Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Untitled
Acta chir belg, 2006, 106, 647-653 Liposuction : Review of the Techniques, Innovations and Applications O. Heymans, P. Castus, F. X. Grandjean, D. Van Zele
Department of Plastic, Reconstructive and Aesthetic Surgery, University Hospital Sart-Tilman Liège, Belgium
Key words. Liposuction ; lipoplasty ; aesthetic surgery. Abstract. Liposuction is currently the most frequently performed aesthetic operation in the world. Despite its wide- spread popularity, it should nevertheless be stated that it is not trivial surgery, not always benign and not as safe as inti- mated in the glossy office brochures. Since the initial description of liposuction, numerous changes have taken place. Today, surgical indications are well defined and the liposuction procedure is well codified. However, several surgeons and manufacturers have developed new equipment and techniques. We propose to survey all the techniques showing the real place of each of them. Their advantages and disadvantages will be discussed. The various techniques dealt with are : the wetting solution techniques, standard liposuction or Suction-Assisted Lipoplasty (SAL), internal Ultrasound- Assisted Liposuction (iUAL), VASSER assisted liposuction, external Ultrasound-Assisted Liposuction (eUAL), Laser- Assisted Liposuction (LAL), Power-Assisted Liposuction (PAL) and Vibroliposuction (VL). On the basis of this review of the literature and of our clinical experience, we conclude that VL is the safest, most effective and precise surgery that can be used in any of the modern indications for liposuction. We concluded that VL seems to have all the advantages and none of the disadvantages associated with iUAL. Introduction Indications and Patient Selection
Liposuction is currently the most frequently performed
The best results are still obtained when treating moder-
aesthetic operation in the world. Despite its widespread
ate localized fat deposits in a normal-weight patient
popularity, it should nevertheless be stated that it is not
which cannot be managed by diet and exercise (Fig. 1).
trivial surgery, not always benign and not quite as safe as
At the present moment, the key to success is the capaci-
intimated in the glossy office brochures. Mortality and
ty of the skin to redrape on the new adipose tissue shape,
morbidity related to liposuction procedures still exist
in order to avoid surface irregularities and wrinkles due
to skin excess. This important property has to be evalu-
The first surgical procedure was performed, by
DUJARRIER in 1921. He used a uterine curette to remove
Although a smooth, young and tight skin is a desir-
fat from the knees of a well-known ballerina, with a dis-
able criterion in patient selection, patients with less elas-
astrous outcome. In the 1960s SCHRUDDE removed sub-
tic or older skin, skin wrinkling or multiple fine irregu-
cutaneous fat deposits through stab incisions by sharp
larities (cellulite) may also benefit from liposuction and
curettage (3). In 1978 KESSELRING added strong suction
more specifically from superficial liposuction inducing
to this sharp curettage method (4). Shortly after, ILLOUZ
replaced the curette by a blunt cannula inserted subcuta-
Good health is a basic requirement for aesthetic body
neously and connected to a vacuum pump to aspirate the
contouring procedures. Failure to screen out patients
fatty tissue (5). He also proposed irrigation of the sub-
whose health is suboptimal is one of the important con-
cutaneous space with a hypotonic saline solution in the
tributing factors to serious morbidity following liposuc-
belief that the fat cells would swell and rupture, but this
tion. Most surgeons agree that liposuction is NOT a
process has never been confirmed clinically.
weight loss technique (7). However, it can be used for
In the past decade, many innovations have been made
patients who far exceed ideal body weight, but the results
and the anatomy and physiology of the fatty tissue have
are less dramatic, although very helpful in improving the
been studied in ever greater depth. Modern innovations
fit of clothing in problem areas, such as the hips.
in suction lipectomy include the superwet and thetumescent wetting techniques, Ultrasound–Assisted
General Aspects
Aspiration (UAL), VASSER, Laser-Assisted Lipo-suction (LAL), Power Assisted Liposuction (PAL) and
Numerous changes have taken place in the original tech-
nique of suction lipectomy. The original large, sharp,
with less danger of penetration or neurovascular bundledamages. The distal aperture should be positionedbehind the tip ; this has the advantage that skin can belifted by the tip of the cannula without direct subcuta-neous fat removal. Multiple holes increase the efficien-cy of fat removal, resulting in fewer passes of the can-nula and less tissue trauma.
As regards the diameter of the cannula, no single
diameter suits all anatomic areas. Originally, traditionalliposuction was performed using very large cannulas(10 mm) which had to be kept in the deep fat to avoidsurface irregularities. With the advent of smaller cannu-las (2-3 mm) and different tip configurations, surgeonscan work closer to the skin without creating noticeable
irregularities and perform liposuction of areas of sparsefat deposits. After superficial liposuction treatment of
2,500 patients, Gasperoni describes good aesthetic
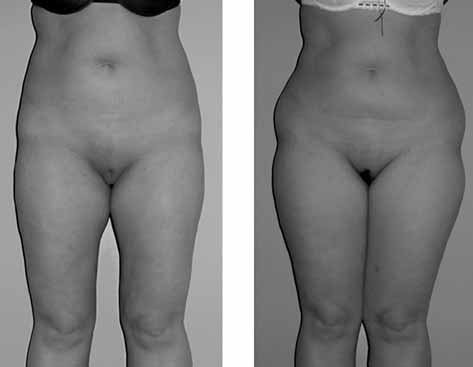
A. This is an excellent case for limited liposuction of fat
results on patients with “old and less elastic skin”. A
deposits located at the top of the thighs and on the hips, with
skin retraction, following the superficial removal of fat
excellent skin quality ; B. At 6 months post-operativesmoother curves can be observed with excellent skin retraction
deposits would be responsible for these results (8).
However, most authors agree on the fact that cellulitis isnot a good indication for liposuction. As a general rule,large, deep fat deposits should be treated with large-
single-hole cannulas were replaced by smaller cannulas
diameter cannulas (5-6 mm), and small, superficial fat
with blunt tips and multiple holes (Fig. 3). Sharp tips are
deposits should be treated with small-diameter cannulas
more likely to penetrate the fascia or skin, whereas a
(3-4 mm). Facial suction requires cannulas of only 1.5-
rounded tip permits easy movement through the tissues
A. This is not a good candidate for liposuction. The skin is of poor quality, aged, hardened, striated with wrinkles and poor retrac-tion capacity ; B-C. When the patient is young, with a skin of excellent quality, an good cutaneous covering retraction can be expect-ed and significant liposuction can be carried out with no risk.
The cannula most often used with the Lipomatic® is size 4,with a foam end and multiple holes. The nutation movementsof the head and the multiple holes make for optimum fatremoval during a cannula pass.
This is a perioperative view of the subcutaneous tissue being
The stab incisions into the skin are placed adjacent to
lipoaspirated with the Lipomatic®. The cannula pass removesthe fat while respecting the fascio-neuro-vascular structures.
the area to be treated, concealed in a natural fold. Theincisions should be slightly longer than the cannuladiameter to avoid skin trauma and burns. Liposuctioncreates a discontinuous cavity or multiple small cavities.
attempted to induce swelling and hydrolysis of in vivo
More accurately the treated area is characterized by a
fat cells, i.e., “lypolysis” (5). There remains no clinical
fascia-neurovascular-lymphatic framework from which
evidence to support this action mechanism, and the use
of hypotonic saline has fallen into disfavour. The use of
After infiltration, the cannula is inserted for suction-
saline infiltration, however, gained popularity, and by
ing. Keeping the tip in the central deep fat permits con-
the early 1980s the majority of surgeons were using the
tour reduction, leaving the superficial fat undisturbed to
wet technique. They infiltrated 200 to 300 cc of saline,
provide smooth, soft cover above the treated area. If
with or without additives (Lidocaine and Adrenaline),
superficial liposuction is planned, it will be performed
into a surgical area. These two techniques were both
after the deep fat liposuction. However, some anatomic
abandoned because of excessive blood loss, the suction
areas may only have a single, thin fatty layer, so the sur-
aspirate containing 20-45% of blood in the dry tech-
geon has to direct the tip immediately below the skin
nique (9-11) and 4-30% in the wet technique (12).
New solutions appeared with the superwet tech-
Before concluding the procedure, the edges have to
nique (13, 14) and the tumescent technique (15), which
be palpated in the search for lumps and abrupt steps
dramatically improved the safety of liposuction. The
from treated to untreated areas. If present, smoothing
superwet technique is defined as 1ml of infiltrate per
can be performed by removing small amounts of fat in
1 ml of aspirate. The tumescent technique is defined as
the transition zone using a fine-diameter cannula.
2-3 cc of infiltrate per 1cc of aspirate. In these methods,
General guidelines call for a halt when skin flaccidity
the subcutaneous fat is infiltrated with large volumes of
precludes secondary shrinkage. The final contour will
a mixture of lidocaine, adrenaline, sodium bicarbonate
not be determined by the amount of fat removed, but
and normal saline before fat removal. Blood loss
rather by how much is still in place at the end of the
dropped to 1 percent of the aspirate, which allows a larg-
er volume of fat to be safely aspirated (14). Anotheradvantage is the reduced need for intravenous adminis-
Wetting solution techniques
Lidocaine may be used at dosages higher than those
The terminology relating to infiltration of the subcuta-
listed in the standard references (7 mg/kg or 500 mg
neous fat before liposuction includes : the dry, the wet,
maximum doses). Several studies have shown that much
the superwet and the tumescent technique. The dry and
larger doses can be used safely. PITMAN has injected up to
wet techniques are now of historical interest only. In the
2000 mg of dilute lidocaine and epinephrine over 10 min-
dry technique, liposuction was performed without the
utes without any problems (16), KLEIN used doses of
addition of subcutaneous solution injection (9). The wet
35 mg/kg with the tumescent technique (17) and BURK
technique was introduced by ILLOUZ in 1984 and
28 mg/kg (18). Rohrich believes that 35 mg/kg is the safe
consisted of injecting hypotonic saline solution. He
limit for liposuction with the tumescent technique (14).
Epinephrine induces vasoconstriction, improving
that this technique causes enhanced contraction of the
haemostasis, delays absorption of the anaesthetic agent,
prolongs its effect to four times as long, decreases the
At the present time this technique is suffering from
amount needed and reduces the risk of lidocaine toxici-
increased operating time with similar volume fat
ty. It is recommended that 0.7 mg/kg not be exceeded,
removal compared with conventional lipoplasty (21). A
although doses as high as 10 mg already have been used
number of complications are also associated with this
technique : skin loss (19, 22), seroma with rates as high
There is still no consensus regarding the optimal
as 50% in the initial experience in the USA (23), and
composition and amount of subcutaneous infiltration
peripheral nerve injury (24). KARMO et al. showed that
solution for safety or for optimal aesthetic results. With
blood loss using the iUAL is slightly higher even if sub-
these techniques, the focus has shifted from hypovo-
clinical (25). IGRA et al. were unable to show a difference
lemia prevention to the prevention of fluid over-
in the postoperative course or the final cosmetic result
load (15). The risk of fluid overload and congestive heart
when comparing the SAL and iUAL techniques (26).
failure seems to be lower with the superwet technique.
After initial enthusiasm for iUAL, many surgeons have
There are no proofs in the literature supporting advan-
now rejected this technique. They asserted that the poten-
tages, with respect to safety and efficacy, when ratios
tial benefits do not outweigh its greater cost, need for
training, and increased risk of complications. The longterm consequences of iUAL are also unknown. Internal Ultrasound-assisted lipoplasty (iUAL)
Fodor stated that the operating time is longer (+ 40%)
and longer incisions are needed (21). Moreover, rigid
Some additional pieces of equipment are required for
cannulas are needed (making for difficulty in passing
iUAL, compared with the SAL (19). As a minimum,
around the body curves) which are expensive due to the
these devices include an ultrasonic generator that con-
need for frequent replacement (one single cannula : 20 h
verts the standard electricity supply into high-frequency
life, 1,000 USD !). Skin protection is essential, in the
electrical energy. The generator is connected to a surgi-
cal handpiece, which contains a piezoelectric crystal that
The incidence of skin slough or necrosis has been
converts electrical energy into a mechanical vibration. A
reported to be as high as 4%-6% (19). While some
titanium probe (solid or hollow) attached to the hand-
authors like ZOCCHI (20) advocate a superficial iUAL to
piece amplifies these vibrations and transmits it to its tip,
stimulate the dermis and enhance skin retraction, others
which produces alternately reduced and increased pres-
like Maxwell abandoned aggressive iUAL because of
sure in the surrounding fluid of the adipose tissue. This
process causes a “cavitation process” which induces adi-
The incidence of seroma is definitely higher after
pose cell wall rupture. The triglyceride released com-
iUAL, compared with the negligible rate associated with
bined with the tumescent solution and the interstitial
fluid form a stable fatty emulsion in the subcutaneous
HOWARD et al. (24) examined the sensory changes
space. This emulsion can be removed with low-vacuum
after iUAL. Their analysis showed that recovery time
suction and small diameter cannulas.
appeared to be longer (10 weeks) compared with SAL
The iUAL is a three-step process (19). First the sub-
(6 weeks). Indeed, the neurosurgical literature has docu-
cutaneous fat is infused. The second step consists of fat
mented the injurious effects of ultrasound energy on
emulsification with the probe vibrating at ultrasound fre-
peripheral nerves (27, 28). The potential for ultrasound
quency. The third step is the evacuation of emulsified fat
energy causing damage to peripheral nerves suggests
by lipoaspiration. An aspiration function can be incor-
that the risks of using iUAL in arms, legs, neck and face
porated in the probe (hollow) to remove as much aspi-
may outweigh any potential benefits. HOWARD et al. (24)
rate as possible while energy is being applied to emulsi-
recommend caution when considering iUAL in the ex-
fied fat (19). The two cardinal rules of utmost impor-
tremities and in anatomic areas containing nerves. They
tance in iUAL to prevent thermal injury are that the
found a direct correlation between the amplitude (gener-
ultrasound energy must be applied in a wet environment
ator setting), number of passes made, and degree of
and the probe must always be kept in motion.
injury, noted both grossly and by walking track analysis.
This technique, conceived by Zocchi in the late
Fortunately, the frequency of these complications
1980s (20), has been promoted as an ideal method for
associated with iUAL has steadily decreased thanks to
the extraction of large volumes of fat with minimal
greater operator experience and the use of lower ultra-
fatigue to the surgeon, minimal blood loss, little or no
sonic energy levels for shorter periods of time. Many
bruising, and exceptional control of contour (19, 20).
surgeons believe that it produces results superior to
Difficult fibrous areas such as the male breast and back
those obtained with SAL for large-volume removals,
are especially well treated (19). It has been suggested
fibrous areas, and repeat operations (19, 20, 21, 29, 30). VASSER (Sound Surgical, Denver, Colo.)
off bloodlessly. APFELBERG et al. concluded in their mul-ticentre study that there was no clear and significant
The search for an improved iUAL device has led to the
benefit to be gained from LAL over conventional lipo-
introduction onto the market of the VASSER–Assisted
suction (35). The disadvantages are the slightly cumber-
Liposuction (21). Adjustments have been made to render
some and awkward equipment, and the fact that experi-
the device safer. Only small-diameter solid probes (2.9
ence in laser use is essential. Safety glasses are neces-
and 3.7 mm) are used and require much less ultrasound
sary, the procedure is noisy and constant cooling is
energy than the traditional iUAL systems currently used.
required. The only advantages are greater ease and less
Grooves near the tip are added to increase fragmentation
efficacy. The VASSER still liquefies fat, but the risk of
Neira used the Low-Level Laser-Assisted Lipoplasty
thermal injury (from end blows and at the insertion site)
(LLLAL) in 2000 (36). Low-level laser therapy is
is reduced. In many ways, this new technology is more
defined as treatment with a dose rate that causes no
like power-assisted lipoplasty than traditional internal
immediate detectable temperature rise in the treated tis-
ultrasound-assisted lipoplasty. However, skin protection
sue and no macroscopically visible changes in tissue
(ports and wet towels) is still needed.
structure (36). The LLLAL consists of the tumescentliposuction technique with the external application of a
External-UAL (eUAL)
cold laser (635 nm and 10 mW intensity for a 6-minuteperiod) through the skin. They demonstrated that exter-
External ultrasound application was introduced by
nal lower-level laser associated with tumescent infiltra-
Silberg in 1998 (31). Immediately after injecting the
tion of the subcutaneous tissue produces a transitory
tumescent fluid, the ultrasonic energy transducer is
pore in the adipocyte membrane (99% of the adipocytes
placed on the area. Moderate pressure is used to help
after 6 minutes of laser exposition), preserving the inter-
energy delivery to the deeper fat and a slow continuous
stitium and the capillaries in particular. This allows fat to
motion of the transducer must be maintained (31).
move from inside to outside the cell, placing it in the
According to his preliminary report, the advantages of
interstitial space. The release of fat by suction is facili-
this technique were that more fat could be removed in a
tated, surgical trauma is diminished, ecchymosis or
significantly shorter period of time, and the fat was
hematoma is reduced and patient recovery is fasten-
whiter and of a looser consistency. There was less resis-
ed (36). However in 2004, BROWN et al. analyzed the
tance to the movement of the canula, less bruising, and
effect of low-level laser therapy on abdominal
less post-operative swelling and discomfort (31). These
adipocytes before lipoplasty procedures and their results
results have been confirmed by other investigators (7,
did not bear out the effect of low-level laser therapy on
Nearly all the complications associated with iUAL
A third innovative laser technique is the use of a
are avoided. Silberg reported one case of post-operative
pulsed Nd-YAG laser beam (1064 nm) delivered via an
seroma, but otherwise no skin slough or nerve lesions
optical fibre of only 300 micrometers inserted in a 1 mm
(which are induced by direct contact of the probe in the
cannula. After lipolysis, the liquid fat is suctioned by a
iUAL) were reported (7, 31-33). The large incisions
3 mm cannula. Proposed indications are flaccid areas,
required for internal ultrasound liposuction were no
small areas, secondary liposuction and difficult
longer necessary (33) and good skin retraction was also
cases (38). KUWAHARA showed that the ultra short stress
observed (33, 34). Gasperoni considers external ultra-
waves generated can mechanically cavitate fat in vitro
sound as an ideal complementary procedure to superfi-
without significant damage to adjacent structures (39).
cial subdermal liposuction, since the eUAL permits amore uniform aspiration of the subdermal fat layer, mak-
Powered Assisted Liposuction
ing skin retraction even more effective (33).
The notion of PAL was first introduced by Charles
Laser-Assisted Liposuction (LAL)
Gross, an American surgeon (40). The original motordesign provided for a rotating blade within the cannula.
Different kinds of LAL have recently been developed
Recently, several manufacturers have introduced sys-
and some are still at the experimental stage. An initial
tems that drive the cannula using a power source. These
type of LAL has been tested by Apfelberg (35). The
systems rely on electricity or are gas-driven. A small,
operator inserts the cannula (special design, single-
variable-speed motor generates a reciprocating motion
holed, 4-6mm diameter), activates the suction, and then
(forward and backward) in the cannula to produce a
depresses the foot pedal to activate the laser. The nega-
2 mm to 4 mm excursion at the tip. The mechanism
tive suction draws the fat globule into the hole of the
action is due to a jackhammer-type movement of the
cannula where the laser beam (YAG laser 40W) shears it
cannula tip which breaks up fat, and the fat aspirated
into the cannula openings is avulsed by the reciprocating
insulin lipodystrophy, lymphedema and axillary hyper-
motion. FODOR and VOGT (41) found that the two proce-
dures were comparable with respect to complications,
It is also used in open procedures. As shown in the
speed of recovery, and aesthetic results, and PAL was
figure 4, removal of the fatty tissue around the neu-
superior in terms of ease of fat removal. In addition, the
rovascular bundles creates a pseudo-plane facilitating
aspirate from suction-assisted and power assisted
tissue mobilisation with maximal safety. This allows
lipoplasty are similar, and powered cannulas do not pro-
improved healing and faster sensitivity recovery than
duce more bleeding than SAL when the tumescent tech-
with the usual undermining. This property, combining
nique is used (41, 42). According to COLEMAN (42), PAL
defatting and respect for the neurovascular structures, is
has all the advantages and none of the disadvantages
used in abdominoplasty (46), bodylift (47), concentric
associated with iUAL. Vibration and noise are the only
medial thigh lift (48), breast reduction (49, 50) and bra-
disadvantages of this technique. SCUDERI et al. (43) com-
pared iUAL, PAL and SAL. PAL is said to be a handy
Extravasation injuries, which may induce important
technique, with the most favourable cost-benefit ratio,
sequelae, can be managed by liposuction. Contrast solu-
and seems to be the best option for busy liposuction
tion or chemotherapeutic drugs in the subcutaneous
practices or fast office procedures.
tissue lead to necrosis and retraction. Performed imme-diately after the accident, soft tissue necrosis rarely
Vibroliposuction (VL)
Vibroliposuction represents a development of the PAL
Conclusion
concept. In this system, the cannula is activated by airpressure, producing a complex movement of the tip.
Liposuction is currently the most frequently performed
This movement, combining antero-posterior, supero-
aesthetic operation in the world. Despite its widespread
inferior and parasaggital displacement is called “nuta-
popularity, it must be practiced with maximum care and
tion”. The amplitude of this movement depends on the
safety. Over time, many changes have taken place in the
cannula length and diameter as well as the pressure
instrumentation and new techniques have been intro-
entering the handpiece. A recent publication by
duced. A number liposuction techniques are currently in
REBELO (44) describes this technique.
use but our preference is for vibroliposuction. Fat
A study conducted in our department showed that
extraction is easier, even in fibrous region or in sec-
vibroliposuction is more efficient than SAL. It removed
ondary operations and the lymphatic and neurovascular
40% more fat than SAL under the same conditions.
structures encountered are respected. Thanks to the
After centrifugation of the aspirated fat, the pure fat
more efficient fat extraction, less cannula passes are nec-
fraction was 70% greater than in the SAL.
essary, reducing morbidity. Local traumas and surgeon
The use of VL in our daily practice has shown that
fatigue are diminished. This results in safe, effective and
this procedure is safe. Complications were even fewer
precise surgery that can be used in any of the modern
than with our previous use of SAL. We had no seromas
indications for liposuction, from precise and superficial
and local hematomas were reduced. This technique is
aspiration in extravasation injury to massive fat aspira-
less traumatic because fat extraction is more efficient
needing fewer passes of the cannula. VL respects thelymphatic vessels and neurovascular bundles. The com-bination of VL and open procedures showed the neuro-
References
vascular structures to have been left intact, in themeshed tissue, and hematomas were fewer, compared
1. KLEIN J. A. Deaths related to liposuction. N Engl J Med, 1999,
341 : 1002-3.
2. HANKE C. W., COLEMAN W. P. 3rd Morbidity and mortality related
In conclusion, this technique allows easier tissue pen-
to liposuction. Questions and answers. Dermatol Clin, 1999, 17 :
etration and causes less fatigue to the surgeon.
3. SCHRUDDE J. Relation of plastic surgery to corrective dermatology. Arch Klin Exp Dermatol, 1964, 219 : 676-88. Applications
4. KESSELRING U. K., MEYER R. A suction curette for removal of
excessive local deposits of subcutaneous fat. Plast Reconstr Surg,
Liposuction is not only an aesthetic tool. Non-cosmetic
1978, 62 : 305-6.
5. ILLOUZ Y. G. Body contouring by lipolysis : a 5-year experience
applications have continued to improve since the intro-
with over 3000 cases. Plast Reconstr Surg, 1983, 72 : 591-7.
duction of the technique. Although the most common
6. SMALLS L., LEE C. Y., WHITESTONE J., KITZMILLER W. J.,
use is lipoma removal, liposuction has also been used for
WICKETT R. R., VISSCHER M. O. Quantitative model of cellulite :Three-dimensional skin surface topography, biophysical charac-
benign symmetric lypomatosis, flap defatting, gynaeco-
terization, and relationship to human perception. J Cosmet Sci,
mastia, breast reduction, buffalo hump, hypertrophic
2004, 56 : 105-120.
7. ROHRICH R. J., BROUGHTON G. 2nd, HORTON B., LIPSCHITZ A.,
32. GASPERONI C., SALGARELLO M. The use of external ultrasound com-
KENKEL J. M., BROWN S. A. The key to long-term success in lipo-
bined with superficial subdermal liposuction. Ann Plast Surg,
suction : a guide for plastic surgeons and patients. Plast Reconstr
2000, 45 : 369-73. Surg, 2004, 114 : 1945-52.
33. MENDES F. H. External ultrasound-assisetd lipolasty from our own
8. GASPERONI C., SALGARELLO M., EMILIOZZI P., GARGANI G.
experience. Aesthetic Plast Surg, 2000, 24 : 270-274.
Subdermal liposuction. Aesthetic Plast Surg, 1990, 4 : 137-42.
34. ROSENBERG G. J., CABRERA R. C. External ultrasonic lipoplasty : an
9. FOURNIER P. F., OTTENI F. M. Lipodissection on body sculpturing :
effective method of fat removal and skin shrinkage. Plast Reconstr
The dry procedure. Plast Reconstr Surg, 1983, 72 : 598-609. Surg, 2000, 105 : 785-91.
10. CLAYTON D. N., CLAYTON J. N., LINDLEY T. S., CLAYTON J. L. Large-
35. APFELBERG D. B. Results of multicenter study of laser-assisted
volume lipoplasty. Clin Plast Surg, 1989, 16 : 305-12.
liposuction. Clin Plast Surg, 1996, 23 : 713-9.
11. COURTISS E. H., CHOUCAIR R. J., DONELAN M. B. Large-volume
36. NEIRA R., ARROYAVE J., RAMIREZ H., ORTIZ C. L., SOLARTE E.,
suction lipectomy : An analysis of 108 patients. Plast Reconstr
SEQUEDA F., GUTIERREZ M. I. Fat liquefaction : effect of low-level
Surg, 1992, 89 : 1068-79.
laser energy on adipose tissue. Plast Reconst Surg, 2002, 110 :
12. ROHRICH R. J., BERAN S. J., FODOR P. B. The role of subcutaneous
infiltration in suction-assisted lipoplasty : A Review. Plast
37. BROWN S. A., ROHRICH R. J., KENKEL J., YOUNG V. L., HOOPMAN J.,
Reconstr Surg, 1997, 99 : 514-9.
COIMBRA M. Effect of low-level laser therapy on abdominal
13. FODOR P. B., WATSON J. P. Wetting solutions in ultrasound-assisted
adipocytes before lipoplasty procedures. Plast Reconstr Surg,
lipoplasty. Clin Plast Surg, 1999, 26 : 289-93.
2004, 113 : 1796-804.
14. ROHRICH R. J., KENKEL J. M., JANIS J. E., BERAN S. J., FODOR P. B.
38. BADIN A. Z., MORALES L. M., GONDEK L., CHIARATTI M. G.,
An update on the role of subcutaneous infiltration in suction-
CANTA L. Laser lipolysis : flaccidity under control. Aesthetic Plast
assisted lipoplasty. Plast Reconstr Surg, 2003, 111 : 926-7. Surg, 2002, 26 : 335-9.
15. KLEIN J. A. Tumescent technique for local anesthesia improves
39. KUWAHARA K., GLADSTONE H. B., GUPTA V., KIREEV V., NEEL V.,
safety in large-volume liposuction. Plast Reconstr Surg, 1993, 92 :
MOY R. L. Rupture of fat cells using laser-generated ultra short
stress waves. Lasers Surg Med, 2003, 32 : 279-85.
16. PITMAN G. H. Tumescent technique in liposuction. Plast Reconstr
40. GROSS C. W., BECKER D. G., LINDSEY W. H., PARK S. S.,
Surg, 1995, 95 : 612-3.
MARSHALL D. D. The soft-tissue shaving procedure for removal of
17. KLEIN J. A. Tumescent technique for regional anesthesia permits
adipose tissue. A new, less traumatic approach than liposuction.
lidocaïne doses of 35mg/kg for liposuction. J Dermatol SurgArch Otolaryngol Head Neck Surg, 1995, 121 : 1117-20. Oncol, 1990, 16 : 248-63.
41. FODOR P. B., VOGT P. A. Power-assisted lipoplasty (PAL) : A clin-
18. BURK R. W. 3rd, GUZMAN-STEIN G., VASCONEZ L. O. Lidocaine and
ical pilot study comparing PAL to traditional lipoplasty. Aesthetic
epinephrine levels in tumescent technique liposuction. PlastPlast Surg, 1999, 23 : 379-85. Reconstr Surg, 1996, 97 : 1379-84.
42. COLEMAN W. P. 3rd .Powered liposuction. Dermatol Surg, 2000,
19. MAXWELL G. P., GINGRASS M. K. Ultrasound-assisted lipoplasty :
26 : 315-8.
A clinical study of 250 consecutive patients. Plast Reconstr Surg,
43. SCUDERI N., PAOLINI G., GRIPPAUDO F. R., TENNA S. Comparative
1998, 101 : 189-202.
evaluation of traditional, ultrasonic, and pneumatic assisted
20. ZOCCHI M. Ultrasonic liposculpturing. Aesthetic Plast Surg, 1992,
lipoplasty : analysis of local and systemic effects, efficacy, and
16 : 287-98.
costs of these methods. Aesthetic Plast Surg, 2000, 24 : 395-400.
21. FODOR P. B. Personal experience with ultrasound-assisted lipo-
44. REBELO A. Power-assisted liposuction. Clin Plast Surg, 2006, 33 :
plasty : a pilot study comparing ultrasound-assisted lipoplastywith
traditional lipoplasty. Plast Reconstr Surg, 2004, 113 : 1852-4.
45. COLEMAN W. P. 3rd. Noncosmetic applications of liposuction.
22. BUSSEIN R., MAILLARD G. F. Skin necrosis after ultrasound lipoly-
J Dermatol Surg Oncol, 1988, 14 : 1085-90.
sis. Ann Chir Plast Esthet, 1997, 42 : 281-2.
46. LE LOUARN C. L., PASCAL J. F. High Superior tension abdomino-
23. COMMONS G. Presented at University of California at San
plasty. Aesth Plast Surg, 2000, 24 : 375-381.
Francisco Aesthetic Surgery Symposium, March, 1997.
47. LE LOUARN C. L., PASCAL J. F. Remodeling bodylift with high lat-
24. HOWARD B. K., BERAN S. J., KENKEL J. M., KRUEGER J., ROHRICH R.
eral tension. Aesth Plast Surg, 2002, 26 : 223-30.
J. The effects of ultrasonic energy on peripheral nerves : implica-
48. LE LOUARN C. L., PASCAL J. F. The concentric medial thigh flap.
tions for ultrasound-assisted liposuction. Plast Reconstr Surg,
Aesth Plast Surg, 2004, 28 : 20-3.
1999, 103 : 984-9.
49. LEJOUR M., ABBOUD M., DECLETY A., KERTESZ P. Reduction of
25. KARMO F. R., MILAN M. F., SILBERGLEIT A. Blood loss in major
mammaplasty scars : from a short inframammary scar to vertical
liposuction procedures : a comparison study using suction-assist-
scar. Ann Chir Plast Esthet, 1990, 35 : 369-79.
ed versus ultrasonically assisted lipoplasty. Plast Reconstr Surg,
50. MATARASSO A., COURTISS E. H. Suction mammaplasty : the use of
2001, 108 : 241-7.
suction lipectomy to reduce large breasts. Plast Reconstr Surg,
26. IGRA H., SATUR N. M. Tumescent liposuction versus internal ultra-
1992, 87 : 709-17.
sonic-assisted tumescent liposuction. A side-to-side comparison.
51. LE LOUARN C. L., PASCAL J. F. Brachioplasty. Aesth Plast Surg,
Dermatol Surg, 1997, 23 : 1213-8.
2005, 29 : 423-9.
27. RIDDERHEIM P. A., VON ESSEN C., ZETTERLUND B. Indirect injury to
52. LILLIS P. J. Liposuction of the arms. Dermatol Clin, 1999, 17 :
cranial nerves after suregery with Cavitron ultrasonic surgical
aspirator (CUSA). Acta Neurochir, 1987, 89 : 84-6.
53. VANWIJCK R., LENGELE B. Liposuction as a help for radiologists.
28. YOUNG W., COHEN A., HUNT C. D., RANSOHOFF J. Acute physiolog-
Technical note. Ann Chir Plast Esthet, 1994, 39 : 744-9.
ical effects of ultrasonic vibrations on nervous tissue. Neuro- surgery, 1981, 8 : 689-94.
29. PERES J. A., VAN TETERING J. P. Ultrasound-assisted lipolasty : a
review of over 350 consecutive cases using a two-stage technique.
Service de Chirurgie Plastique et Maxillo-faciale
Aesthetic Plast Surg, 2003, 27 : 68-76.
30. TEBBETTS J. B. Minimizing complications of ultrasound-assisted
lipoplasty : an initial experience with no related complications. Plast Reconstr Surg, 1998, 102 : 1690-7.
31. SILBERG B. N. The technique of external ultrasound-assisted
lipoplasty. Plast Reconstr Surg, 1998, 101 : 552.
Complementary Health Practice Review 000(00)Greetings, and thank you for publishing with SAGE Publications. Your article has beencopyedited, and we have a few queries for you. Please address these queries when you send yourproof corrections to the production editor. Thank you for your time and effort. Please assist us by clarifying the following queries:Please provide complete reference details
Tinnitus, a Military Epidemic: Is Hyperbaric Oxygen Therapy the Answer? ABSTRACT Tinnitus is the phantom perception of sound in the absence of overt acoustic stimulation. Its impact on themilitary population is alarming. Annually, tinnitus is the most prevalent disability among new cases added to theVeterans Affairs numbers. Also, it is currently the most common disability from the War o
 with less danger of penetration or neurovascular bundledamages. The distal aperture should be positionedbehind the tip ; this has the advantage that skin can belifted by the tip of the cannula without direct subcuta-neous fat removal. Multiple holes increase the efficien-cy of fat removal, resulting in fewer passes of the can-nula and less tissue trauma.
As regards the diameter of the cannula, no single
diameter suits all anatomic areas. Originally, traditionalliposuction was performed using very large cannulas(10 mm) which had to be kept in the deep fat to avoidsurface irregularities. With the advent of smaller cannu-las (2-3 mm) and different tip configurations, surgeonscan work closer to the skin without creating noticeable
irregularities and perform liposuction of areas of sparsefat deposits. After superficial liposuction treatment of
2,500 patients, Gasperoni describes good aesthetic
A. This is an excellent case for limited liposuction of fat
results on patients with “old and less elastic skin”. A
deposits located at the top of the thighs and on the hips, with
skin retraction, following the superficial removal of fat
excellent skin quality ; B. At 6 months post-operativesmoother curves can be observed with excellent skin retraction
deposits would be responsible for these results (8).
with less danger of penetration or neurovascular bundledamages. The distal aperture should be positionedbehind the tip ; this has the advantage that skin can belifted by the tip of the cannula without direct subcuta-neous fat removal. Multiple holes increase the efficien-cy of fat removal, resulting in fewer passes of the can-nula and less tissue trauma.
As regards the diameter of the cannula, no single
diameter suits all anatomic areas. Originally, traditionalliposuction was performed using very large cannulas(10 mm) which had to be kept in the deep fat to avoidsurface irregularities. With the advent of smaller cannu-las (2-3 mm) and different tip configurations, surgeonscan work closer to the skin without creating noticeable
irregularities and perform liposuction of areas of sparsefat deposits. After superficial liposuction treatment of
2,500 patients, Gasperoni describes good aesthetic
A. This is an excellent case for limited liposuction of fat
results on patients with “old and less elastic skin”. A
deposits located at the top of the thighs and on the hips, with
skin retraction, following the superficial removal of fat
excellent skin quality ; B. At 6 months post-operativesmoother curves can be observed with excellent skin retraction
deposits would be responsible for these results (8).
 The cannula most often used with the Lipomatic® is size 4,with a foam end and multiple holes. The nutation movementsof the head and the multiple holes make for optimum fatremoval during a cannula pass.
The cannula most often used with the Lipomatic® is size 4,with a foam end and multiple holes. The nutation movementsof the head and the multiple holes make for optimum fatremoval during a cannula pass.