miss a dose of medication, and
master when, if, and how to obtain refills of their medication” (Gazmararian et al., 2003). The problem will only continue to grow as patients are asked to assume more responsibility for self-care in a complex health care system.
Pharmacists, as the most accessible health professionals, are in a unique position to identify patients who
struggle with inadequate health literacy and to assist patients in overcoming the barriers that may be limiting their ability to function adequately in the healthcare system (Youmans & Schillinger, 2003). Pharmacists currently use several methods to assist low literate patients with learning how to take medications correctly. One strategy is to draw a symbol (e.g., a red heart for a heart medication) on the label of the prescription bottle and the same symbol on paper accompanied by instructions of how to take the medication. Some medication containers have a mechanism that indicates how often a medication should be taken and there are even ‘talking’ prescription bottles that play a message recorded by the pharmacist for an individual patient. Another strategy sometimes used by pharmacists is to scotch tape actual pills to an instruction sheet. This technique is undesirable because many medications are costly and look very similar. It is unreliable because the pills may not remain attached to the instruction sheet rendering the instructions meaningless. Small children may also find and ingest them.
Many of the articles that document the prevalence and consequences of low health literacy make only brief
references to using pictorial images to communicate health and drug information. There is some evidence that people more easily retain pictorial information than verbal, written information (Doak & Doak; Haber & Myers, 1982). Research that has explored the use of visual learning for communicating medication information has often focused on images such as pictograms that communicate a single idea. Pictograms are effective in stimulating recall of information that was previously learned (Dowse & Ehlers, 2001). Since people’s interpretations of symbolic information can be variable, providing training in the intended meaning for pictograms is advisable (Dowse & Ehlers, 2001). Care must also be taken that the pictograms are culturally appropriate (Mansoor & Dowse, 2003). Other research has compared patients’ comprehension of medical information using pictorial images accompanied by text. For example, Mansoor & Dowse (2003) found that a pictogram accompanying a simplified medication leaflet was preferred by patients over the leaflet with text alone and concluded that pictogram use increased comprehension.
Concept maps can incorporate meaningful pictograms to diagram a flow or hierarchy of ideas. They also
provide written, visual, and spatial information and this combination is more likely to be retrievable from memory than written information alone (Robinson, Robinson, & Katayama, 1999). A visual concept map illustrating daily medication instructions could become a portable tool that a patient could carry with them or post on a bulletin board or refrigerator.
Study Purpose
This study will explore the efficacy of using concept maps for communicating medication treatment information to low literate patients with chronic disease(s). Concept maps, used in conjunction with verbal counseling, may further a patient’s understanding of their medication regimens and therefore potentially improve their medication adherence and improve patients’ health outcomes.
Methods for Study Development
Steps for conducting the study are described below.
A literature review was conducted regarding the use of visual images and pictorial information to communicate health information to low literate patients. Principles for creating appropriate visuals that are recommended by many authors include the following: • Design simple, realistic pictures with limited content using familiar objects and symbols
• Work with the target audience to develop visual images
• Pre-test visual images with the target population
• Be cautious in communicating abstract concepts, especially symbols depicting motion or time
Asthma and diabetes were selected for the development of template concept maps because they are chronic disease states often found in ambulatory care pharmacy practice. Patients with these selected diseases need to master self-care techniques, know how and when to take appropriate action in crisis situations, and, in the case of asthma, differentiate when to take maintenance and rescue medications. Further, the link between low literacy and poor health outcomes has been established for both disease states. An advisory group of pharmacy practitioners approved the selection.
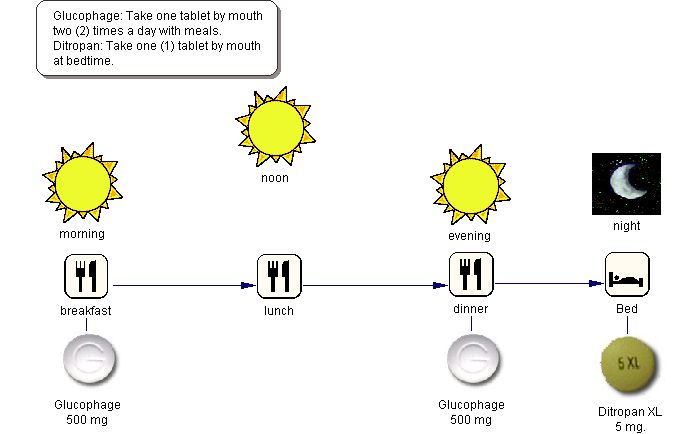
A series of template concept maps are being developed that outline medication treatment steps for the chronic diseases selected. See Figure One and Two for examples. The concept maps will rely primarily on pictorial information including photographs of the actual medications. Written information will be kept to a minimum. These maps are to be used in conjunction with verbal patient counseling and are intended to improve patients’ recall of medication instructions and hopefully their medication adherence. The template concept maps will be reviewed for accuracy by pharmacy faculty before pre-testing with any patients. Inspiration software was used to develop the concept maps. Since graphical software is flexible, the concept maps could be easily tailored for individual patients and updated at each patient visit.
Figure One: Concept Map Illustrating How to Take Glucophage (Antihyperglycemic drug for treatment of diabetes) and Ditropan
(Antispasmodic drug that relieves urinary frequency)
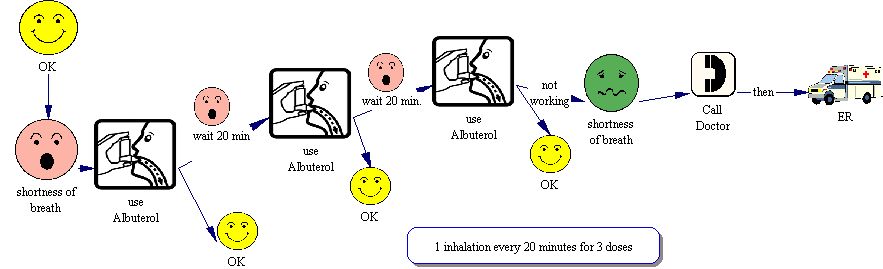
Figure Two: Concept Map Illustrating Use of Rescue Medication for Asthma
A research protocol, including review for Human Subjects Protection, is being written in order to pre-test the use of the template concept maps with a focus group of pharmacy students. Later they will be pre-tested with a focus groups of adults studying literacy, and finally with patients in the ambulatory care setting. Grant funding will be sought to equip ambulatory care pharmacists with laptop computers and color printers so that they can customize the template concept maps for individual patients’ needs. The efficacy of using concept maps for communicating with patients would be determined by tracking whether patients’ understanding of their medication treatment is increased and retained.
Acknowledgements
Travel to this conference is funded in part by a 2004 Inspired Teacher Scholarship for Visual Learning provided by Inspiration Software, Inc.
References
Baker, D. W., Parker, R. M., Williams, M. V., Pitkin, K., Parikh, N. S., Coates, W., & Imara, M. (1996). The
health care experience of patients with low literacy. Archives of Family Medicine, 5(6), 329-334.
Communicating with patients who have limited literacy skills. (1998). Report of the National Work Group on
Literacy and Health. Journal of Family Practice, 46(2), 168-176.
Davies, S., Haines, H., Norris, B., Wilson, J. R. (1998). Safety pictograms: Are they getting the message across?
Applied Ergonomics, 29(1), 15-23.
DiMateo, M. R. (2004). Variations in patients’ adherence to medical recommendations: A quantitative review of
50 years of research. Medical Care , 42, 200-209.
Doak, L. C., Doak, C. C. Pfizer Principles for Clear Health Communication Handbook. Available
http://www.pfizerhealthliteracy.com/improving.html (accessed April 23, 2004).
Dowse, R., Ehlers, M. S. (2001). The evaluation of pharmaceutical pictograms in a low-literate South African
population. Patient Education and Counseling, 45(2), 87-99.
Gazmararian, J. A., Williams, M. V., Peel, J., Baker, D. W. (2003). Health literacy and knowledge of chronic
disease. Patient Education and Counseling , 51(3), 267-275.
Haber, R.N., Myers, B. L. (1982). Memory for pictograms, pictures, and words separately and all mixed up.
Healthy People 2010. Available http://www.cdc.gov/nchs/about/otheract/hpdata2010/abouthp.htm (accessed April
Houts, P. S., Witmer, J. T., Egeth, H. E., Loscalzo, M. J., Zabora, J. R. (2001). Using pictographs to enhance
recall of spoken medical illustrations. Patient Education and Counseling, 43, 231-242.
Kirsch, I. S., Jungeblut, A., Jenkins, L., Kolstad, A. (1992). Adult Literacy in America: A First Look at the Findings of the National Adult Literacy Survey. Washington DC: National Center for Education Statistics, U.S. Department of Education.
Mansoor, L. E., Dowse. R. (2003). Effect of pictograms on readability of patient information materials. The Annals of Pharmacotherapy, 37(7-8), 1003-1009.
Robinson, D.H., Robison, S.L., Katayama, A.D. (1999). When words are represented in memory like pictures:
Evidence for spatial encoding of study materials. Contemporary Educational Psychology, 24, 38-54.
Youmans, S. L., Schillinger, D. (2003). Functional health literacy and medication use: The pharmacist’s role.
The Annals of Pharmacotherapy, 37, 1726-1729.
Williams, M. V., Parker, R. M., Baker, D. W., Parikh, N. S., Pitkin, K., Coates, W. C., Nurss, J. R/. (1995).
Inadequate functional health literacy among patients at two public hospitals. Journal of American Medical Association, 274(21), 1677-1682.
Woodworm Killer Safety Data Sheet Product Identification Trade Name: Description: Aqueous blend of non-ionic surfactants and insecticide. Hazardous Ingredients Component CAS Number Classification Hazard Identification Irritating to eyes. May cause sensitisation by skin contact. Environmental: Very toxic to aquatic organisms. May cause long-term adve
MIT Department of Biology: H. Robert Horvitzhttp://web.mit.edu/biology/www/facultyareas/facresearch/horvitz. Home Faculty and Areas of Research H. Robert Horvitz OVERVIEW Medical InstitutePh.D. 1974, Harvard Universitytransduction, cell lineage, cell fate, and morphogenesis, with some emphasis on nervous system development. Study ofthe cellular and molecular
 Asthma and diabetes were selected for the development of template concept maps because they are chronic disease states often found in ambulatory care pharmacy practice. Patients with these selected diseases need to master self-care techniques, know how and when to take appropriate action in crisis situations, and, in the case of asthma, differentiate when to take maintenance and rescue medications. Further, the link between low literacy and poor health outcomes has been established for both disease states. An advisory group of pharmacy practitioners approved the selection.
A series of template concept maps are being developed that outline medication treatment steps for the chronic diseases selected. See Figure One and Two for examples. The concept maps will rely primarily on pictorial information including photographs of the actual medications. Written information will be kept to a minimum. These maps are to be used in conjunction with verbal patient counseling and are intended to improve patients’ recall of medication instructions and hopefully their medication adherence. The template concept maps will be reviewed for accuracy by pharmacy faculty before pre-testing with any patients. Inspiration software was used to develop the concept maps. Since graphical software is flexible, the concept maps could be easily tailored for individual patients and updated at each patient visit.
Figure One: Concept Map Illustrating How to Take Glucophage (Antihyperglycemic drug for treatment of diabetes) and Ditropan
Asthma and diabetes were selected for the development of template concept maps because they are chronic disease states often found in ambulatory care pharmacy practice. Patients with these selected diseases need to master self-care techniques, know how and when to take appropriate action in crisis situations, and, in the case of asthma, differentiate when to take maintenance and rescue medications. Further, the link between low literacy and poor health outcomes has been established for both disease states. An advisory group of pharmacy practitioners approved the selection.
A series of template concept maps are being developed that outline medication treatment steps for the chronic diseases selected. See Figure One and Two for examples. The concept maps will rely primarily on pictorial information including photographs of the actual medications. Written information will be kept to a minimum. These maps are to be used in conjunction with verbal patient counseling and are intended to improve patients’ recall of medication instructions and hopefully their medication adherence. The template concept maps will be reviewed for accuracy by pharmacy faculty before pre-testing with any patients. Inspiration software was used to develop the concept maps. Since graphical software is flexible, the concept maps could be easily tailored for individual patients and updated at each patient visit.
Figure One: Concept Map Illustrating How to Take Glucophage (Antihyperglycemic drug for treatment of diabetes) and Ditropan