Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Amgast#72124
Systematic Review on the Management of IrritableBowel Syndrome in North AmericaLawrence J. Brandt, M.D., Chairman,1 David Bjorkman, M.D.,2 M. Brian Fennerty, M.D.,3G. Richard Locke, M.D.,4 Kevin Olden, M.D.,5 Walter Peterson, M.D.,6 Eamonn Quigley, M.D.,7Philip Schoenfeld, M.D., M.S.Ed., M.Sc. (Epi),8 Marvin Schuster, M.D.,9 and Nicholas Talley, M.D., Ph.D.101Albert Einstein College of Medicine, Bronx, NY; 2University of Utah School of Medicine, Salt Lake City,UT; 3Oregon Health Sciences University, Portland, OR; 4Mayo Clinic, Rochester, MN; 5Mayo Clinic,Scottsdale, AZ; 6University of Texas Southwestern Medical School, Dallas, TX; 7National University ofIreland, Cork, Ireland; 8University of Michigan School of Medicine, Ann Arbor, MI; 9Johns Hopkins BayviewMedical Center, Baltimore, MD; and 10Nepean Hospital, Penrith, New South Wales, Australia2.1 METHODS
ments have been described, and IBS experts on the TaskForce contributed their advice about the effect of individual
patient preferences on these recommendations.
a. a transparent link between the evidence and the recom-
Literature Search
In order to identify relevant IBS therapy trials for inclusion
b. explicit criteria for inclusion of studies to serve as the
in this guideline, the following literature search techniques
were employed. Separate PUBMED, MEDLINE, and EM-
c. comprehensive searching of the literature for relevant
BASE searches of English language articles from 1980 to
2001 were performed with different combinations of the
d. a standardized and explicit system for grading the meth-
following search terms: “antispasmodics,” “antimusca-
rinics,” “dicyclomine,” “hyoscyamine,” “constipation,” “fi-
e. a standardized and explicit system for grading recom-
ber,” “polycarbophil,” “bulking agents,” “laxatives,” “anti-
f. recommendations should acknowledge the magnitude of
“alosetron,” “antidiarrheal agents,” “loperamide,” “behav-
treatment benefit, the adverse events associated with the
ioral therapy,” “irritable bowel syndrome,” “clinical trial,”
treatment, and individual patient preferences that may
and “randomized (pt).” The bibliographies of IBS therapy
guide the application of guideline recommendations (1–3).
trials, selected review articles, and selected meta-analyseswere manually searched. Multiple pharmaceutical compa-nies, including AstraZeneca, Pfizer, Salix, Novartis, Solvay,
In order to fulfill these requirements, Task Force members
Merck, and GlaxoSmithKline, were contacted to identify
used several techniques. Each section of the systematic
relevant unpublished trials of IBS therapies and to obtain
review has been numbered to provide a link between the
additional data from published trials of IBS therapies.
evidence and the recommendations. Standard techniques for
In order to identify relevant trials about the epidemiology
literature searching and study selection were used for each
of IBS and the diagnostic approach to patients with IBS
section of this document (4, 5). Data on study methodology
symptoms, the following literature search techniques were
and study results were extracted onto standard forms and
employed. Separate MEDLINE and EMBASE searches of
summaries of data are presented in tables and graphs, en-
English language articles were performed with different
suring that the methodologic rigor of individual studies is
combinations of the following search terms. For epidemi-
defined and that the magnitude of treatment benefit is quan-
ology of IBS, “colonic diseases, functional” was exploded
tified. A commonly used system for grading recommenda-
with key words “incidence,” “prevalence,” “prognosis,” and
tions in evidence-based guidelines (6) was adapted for this
“natural history.” Similar combinations were exploded us-
document (see Section 2.2), ensuring that an explicit and
ing “irritable colon.” For diagnostic approach to the patient
transparent process was used to make recommendations
with IBS symptoms, search terms were “colonic diseases,
based on the strength of the evidence. Adverse events and
functional (diagnosis)” or “irritable, functional, or spastic
individual patient preferences may affect the application of
colon.” These terms were then exploded with the descriptive
guideline recommendations. Therefore, adverse events have
key words “blood,” “parasite,” “stool analysis,” “radiogra-
been assessed, relative contraindications to specific treat-
phy,” “hydrogen breath testing,” “endoscopy,” “barium en-
ACG Functional GI Disorders Task Force
ema,” “colonoscopy or flexible sigmoidoscopy.” Bibliogra-
Table 2.1.1. Quantitative Assessment of Study Methodology
phies from all potentially relevant articles were manually
1. ROME criteria to identify patients with IBS.
A medical education and research company (EBMed,
2. Randomization. 3. Parallel study design (i.e., no crossover studies).
LLC, Anaheim Hills, CA) assisted the Task Force with
literature searches, application of study selection criteria,
data extraction and analysis, and assessment of method-
ologic quality of individual trials.
7. Baseline observation of patients to assess symptoms. 8. Treatment duration of 8–12 weeks or longer. 9. Follow-up after treatment to assess symptoms. Study Selection Criteria
10. Compliance with the treatment is measured.
The titles and abstracts of all citations identified by the
11. Sample size calculation is provided and adequate sample
literature searches were reviewed. Potentially relevant stud-
ies were retrieved, and the selection criteria were applied.
12. Primary outcome of the trial is improvement in global IBS
Since a North American perspective was used, only treat-
13. Primary outcome is based on patient assessment.
ments available in the United States were examined and
14. Validated scale used to measure improvement in IBS
only epidemiologic studies from North American popula-
tions were reviewed. For IBS therapy trials, the selection
Data from Veldhuyzen van Zanten SJO, Talley NJ, Bytzer P, et al. Design of treatment
criteria were 1) randomized controlled trial (RCT); 2) pop-
trials for functional gastrointestinal disorders. Gut 1999;45(suppl II):II69 –77.
* The members of the Committee on Design of Treatment Trials for Functional
ulation of adult patients with IBS; 3) comparison of IBS
Gastrointestinal Disorders of the Rome II committee also noted additional recom-
therapy vs placebo or control therapy; 4) evaluation of relief
mendations for the design of clinical trials, including a priori defined study endpointand definition of patient setting (primary care vs tertiary care). However, published
of IBS symptoms; 5) results published in English in full
reports rarely provided adequate information to assess the use of these additional
manuscript form (or adequate data available after written
techniques in the conduct of treatment trials. Therefore, these additional techniqueswere not included in the scale.
communication with investigators); and 6) therapy availablein the United States. For epidemiology of IBS studies, theselection criteria were 1) studies of population-based sam-
study endpoints, and dosages of study medication, no at-
ples of IBS patients in North America; 2) use of Manning,
tempt was made to combine results into meta-analyses.
ROME I, or ROME II criteria to identify IBS patients; 3)
In this data analysis, improvement in global IBS symp-
population of adult patients; 4) results reported on preva-
toms was considered the primary outcome of interest. The
lence, incidence, or natural history of IBS; and 5) results
Task Force agrees with the recommendations of the ROME
published in English and in full manuscript form. For trials
Committee (7): “The primary outcome measure should
about the diagnostic approach to the patient with IBS symp-
. . .integrate the key symptoms of [IBS]. . .allowing the pa-
toms, the selection criteria were 1) use of a cohort of IBS
tient to integrate the contribution of a disparate group of
patients explicitly diagnosed via symptom-based criteria
symptoms (abdominal pain, bloating, and altered bowel
(e.g., Manning or ROME criteria); 2) performance of a
function) into a single global clinical rating.” This assess-
commonly applied diagnostic test with a blinded compari-
ment should be done by the patient, as it is doubtful that a
son to an appropriate gold standard diagnostic test for or-
physician’s assessment of a patient’s improvement in global
ganic GI disease; and 3) quantification of the results as
IBS symptoms would be more accurate or more reliable than
either normal or abnormal, in which case an additional or
alternative diagnosis of organic disease was made based on
For epidemiology of IBS studies, data on study method-
ology and study results were also abstracted onto standardforms. Data were abstracted about 1) symptom-based defi-
Data Extraction and Analysis
nition of IBS (e.g., Manning Criteria or ROME Criteria); 2)
For IBS therapy trials, data on study methodology and study
sample size and case ascertainment technique to identify
results were abstracted onto standard forms for the perfor-
IBS patients; 3) prevalence, incidence, prevalence of IBS
mance of systematic reviews. Data were extracted about 1)
subgroups, gender distribution, and mean age of onset of
study population, including proportion of female patients; 2)
symptoms; and 4) disease activity (e.g., prevalence of IBS
intervention: dosage and schedule of administration of treat-
over time and frequency of IBS flares within a specified
ment vs placebo or control therapy; 3) study duration; and 4)
period of time). For trials about the diagnostic approach to
proportion of patients achieving improvement in global IBS
the patient with IBS symptoms, data were abstracted about
symptoms, abdominal pain, bloating, changes in bowel hab-
1) symptom-based criteria used to identify IBS patients; 2)
its, and adverse events. The ROME committee recom-
diagnostic evaluation performed and gold standard compar-
mended study design techniques to minimize bias in trials of
ison; 3) prevalence of confirmed organic GI disease, result-
functional GI disorders (7) (Table 2.1.1). Data on the use of
ing in an alternative diagnosis to explain IBS symptoms; and
these techniques were extracted and summarized in tabular
4) the accuracy of diagnostic tests in a population of IBS
form; however, because of wide variation in study design,
Management of IBS 2.2 LEVELS OF EVIDENCE AND GRADING OF
produce a Type I error. Intermediate-quality RCTs may also
RECOMMENDATIONS
be susceptible to Type II errors due to inadequate samplesize. Level III–V evidence comes from nonrandomized tri-
Quantitative Assessment of Study Methodology
als or case studies. These are observational studies and are
Previous reviews and epidemiologic studies (8 –10) have
prone to multiple biases that produce Type I errors. For this
established methodologic criteria that minimize bias and
review, Level III–V evidence was not used to make recom-
enhance validity of trials about therapy, including the use of
mendations about IBS therapies. Level III–V evidence was
randomization, concealed allocation, double blinding, and
only used to make recommendations about the diagnostic
complete patient follow-up. Additionally, the ROME com-
approach to the patient with IBS symptoms or about epide-
mittees described the preferred design of treatment trials for
miology of IBS because data on these topics may only be
functional gastrointestinal disorders (7) (Table 2.1.1). In
available from observational studies.
order to assess the methodologic strength of individualstudies about IBS therapies, a quantitative scale of study
Grading of Recommendations
quality was developed. This scale uses the ROME commit-
Recommendations are listed as Grade A, Grade B, or Grade
tee recommendations for design of treatment trials for func-
C (see Table 1.0.2 in Evidence-Based Position Statement on
tional gastrointestinal disorders (Table 2.1.1). Each meth-
Management of IBS). Grade A recommendations are sup-
odologic criterion on the scale was assigned one point.
ported by the strongest (Level I) evidence. Task Force
Therefore, a study could receive a maximum score of 14
members strongly believe that these recommendations are
points for quality of study methodology. This scale esti-
accurate, based on the evidence. Grade B recommendations
mates the methodologic rigor of an individual trial: a trial
are supported by intermediate-quality (Level II) evidence.
with a low quality score may be more likely to produce
Task Force members believe that Grade B recommendations
inaccurate or biased results and a trial with a high quality
may have important limitations due to the intermediate
score may be more likely to produce accurate and unbiased
quality of the evidence. These recommendations may
change in the future if high-quality (Level I) evidence be-
No standard criteria are available to rate the methodologic
comes available. Grade C recommendations are supported
strength of epidemiologic studies in a systematic review.
by Level III–V evidence. Because these recommendations
Population-based studies may be preferable to studies of
are based largely on observational studies, the strength of
referral populations as referral populations may provide
evidence behind these recommendations is limited. Grade C
inflated estimates of the prevalence and incidence of a
recommendations are only provided because they represent
disorder. Therefore, epidemiologic studies in this review are
the best evidence about the epidemiology of IBS and the
limited to population-based studies. In order to assess the
diagnostic approach to patients with IBS symptoms.
methodologic strength of studies about the diagnostic tests,a standard scale was used to evaluate the methodologicquality of studies (11). The quality of each diagnostic test
REFERENCES: SECTION 2.1 AND 2.2
study was determined by assessing the methodology for 1)
1. Hayward R, Wilson M, Tunis S, et al. User’s guides to the
study population; 2) verification bias; 3) blinded interpreta-
medical literature. VIII. How to use clinical practice guideline
tion of test results; 4) biased patient selection; 5) data
recommendations. A. Are the recommendations valid? JAMA
collection; 6) details of diagnostic tests; 7) details of refer-
2. Wilson M, Hayward R, Tunis S, et al. User’s guide to the
ence tests; and 8) details of the study population. The total
medical literature. VIII. How to use clinical practice guide-
lines. B. What are the recommendations and will they help youin caring for your patients? JAMA 1995:274;1630 –2. Levels of Evidence
3. Guyatt G, Sackett D, Sinclair J, et al. User’s guide to the
Levels of evidence have been previously defined (see Table
medical literature. IX. A method for grading health care rec-ommendations. JAMA 1995;274:1800 – 4.
1.0.2 in Evidence-Based Position Statement on Manage-
4. Egger M, Smith GD. Principles of and procedures for system-
ment of IBS). Level I evidence represents high-quality
atic reviews. In: Egger M, Smith GD, Attman DG, eds. Sys-
RCTs. These RCTs have few limitations in their study
tematic reviews in health care, 2nd ed. London: BMJ, 2001:
design, which should minimize Type I errors. Thus, if the
trial does show a significant difference between treatment
5. Oxman A, Guyatt G, Cook D, et al. Summarizing the evi-
dence. In: Guyatt G, Rennie D, eds. User’s guide to the
and placebo, then it will be unlikely that this finding is due
medical literature: A manual for evidence-based clinical prac-
to biased study design. High-quality RCTs also have ade-
tice. Chicago: AMA Press, 2001:155–75.
quate power to minimize Type II errors. Thus, if the trial
6. Cook D, Guyatt G, Laupacis A, et al. Rules of evidence and
does not show a significant difference between treatment
clinical recommendations on the use of anti-thrombotic
and placebo, then it will be unlikely that this finding is due
agents. Chest 1992;102(suppl 4):3055–115.
7. Veldhuyzen van Zanten SJO, Talley NJ, Bytzer P, et al.
to an inadequate sample size of patients. Level II evidence
Design of treatment trials for functional gastrointestinal dis-
represents intermediate-quality RCTs. These RCTs have
orders. Gut 1999;45(suppl II):II69 –77.
important limitations in their study design, which could
8. Schoenfeld P, Cook D, Hamilton F, et al. An evidence-based
ACG Functional GI Disorders Task Force Table 2.3.1. Symptom-Based Criteria for the Diagnosis of IBS
At least 12 weeks of continuous or recurrent
At least 12 weeks, which need not be consecutive, in
the preceding 12 months of abdominal discomfortor pain that has two of the following threefeatures:
Onset associated with a change in frequency of stool
(2) associated with a change in frequency
Onset associated with a change in form (appearance)
Two or more of the following, at least on
(4) Passage of mucus, or(5) Bloating or feeling of abdominal
1. Manning AP, Thompson WG, Heaton KW, et al. Towards a positive diagnosis of the irritable bowel syndrome. BMJ 1978;2:653– 4. 2. Thompson WG, Dotewall G, Drossman DA, et al. Irritable bowel syndrome: Guidelines for the diagnosis. Gastroenterol Int 1989;2:92–5. 3. Thompson WG, Longstreth GF, Drossman DA, et al. Functional bowel disorders and functional abdominal pain. Gut 1999;45(suppl II):II43–7.
approach to gastroenterology therapy. Gastroenterology 1998;
diagnosis of IBS in research studies (4 – 8). These criteria,
which include the Manning criteria and ROME I and ROME
9. Schulz KF, Chalmers I, Hayes RJ, et al. Empirical evidence of
II Committee criteria (Table 2.3.1), are widely used to
bias: Dimensions of methodological quality associated withestimates of treatment effects in controlled trials. JAMA 1995;
identify IBS patients for epidemiologic studies and to ensure
that appropriate IBS patients are enrolled in trials of IBS
10. Chalmers TC, Celano P, Sacks HS, et al. Bias in treatment
therapies; however, the usefulness of these detailed criteria
assignment in controlled clinical trials. N Engl J Med 1983;
in the clinical setting is uncertain. Few primary care physi-
cians use these criteria in practice or even know that these
11. Lijmer JG, Mol BW, Heisterkamp S, et al. Empirical evidence
of design-related bias in studies of diagnostic tests. JAMA
criteria exist (9). Overall, these criteria emphasize that IBS
is characterized by abdominal discomfort associated withaltered bowel habits. Given the varied symptoms of IBS andthe uncertain clinical utility of Manning and ROME criteria,
2.3 SYMPTOM-BASED CRITERIA FOR IRRITABLE BOWEL
Task Force members suggest that physicians should use a
SYNDROME AND THRESHOLD TO TREAT IRRITABLE
broad definition of IBS: “abdominal discomfort associatedBOWEL SYNDROME
The ROME I committee of IBS experts has characterized
IBS is defined as abdominal discomfort associated with
subgroups of functional gastrointestinal disorders, including
altered bowel habits (Grade C recommendation). IBS sig-
diarrhea-predominant IBS and constipation-predominant
nificantly diminishes the quality of life among most IBSpatients who actively seek medical care (Grade C recom-
IBS (10). These subgroup classifications have been used to
mendation). Treatment of IBS patients is indicated when the
enroll patients in trials of IBS therapies; however, the
patient and physician believe that the IBS symptoms dimin-
ROME II committee of IBS experts noted that subgroup
ish the quality of life of the patient (Grade C recommenda-
classifications are unstable over time (11). IBS with consti-
tion). IBS therapies should improve global IBS symptoms,
pation may change to constipation alone or IBS alternating
including abdominal discomfort, bloating, and altered
between constipation and diarrhea. Given this symptom
bowel habits (Grade C recommendation).
instability, the ROME II committee discouraged the use of
IBS lacks a biological marker. No structural, biochemical,
IBS subtypes to categorize patients, and the Task Force
or physiological abnormalities are consistently demon-
members agree and endorse this recommendation. Task
strated in IBS patients. Thus, the definition of IBS is symp-
Force members recommend that IBS patients should be
tom-based and obtaining an accurate history of the patient’s
identified using symptom-based criteria: IBS alternating be-
symptoms is crucial. Symptoms of IBS may include, but are
tween diarrhea and constipation; IBS associated with ab-
not limited to, abdominal discomfort/pain, bloating, diar-
dominal discomfort, bloating, and constipation; or IBS as-
rhea, fecal urgency, and constipation (1–3).
sociated with abdominal discomfort, fecal urgency, and
Multiple symptom scores and symptom-based criteria for
IBS have been developed by IBS experts to facilitate the
IBS symptoms significantly diminish the quality of life of
Management of IBS
IBS patients who actively seek medical care for their symp-
7. Thompson WG, Longstreth FG, Drossman DA, et al. Func-
toms (12–16). Trials using validated scales of quality of life
tional bowel disorders and functional abdominal pain. Gut1999;45(suppl II):II43–7.
demonstrate that IBS patients have worse quality of life than
8. Kruis W, Thieme CH, Weinzierl M, et al. A diagnostic score
healthy controls and patients with gastroesophageal reflux
for the irritable bowel syndrome: Its value in the exclusion of
disease (GERD). Their quality of life was similar to patients
organic disease. Gastroenterology 1984;87:1–7.
with diabetes mellitus but better than patients with end-stage
9. Thompson WG, Heaton KW, Smyth GT, et al. Irritable bowel
renal disease (12, 16). The ability to generalize the findings
syndrome: The view from general practice. Eur J Gastroen-terol Hepatol 1997;9:689 –92.
of these studies to all patients with IBS is limited because
10. Drossman DA, Thompson WG, Talley NJ, et al. Identification
many of these studies evaluated patients with moderate-
of subgroups of functional gastrointestinal disorders. Gastro-
severe IBS being seen in subspecialty clinics. Observational
studies of IBS patients also indicate that IBS symptoms lead
11. Veldhuyzen van Zanten SJO, Talley NJ, Bytzer P, et al.
to increased absenteeism and lost productivity at work (17,
Design of treatment trials for functional gastrointestinal dis-orders. Gut 1999;45(suppl II):II69 –77.
12. El-Serag HB, Olden K, Bjorkman D. Health-related quality of
Although IBS diminishes quality of life, no data are
life among persons with irritable bowel syndrome: A system-
available to guide recommendations about the threshold to
atic review. Aliment Pharmacol Ther 2002;16:1171– 85.
treat IBS. Therefore, Task Force members developed an
13. Whitehead WE, Burnett CK, Cook EW, et al. Impact of
expert-based recommendation about this topic. Some IBS
irritable bowel syndrome on quality of life. Dig Dis Sci 1996;41:2248 –53.
patients may seek medical care simply for reassurance.
14. O’Keefe EA, Talley NJ, Zinsmeister AR, et al. Bowel disor-
When such patients are reassured that their symptoms do not
ders impair functional status and quality of life in the elderly:
represent cancer or another life-threatening disorder, no
A population-based study. J Gerontol A Biol Sci Med 1995;
further treatment may be needed; however, treatment should
be offered if the patient and physician believe that the IBS
15. McGee HM, O’Boyle CA, Hickey A, et al. Assessing the
quality of life of the individual: The SEIQoL with a healthy
symptoms diminish the quality of life of the patient.
and a gastroenterology unit population. Psychol Med 1991;
The ROME committee of IBS experts opined that im-
provement in global IBS symptom improvement should be
16. Gralnek I, Hays RD, Kilbourne A, et al. The impact of irritable
the primary outcome in trials of IBS therapies (11): “The
bowel syndrome on health-related quality of life. Gastroenter-
symptoms that result in a diagnosis [of IBS] are varied and
17. Hahn BA, Yan S, Strassels S. Impact of irritable bowel syn-
interact in complex ways. Thus, there is a strong argument
drome on quality of life and resource use in the United States
for a primary outcome measure that allows the patient to
and United Kingdom. Digestion 1999;60:77– 81.
integrate the contribution of a disparate group of symptoms
18. Drossman DA, Li Z, Andruzzi E, et al. US Householder
into a single global rating.” The Task Force members agree
survey of functional gastrointestinal disorders: Prevalence,
sociodemography, and health impact. Dig Dis Sci 1993;38:1569 – 80. In clinical practice, IBS may be defined as abdominaldiscomfort associated with altered bowel habits. IBS signif-icantly diminishes the quality of life among most IBS pa-2.4 EPIDEMIOLOGY OF IRRITABLE BOWEL SYNDROME tients seeking medical care, and treatment should be offeredIN NORTH AMERICA to these patients. IBS therapies should improve global IBSsymptoms, including abdominal discomfort, bloating, andThe prevalence of IBS in North America is approximately10 –15%, equally divided among IBS with constipation, IBSwith diarrhea, and IBS alternating between diarrhea andconstipation. There is a 2:1 female predominance of IBS inREFERENCES: SECTION 2.3 North America in population-based studies (Grade C rec-ommendation).
1. Maxton DG, Whorwell PJ. Abdominal distention in the irri-
Knowledge about the epidemiology of IBS serves several
table bowel syndrome: The patient’s perspective. Eur J Gas-troenterol Hepatol 1992;101:927–34.
purposes. Understanding the natural history of IBS facili-
2. Maxton DG, Morris JA, Whorwell PJ. Ranking of symptoms
tates patient education. Data on the use of diagnostic tests,
in the irritable bowel syndrome. BMJ 1989;299:1138.
surgeries, and medications in IBS patients may educate
3. Lembo T, Naliboff B, Munakata J, et al. Symptoms and
physicians about the management of IBS. Finally, simply
visceral perception in patients with pain-predominant IBS.
confirming that IBS is very common may justify renewed
Am J Gastreonterol 1999;94:1320 – 6.
4. Manning AP, Thompson WG, Heaton KW, et al. Towards
research about this disorder. In this portion of the mono-
positive diagnosis of the irritable bowel. BMJ 1978;2:653– 4.
graph, the objectives were to systematically review the IBS
5. Kruis W, Thieme CH, Weinzierl M, et al. A diagnostic score
epidemiology literature about 1) the prevalence of IBS and
for the irritable bowel syndrome: Its value in the exclusion of
the prevalence of IBS subtypes in North America; 2) the age
organic disease. Gastroenterology 1984;87:1–7.
of onset and gender distribution of IBS in North America;
6. Thompson WG, Creed FH, Drossman DA, et al. Functional
bowel disorders and functional abdominal pain. Gastroenterol
and 3) the natural history of IBS in North America.
Nine population-based North American studies (1–9)
ACG Functional GI Disorders Task Force Table 2.4.1. Population-Based IBS Prevalence Studies in North America
* Manning 2 reflects that patient only needed to meet two Manning criteria to be diagnosed with IBS. Data from Saito YA, Schoenfeld P, Locke GR. The epidemiology of irritable bowel syndrome in North America: A systematic review. Am J Gastroenterol 2002;97:1910 –5.
quantified the prevalence of IBS, the gender distribution of
IBS at the beginning of the study did not meet diagnostic
IBS, and prevalence of IBS subtypes. Literature search
criteria for IBS after 1 year. Data from referral populations
techniques, study selection criteria, and data analysis are
suggest that other causes of IBS symptoms are rarely iden-
outlined in Section 2.1. In these studies, the diagnosis of IBS
tified during long-term follow-up (11, 12) and that patients
was made using symptom-based criteria (either Manning
with active IBS symptoms experience frequent flares, char-
criteria, ROME criteria, or a modification of ROME crite-
acterized by several days with more severe symptoms fol-
ria). The literature search did not reveal any North American
lowed by several days with minimal symptoms (12, 13).
population-based studies about the natural history of IBS.
Data from Europe (12, 14 –16) demonstrate that IBS patients
Also, no studies specified the age of onset of IBS symptoms.
are two times more likely to undergo abdominal surgery
The prevalence of IBS varied between 3% and 20%
than healthy controls. Future studies should report on the
across different studies (1– 4, 9), although most estimates
disease activity (e.g., frequency, duration, and intensity of
were concentrated between 10% and 15% (Table 2.4.1). The
symptoms) of IBS and current management of IBS, includ-
differences in the reported prevalence of IBS probably re-
ing use of diagnostic tests, surgery, and medication. As
flect different definitions of IBS (e.g., Manning criteria vs
noted in previous systematic reviews (12), ideal natural
ROME criteria) and differences in study design rather than
history studies would 1) use a population-based sample of
true differences in the prevalence of IBS. Three studies (1,
IBS patients followed from the time of diagnosis; 2) use an
2, 9) estimated a 2:1 female predominance of IBS, and two
appropriate and objective standard for the diagnosis of IBS
population-based studies limited to Olmsted County, MN
(e.g., ROME II criteria); 3) use repeated surveys of the
(3, 4) estimated a 1:1 distribution. These results are in
cohort over time; and, 4) provide sufficiently long and
contrast to studies of referral populations, which have usu-
complete follow-up of the cohort of IBS patients.
ally demonstrated a 3:1 or 4:1 female predominance of IBS
Overall, the quality and quantity of studies about IBS
(10). Patients younger than 45 years of age were more likely
epidemiology are limited. IBS is a common disorder in
to be diagnosed with IBS than were those older than 45
North America, and equivalent numbers of IBS patients
years (13.5% vs 9.4%) (2), although one study from Olm-
suffer from constipation, diarrhea, and alternating between
sted County found that the prevalence of IBS rose from 8%
constipation and diarrhea. It is prevalent in young and
in the 65–74-year-old age group to 12% in the group older
elderly patients and in men and women, although younger
than 85 years (5). Two population-based studies (6, 9)
patients and women are more likely to be diagnosed with
assessed the prevalence of IBS subgroups: constipation-
IBS in North America. Data from population-based studies
predominant IBS ϭ 5.2–5.4%; diarrhea-predominant IBS ϭ
about the natural history of IBS in North America is non-
5.0 –5.5%; IBS alternating between diarrhea and constipa-
existent. Limited data from Europe confirm that IBS patients
tion ϭ 5.2%. A study about constipation, the Epidemiology
are unlikely to be diagnosed with other significant medical
of Constipation study (EPOC) (7), estimated the prevalence
disorders over long-term follow-up.
of constipation-predominant IBS at 2.1% and the prevalenceof IBS with rectal outlet symptoms at 3.5%.
No population-based study in North America has esti-
REFERENCES: SECTION 2.4
mated the incidence of IBS or described the natural historyof IBS. One study of Olmsted County, MN residents (8)
1. Hahn BA, Saunders WB, Maier WC. Differences between
found that 38% of patients who met Manning criteria for
individuals with self-reported irritable bowel syndrome
Management of IBS
(IBS) and IBS-like symptoms. Dig Dis Sci 1997;42:2585–
with alarm symptoms or signs. Alarm symptoms or signsmay include, but are not limited to, hematochezia, weight
2. Drossman DA, Zhiming L, Andruzzi E, et al. US householder
loss greater than 10 pounds, family history of colon cancer,
survey of functional gastrointestinal disorders. Dig Dis Sci1993;38:1569 – 80. recurring fever, anemia, and chronic severe diarrhea
3. Talley NJ, Zinsmeister AR, Van Dyke C, et al. Epidemiology
(Grade C recommendation). Routine use of colon cancer
of colonic symptoms and the irritable bowel syndrome. Gas-
screening tools is recommended for all patients Ն50 years
4. Saito YA, Locke GR, Talley NJ, et al. A comparison of the
Rome and Manning criteria for case identification in epidemi-
Multiple diagnostic tests have been recommended as
ological investigations of irritable bowel syndrome. Am J
screening tests for patients with IBS symptoms (1–5). These
diagnostic tests, which include complete blood cell count
5. Talley NJ, O’Keefe EA, Zinsmeister AR. Prevalence of gas-
(CBC), erythrocyte sedimentation rate (ESR), serum chem-
trointestinal symptoms in the elderly: A population-based
istries, thyroid function tests, stool culture and examination
study. Gastroenterology 1992;102:895–901.
6. Talley NJ, Zinsmeister AR, Melton LJ. Irritable bowel syn-
for ova and parasites (stool O & P), fecal occult blood test
drome in a community: Symptom subgroups, risk factors, and
(FOBT), colonic visualization with flexible sigmoidoscopy
healthcare utilization. Am J Epidemiol 1995;142:76 – 83.
(FS), barium enema (BE), or colonoscopy, and hydrogen
7. Stewart WF, Liberman JN, Sandler RS, et al. Epidemiology of
breath tests (1–5), are intended to rule out organic diseases,
constipation (EPOC) study in the United States: Relation of
including hyper/hypothyroidism, inflammatory bowel dis-
clinical subtypes to sociodemographic features. Am J Gastro-enterol 1999;94:3530 – 40.
ease, colorectal cancer, infectious diarrhea, and lactose mal-
8. Talley NJ, Weaver AL, Zinmeister AR, et al. Onset and
absorption. When deciding if a diagnostic test is needed to
disappearance of gastrointestinal symptoms and functional
rule out an organic disease, clinicians should consider the
gastrointestinal disorders. Am J Epidemiol 1992;136:165–
pretest probability or prevalence of the organic disease in
9. Thompson WG, Irvine EJ, Pare P, et al. Functional gastroin-
patients with specific symptoms (6). If the pretest probabil-
testinal disorders in Canada: First population based survey
ity or prevalence is sufficiently high to justify performance
using ROME II criteria with suggestions for improving the
of a diagnostic test, then the clinician should also consider
questionnaire. Dig Dis Sci 2002;47:225–35.
the accuracy (e.g., sensitivity, specificity) of the diagnostic
10. Owens DM, Nelson DK, Talley NJ. The irritable bowel
test before ordering it. (Note: the following analysis does
syndrome: Long-term prognosis and the patient-physician in-teraction. Ann Intern Med 1995;122:107–12.
not apply to IBS patients with alarm symptoms or signs. The
11. Harvey RF, Mavad EC, Brown AM. Prognosis in the irritable
presence of alarm symptoms or signs suggests a higher
bowel syndrome: A 5-year prospective study. Lancet 1987;I:
pretest probability or prevalence of organic disease and may
justify the performance of diagnostic tests. Alarm symptoms
12. Saito YA, Schoenfeld P, Locke GR. The epidemiology of
irritable bowel syndrome in North America: A systematic
or signs include, but are not limited to, hematochezia, ane-
review. Am J Gastroenterol 2002;97:1910 –5.
mia, persistent fevers, weight loss Ͼ10 pounds, chronic
13. Hahn B, Watson M, Yan S, et al. Irritable bowel syndrome
severe diarrhea, and family history of colon cancer.)
symptom patterns: Frequency, duration, and severity. Dig Dis
Six studies (7–12) addressed the pretest probability or
prevalence of organic disease in patients with IBS symp-
14. Kennedy TM, James RH. Epidemiology of cholecystectomy
and irritable bowel syndrome in a UK population. Br J Surg
toms (Table 2.5.1). Literature search techniques, study se-
lection criteria, and data analysis are outlined in Section 2.1.
15. Harvey RF, Mavad EC, Brown AM. Prognosis in the irritable
In these six studies (7–12), the diagnosis of IBS was made
bowel syndrome: A 5-year prospective study. Lancet 1987;1:
using symptom-based criteria (either Manning criteria,
16. Kay L, Jorgensen T, Jensen KH. The epidemiology of irritable
ROME criteria, or a modification of ROME criteria). Qual-
bowel syndrome in a random population: Prevalence, inci-
ity scores for these studies ranged from 5 to 6 on a 0 – 8 point
dence, and natural history and risk factors. J Intern Med
scale, suggesting intermediate-high quality design of a di-
agnostic test study. The symptom-based diagnosis of IBSwas made prior to the performance of diagnostic tests in allstudies. Several caveats about these studies should be con-
2.5 DIAGNOSTIC APPROACH TO THE PATIENT WITH IBS
sidered. First, most studies (8 –10, 12) examined relatively
SYMPTOMS
small populations (100 –200) of IBS patients. Therefore, the
Among IBS patients without alarm symptoms, the routine
ability to generalize these results is limited. Second, several
use of flexible sigmoidoscopy, barium enema, colonoscopy,
studies (7–9) examined referral populations of IBS patients
fecal occult blood tests, stool for ova and parasites, stool for
who had already undergone colonoscopy. It is possible that
culture, or thyroid function tests cannot be recommended
patients with organic diseases were diagnosed at the primary
(Grade C recommendation). Among IBS patients with diar-
care level and that patients seen in referral settings do not
rhea, testing for celiac sprue may be considered (Grade C
provide an accurate estimate of the prevalence of organic
recommendation). Endoscopic studies, stool studies, and
diseases among patients with IBS symptoms. Finally, no
other radiologic tests may be indicated among IBS patients
studies properly used a gold standard test to estimate the
ACG Functional GI Disorders Task Force 2.5.1. Trial Table 2.5.2. Prevalence of Organic Disease in Patients Meeting
Data from Cash BD, Schoenfeld P, Chey WD. The utility of diagnostic tests in IBS
patients: A systematic review. Am J Gastroenterol (in press).
growth syndrome) and did not use an appropriate control
group to determine if antibiotics effectively decreased the
Despite the absence of data to recommend diagnostic
testing in IBS patients, the value of diagnostic testing ispartly derived from the reassurance value of normal diag-
accuracy of diagnostic tests for organic GI diseases among
nostic tests. In other words, both physicians and patients
may be reassured after a negative evaluation for organic
FS, colonoscopy, and BE identified an organic GI disease
disease. The value of this “reassurance” is unclear and
responsible for symptoms in 0 –1.3% of patients with IBS
symptoms (7–10). Neither abdominal ultrasound (10) nor
Overall, available data do not support the performance of
rectal biopsy (9) identified organic disease that was respon-
diagnostic tests among patients with IBS. IBS patients do
sible for symptoms. The use of CBC, serum chemistries, and
not appear to have an increased likelihood of most organic
FOBT identified an organic disease responsible for symp-
diseases compared with control populations without IBS
toms in 0 –1.3% of patients (8, 11). Positive tests for stool O
symptoms. Patients with alarm symptoms (e.g., hematoche-
& P were found in 0 –1.6% of patients with IBS symptoms,
zia, weight loss, etc.) may have a higher prevalence of
although it is unclear if treatment for these infections re-
organic disease and routine diagnostic testing in these pa-
solved the symptoms of IBS (7, 8). Abnormal TSH was
tients may be appropriate. Also, celiac sprue may be more
identified in 0.6 – 6% of patients with IBS symptoms, and
prevalent among patients with IBS symptoms, and routine
abnormal breath tests for lactose intolerance were found in
evaluation of celiac sprue may be considered. The quality
22–26% of patients with IBS symptoms (7, 8). It is unclear,
and quantity of studies about the diagnostic approach to
however, if these disorders accounted for IBS symptoms,
patients with IBS symptoms is limited, and definitive rec-
and the prevalence of abnormal TSH and abnormal breath
ommendations await further research.
tests in IBS patients is similar to the prevalence of theseabnormalities in control populations (13, 14). Further re-view (Table 2.5.2) indicates that the pretest probability or
REFERENCES: SECTION 2.5
prevalence of inflammatory bowel disease and colorectal
1. Drossman DA. An integrated approach to the irritable bowel
cancer is not elevated among patients with IBS symptoms
syndrome. Aliment Pharmacol Ther 1999;13(suppl 2):3–14.
compared with that of control populations (15).
2. Camilleri M, Prather CM. The irritable bowel syndrome:
A single study (11) found that approximately 5% of
Mechanisms and practical approach to management. Ann In-tern Med 1992;116:1001– 8.
patients with IBS symptoms had celiac sprue, while the
3. American Gastroenterological Association Medical Position
prevalence of celiac sprue in a control population was less
Statement: Irritable bowel syndrome. Gastroenterology 1997;
than 1%. The prevalence of celiac sprue varies based on
heritage and across geographic region. Therefore, wide-
4. Schmulson MW, Chang L. Diagnostic approach to the patient
spread screening for celiac sprue with endomysial antibod-
with irritable bowel syndrome. Am J Med 1999;107:20S– 6S.
5. Camilleri M. Management of the irritable bowel syndrome.
ies is not routinely recommended for screening of patients
Gastroenterology 2001;120:652– 68.
with IBS symptoms until additional data are available to
6. Schoenfeld P, Guyatt G, Hamilton F, et al. An evidence-based
support this recommendation. A single study (12) of patients
approach to gastroenterology diagnosis. Gastroenterology
with IBS symptoms referred for breath tests to rule out
bacterial overgrowth syndrome found that 78% of these
7. Hamm LR, Sorrells SC, Harding JP, et al. Additional inves-
tigations fail to alter the diagnosis of irritable bowel syndrome
patients had bacterial overgrowth. Although these data are
in subjects fulfilling the ROME criteria. Am J Gastroenterol
provocative, this study examined a select population (i.e.,
patients referred for breath tests to rule out bacterial over-
8. Tolliver BA, Herrera JL, DiPalma JA. Evaluation of patients
Management of IBS Table 2.6.1. Trial Characteristics: Antispasmodic Agents
who meet clinical criteria for irritable bowel syndrome. Am J
or sublingual q.i.d. The systematic review was limited to
antispasmodic agents available in the United States.
9. MacIntosh DG, Thompson WG, Patel DG, et al. Is rectal
Eighteen RCTs evaluated the effectiveness of antispas-
biopsy necessary in irritable bowel syndrome? Am J Gastro-enterol 1992;87:1407–9.
modic agents available for the treatment of IBS (1–18), but
10. Francis CY, Duffy JN, Whorwell PJ, et al. Does routine
only three RCTs (1, 4, 12) evaluated the effectiveness of
ultrasound enhance diagnostic accuracy in irritable bowel syn-
dicyclomine and hyoscyamine (Table 2.6.1). Trials of dicy-
drome? Am J Gastroenterol 1996;91:1348 –50.
clomine and hyoscyamine were low-intermediate quality
11. Sanders DS, Carter MJ, Hurlstone DP, et al. Association of
(quality scores of 5–7 of possible 14) based on ROME
adult coeliac disease with irritable bowel syndrome: A case-control study in patients fulfilling the ROME II criteria re-
committee criteria for the design of treatment trials for
ferred to secondary care. Lancet 2001;358:1504 – 8.
functional GI disorders. None of these trials used ROME
12. Pimentel M, Chow EJ, Lin HC. Eradication of small intestinal
committee criteria (or Manning criteria) to identify IBS
bacterial overgrowth reduces symptoms of irritable bowel
patients, and none of the trials followed patients after dis-
syndrome. Am J Gastroenterol 2000;95:3503– 6.
continuation of therapy. Only one trial (12) was of at least
13. Helfand M, Redfern CC. Screening for thyroid disease: An
update. Ann Intern Med 1998;129:144 –158.
8 weeks duration. Sample sizes were not calculated a priori
14. Scrimshaw NS, Murray EB. The acceptability of milk and
in any of these trials, and all of these trials enrolled fewer
milk products in populations with a high prevalence of lactose
intolerance. Am J Clin Nutr 1988;48(4 suppl):1079 –159.
Only one (4) of the three studies (1, 4, 12) demonstrated
15. Cash BD, Schoenfeld P, Chey WD. The utility of diagnostic
tests in IBS patients: A systematic review. Am J Gastroenterol
a statistically significant improvement in global IBS symp-
toms with antispasmodic agents compared with placebo. This trial had poor study design (quality score of 5) and usedthe maximum dose of dicyclomine (40 mg q.i.d.), which
2.6 EFFECTIVENESS OF ANTISPASMODIC AGENTS IN
may have led to significantly more adverse events among
THE MANAGEMENT OF IRRITABLE BOWEL SYNDROME
dicyclomine-treated patients (69% vs 16% of placebo-
There are insufficient data to make a recommendation about
treated patients). Also, 15% of dicyclomine-treated patients
the effectiveness of the antispasmodic agents available in
withdrew from the study, while no placebo-treated patients
the United States (Grade B recommendation).
withdrew. In the other two studies (1, 12), no significant
While the exact pathophysiology of IBS remains un-
difference in outcomes was noted between patients treated
known, investigators have postulated that disturbances in
with antispasmodic agents and placebo.
intestinal motility result in symptoms of abdominal pain,
At higher doses, antispasmodic agents may exhibit atro-
bloating, and disturbed defecation. Antispasmodic agents
pine-like side effects related to their antimuscarinic proper-
include those that directly affect intestinal smooth muscle
ties. This atropine-like effect can lead to intolerance of the
relaxation (e.g., mebeverine, pinaverine) and those that act
agent because of visual disturbances, urinary retention, con-
in similar fashion via anticholinergic or antimuscarinic
stipation, and dry mouth. Data on adverse events demon-
properties (e.g., dicyclomine, hyoscyamine) (1–18). The
strate that increasing doses of anticholinergic compounds
mechanism of action of antispasmodics is likely through a
appear to produce more frequent adverse events (4, 20).
decrease in spontaneous activity of intestinal smooth mus-
Specific data on the effect of antispasmodic agents on the
cle. Outside the United States, several antispasmodic agents
frequency of bowel movements in constipated patients are
that directly affect intestinal smooth muscle relaxation (e.g.,
lacking. RCTs (20, 21) suggest that constipation is a poten-
mebeverine, pinaverine) are available (19). Currently, the
tial complication of antispasmodic agents, which is most
only antispasmodics available in the United States are di-
likely due to their muscle relaxant properties. Therefore,
cyclomine and hyoscyamine. The recommended dose for
Task Force members felt that antispasmodics should be used
dicyclomine is 20 – 40 mg by mouth q.i.d. (20), although
with caution among patients with constipation.
dicyclomine is commonly used at lower doses. The recom-
This review was limited to studies published in the En-
mended dose for hyoscyamine is 0.125– 0.25 mg by mouth
glish language. A previous meta-analysis (19) noted that one
ACG Functional GI Disorders Task Force
large trial of hyoscyamine had been published in German
blocker: A randomized double-blind placebo-controlled trial.
(22). Although this large (n ϭ 360), non-English language
Acta Gastroent Latinoamer 1995;25:137– 44.
15. Moshal MG, Herron M. A clinical trial of trimebutine (Me-
trial did not meet criteria for inclusion in this review, this
butin) in spastic colon. J Int Med Res 1979;7:231– 4.
trial found no difference between hyoscyamine and placebo
16. Battaglia G, Morselli-Labate AM, Camarri E, et al. Otilonium
for relief of abdominal pain or distention and no significant
bromide in irritable bowel syndrome: A double blind, placebo-
difference for global IBS symptom improvement. Previous
controlled, 1-week study. Aliment Pharmacol Ther 1998;12:
meta-analyses (19, 23) have produced conflicting recom-
17. CentonzeV, Imbimbo BP, Campanozzi F, et al. Oral ci-
mendations about the effectiveness of direct smooth muscle
metropium bromide, a new antimuscarinic drug, for long-term
relaxants available outside the United States. A complete
treatment of irritable bowel syndrome. Am J Gastroenterol
discussion of these agents (mebeverine, pinaverine, ci-
metropium, and otilonium) is beyond the scope of this
18. Ghidini O, Saponati G, Intrieri L. Single drug treatment for
monograph, but it should be noted that most RCTs of these
irritable colon: Rociverine versus trimebutine maleate. CurrTher Res 1986;39:541– 8.
agents demonstrate poor methodologic quality, limiting the
19. Poynard T, Regimbeau, Benhamou Y. Meta-analysis of
strength of recommendations based on these data.
smooth muscle relaxants in the treatment of irritable bowel
Overall, trials of therapy with antispasmodic agents were
syndrome. Aliment Pharmacol Ther 2001;15:355– 61. generally of short duration, studied small numbers of pa-
20. Package Insert. Dicyclomine. 21. Poynard T, Naveau S, Mory B, et al. Meta-analysis of smooth
tients, were of suboptimal quality, and demonstrated incon-
muscle relaxants in the treatment of IBS. Aliment Pharmacol
sistent effectiveness. Adverse events with these compoundslimit their dose range. Antispasmodics should be used with
22. Schafer VE, Ewe K. Behandlung des colon irritabile. Fortschr
caution in patients with constipation.
23. Jailwala J, Imperiale T, Kroenke K. Pharmacologic manage-
ment of IBS: A systematic review of randomized controlledtrials. Ann Intern Med 2000;133:136 – 47. REFERENCES: SECTION 2.6
1. Wheatley D. Irritable colon syndrome treated with an anti-
spasmodic drug. The Practitioner 1976;217:276 – 80. 2.7 EFFECTIVENESS OF BULKING AGENTS IN THE
2. Greenbaum DS, Ferguson RK, Kater LA, et al. A controlled
MANAGEMENT OF IRRITABLE BOWEL SYNDROME
therapeutic study of the irritable bowel syndrome. N EnglJ Med 1973;288:13– 6. Bulking agents commonly available in the United States are
3. Tasman-Jones C. Mebeverine in patients with the irritable
not more effective than placebo at relieving global IBS
colon syndrome: Double blind study. N Z Med J 1973;77:
symptoms (Grade B recommendation). Randomized con-trolled trials about treatment of IBS with laxatives have not
4. Page J, Dirnberger GM. Treatment of the irritable bowel
syndrome with bentyl (dicyclomine hydrochloride). J ClinGastroenterol 1981;3:153–56.
IBS patients with constipation exhibit delayed intestinal
5. Fielding JF. Double blind trial of trimebutine in the irritable
transit. Therefore, bulking agents that accelerate intestinal
bowel syndrome. Irish Med J 1980;73:377–9.
transit may be beneficial for these patients. Types of bulking
6. Luttecke K. A trial of trimebutine in spastic colon. J Int Med
agents studied include wheat bran, corn fiber, calcium poly-
carbophil, ispaghula husk, and psyllium. Psyllium husk is
7. Piai G, Mazzacca G. Pirifinium bromide in the treatment of the
irritable colon syndrome. Gastroenterology 1979;77:500 –2.
the outer coat of the psyllium seed (known in India as
8. Dobrilla G, Imbimbo BP, Piazzi L, et al. Longterm treatment
ispaghula seed) from the plant Plantago ovata.
of irritable bowel syndrome with cimetropium bromide: A
Thirteen RCTs evaluated the effectiveness of bulking
double blind placebo controlled trial. Gut 1990;31:355– 8.
agents in the treatment of IBS (1–13) (Table 2.7.1). These
9. Kruis W, Weinzierl M, Schussler P, et al. Comparison of the
trials were low-intermediate quality (quality scores 5–9 of
therapeutic effect of wheat bran, mebeverine and placebo in
possible 14) based on ROME committee criteria for the
patients with the irritable bowel syndrome. Digestion 1986;34:196 –201.
design of treatment trials for functional GI disorders. None
10. Piai G, Visconti M, Imbimbo BP, et al. Long-term treatment
of the trials used ROME committee criteria to identify IBS
of irritable bowel syndrome with cimetropium bromide, a new
patients as all of these trials were conducted before the first
antimuscarinic compound. Curr Ther Res 1987;41:967–77.
ROME committee conference was held. None of the trials
11. Luttecke K. A three-part controlled trial of trimebutine in the
followed patients after the cessation of study drug. Few
treatment of irritable colon syndrome. Curr Med Res Opin1980;6:437– 43.
trials were of at least 8 weeks in duration, used a parallel
12. Ritchie JA, Truelove SC. Treatment of irritable bowel syn-
study design, or reported the patient’s assessment of global
drome with lorazepam, hyoscine butylbromide, and ispaghula
IBS symptom improvement (Table 2.7.1). None pre-
sented sample size calculations, and most trials had small
13. Baldi, Longanesi A, Blasi A, et al. Clinical and functional
sample sizes (Ͻ30 patients), which could have led to
evaluation of the efficacy of otilonium bromide: A multicenterstudy in Italy. Ital J Gastroenterol 1991;23(suppl 1):60 –3.
14. Awad D, Dibildox M, Ortiz F. Irritable bowel syndrome
The single study of corn fiber (quality score ϭ 8) found
treatment using pinaverium bromide as a calcium channel
that pain severity, stool frequency, or stool consistency
Management of IBS Table 2.7.1. Trial Characteristics: Bulking Agents
improved with both corn fiber and placebo, but there was no
lism of fiber by intestinal bacteria (14, 15), and IBS
significant difference between the two. Pain frequency and
experts note that increases in fiber intake may increase
duration were not significantly improved with either agent
bloating and abdominal discomfort in IBS patients (16,
(1). The single study of calcium polycarbophil (quality
score ϭ 7) found no significant difference in overall
Overall, none of the trials of bulking agents demonstrated
preference but did report preference of calcium polycar-
high-quality methodology. Sample sizes in most of these
bophil in IBS patients with constipation or alternating
trials were particularly small, which could have produced
constipation and diarrhea. There was no significant dif-
Type II errors. Available evidence clearly indicates that
ference in abdominal pain between active agent and pla-
corn and wheat fiber are ineffective for global IBS symptom
cebo (7). Of the five trials (2– 6) of wheat bran (quality
improvement. Neither calcium polycarbophil nor psyllium
scores 5– 6), only one study (3) without a placebo control
was shown to be more effective than placebo for global IBS
found improvement in pain frequency, severity, and stool
symptom improvement. Although the majority of ispaghula
frequency with wheat bran. The other four were striking
husk studies demonstrated global improvement, this may
for the similarity in effectiveness for wheat bran and
have resulted from increasing frequency of bowel move-
placebo. The single study of psyllium (quality score ϭ 9)
ments in IBS patients with constipation. Although adverse
found that IBS symptoms were not improved with psyl-
event data from RCTs of fiber products are unavailable,
lium compared to placebo (8). Global IBS symptoms were
anecdotal experience and laboratory data suggest that fiber
improved in patients taking ispaghula husk in 4 of 5 studies
products increase intestinal gas, bloating, and abdominal
(9 –13) (quality scores 6 –9). In these studies, subgroup
discomfort in IBS patients. Therefore, fiber is appropriate
analysis of specific symptoms noted that abdominal pain
for treatment of constipation but may not be recommended
was not improved with ispaghula husk, but ease of bowel
movements was improved. The definition of global IBSsymptom improvement was poorly defined in many of thesestudies, making it difficult to determine if global IBS symp-
REFERENCES: SECTION 2.7
tom improvement simply reflected treatment of constipa-
1. Cook IJ, Irvine EJ, Campbell D, et al. Effect of dietary fiber on
tion. Patients in the negative study were all taking 30 g/day
symptoms and rectosigmoid motility in patients with irritable
of bran in addition to ispaghula husk or placebo.
bowel syndrome. Gastroenterology 1990;98:66 –72.
Data on adverse events associated with bulking agents
2. Soltoft J, Gudmand-Hoyer E, Krag B, et al. A double-blind
trial of the effect of wheat bran on symptoms of irritable
were not reported in these trials, precluding evidence-
bowel syndrome. Lancet 1976;1:270 –2.
based comments on possible adverse events associated
3. Manning AP, Heaton KW, Harvey RF, et al. Wheat fibre and
with bulking agents. Bowel gas is produced by metabo-
irritable bowel syndrome. Lancet 1977;2:417– 8. ACG Functional GI Disorders Task Force Table 2.8.1. Trial Characteristics: Antidiarrheal Agents
4. Arffmann S, Andersen JR, Hegnhoj J, et. al. The effect of
eramide is the only antidiarrheal agent appropriately eval-
coarse wheat bran in the irritable bowel syndrome. Scand J
uated for treatment of IBS, precluding evidence-based com-
ments about the effectiveness of other antidiarrheal agents.
5. Lucey MR, Clark ML, Lowndes JO, et al. Is bran efficacious
in irritable bowel syndrome? A double-blind, placebo con-
In these trials, loperamide has been used in dosages of 2–12
trolled crossover study. Gut 1987;28:221–5.
6. Snook J, Shepherd HA. Bran supplementation in the treatment
Three RCTs evaluated the effectiveness of loperamide in
of irritable bowel syndrome. Aliment Pharmacol Ther 1994;
the treatment of IBS (3–5) (Table 2.8.1). These trials were
low-intermediate quality (quality scores ranging from 5 to 7
7. Toskes PP, Connery KL, Ritchey TW. Calcium polycarbophil
compared with placebo in irritable bowel syndrome. Aliment
of possible 14). None of the trials used ROME committee
criteria to identify IBS patients as all of these trials were
8. Longstreth GF, Fox DD, Youkeles L, et al. Psyllium therapy
conducted before the first ROME committee conferences
for irritable bowel syndrome. Ann Intern Med 1981;95:53– 6.
were held. None of the trials was longer than 5 weeks in
9. Ritchie JA, Truelove SC. Treatment of irritable bowel syn-
drome with lorazepam, hyoscine butylbromide, and ispaghula
duration, and none presented sample size calculations. All
trials had relatively small sample sizes (30 –90 patients),
10. Golechha AC, Chadda VS, Chadda S, et al. Role of ispaghula
which could have led to Type II errors.
husk in the management of irritable bowel syndrome (a ran-
In the first study (3), loperamide decreased stool fre-
domized double-blind crossover study). J Assoc Physicians
quency from 1.9/day to 1.3/day, decreased the percentage
11. Arthurs Y, Fielding JF. Double blind trial of ispaghula/polax-
of unformed stools from 60% to 31%, and decreased the
amer in the irritable bowel syndrome. Irish Med J 1983;76:
incidence of urgency from 2.4 days/wk to 1.1 days/wk
(all p Ͻ 0.05). Placebo produced no significant decrease
12. Prior A, Whorwell PJ. Double blind study of ispaghula in
in these outcomes. There was no significant difference in
irritable bowel syndrome. Gut 1987;28:1510 –3.
abdominal distension or abdominal pain with either lop-
13. Jalihal A, Kurian G. Ispaghula therapy in irritable bowel
syndrome: improvement in overall well-being is related to
eramide or placebo. There was no significant difference
reduction in bowel dissatisfaction. J Gastroenterol Hepatol
in global IBS symptom improvement between loperam-
ide-using patients and placebo-using patients. In the sec-
14. Haderstorfer B, Psycholgin D, Whitehead WE, et al. Intestinal
ond study (4), results were only reported for patient
gas production from bacterial fermentation of undigested car-bohydrate in IBS. Am J Gastroenterol 1989;84:375– 8.
subgroups defined by the investigators: patients with
15. Lasser RB, Levitt MD. The role of intestinal gas in functional
painless diarrhea, patients with painless constipation, pa-
abdominal pain. N Engl J Med 1975;293:524 – 6.
tients with pain and alternating diarrhea and constipation,
16. Francis CY, Whorwell PJ. Bran and IBS: Time for reappraisal.
and patients without pain but with alternating diarrhea
and constipation. Among patients with painless diarrhea,
17. Camilleri M. Review article: Clinical evidence to support
current therapies of IBS. Aliment Pharmacol Ther 1999;
loperamide-using patients were more likely than placebo-
using patients to note improvement in stool frequency(100% vs 40%), stool consistency (100% vs 50%), and
2.8 EFFECTIVENESS OF THE ANTIDIARRHEAL AGENT
overall symptoms (100% vs 25%) (p Ͻ 0.01 for alloutcomes). Among patients without pain who alternated
LOPERAMIDE IN THE MANAGEMENT OF IRRITABLE
between constipation and diarrhea, there was no signifi-
BOWEL SYNDROME
cant difference between loperamide and placebo. Among
The antidiarrheal agent loperamide is not more effective
patients with painless constipation, loperamide-using pa-
than placebo at relieving global IBS symptoms (Grade B
tients had “worse” symptoms, but such worsening was
recommendation). Randomized controlled trials about
not significantly different from placebo-using patients. treatment of IBS with other antidiarrheal agents have not
Among patients with pain who alternated between con-
stipation and diarrhea, loperamide-using patients im-
IBS patients with diarrhea demonstrate accelerated intes-
proved significantly more than placebo-using patients
tinal transit (1, 2). Therefore, antidiarrheal agents that delay
with regard to stool frequency (95% vs 25%) and stool
intestinal transit may be beneficial for these patients. Lop-
consistency (95% vs 45%) (p Ͻ 0.02 for both). In the
Management of IBS Table 2.9.1. Trial Characteristics: Antidepressant Agents
third study (5), loperamide-using patients improved sig-
2.9 EFFECTIVENESS OF ANTIDEPRESSANTS IN THE
nificantly more than placebo-using patients with regard to
MANAGEMENT OF IRRITABLE BOWEL SYNDROME
stool frequency (35% vs 10%) and stool consistency(50% vs 20%) during weeks one to five (p Ͻ 0.05). There
Tricyclic antidepressants (TCAs) are not more effective than
was no significant difference in abdominal pain. Improve-
placebo at relieving global IBS symptoms. TCAs improve
ment in global IBS symptoms was not reported. abdominal pain in IBS patients (Grade B recommendation).
Only one study (1) reported data on adverse events. In
Randomized controlled trials about the effectiveness of se-
this trial, 29% of loperamide-treated patients reported ad-
lective serotonin re-uptake inhibitors (SSRIs) in the treat-
verse events vs 36% of placebo-treated patients (p Ͼ 0.05). ment of IBS have not been published in manuscript form.
No other details were provided. Because of the relative lack
IBS patients exhibit visceral hypersensitivity. In other
of adverse event data, no evidence-based comments about
words, IBS patients sense pain or discomfort with less
possible adverse events associated with loperamide can be
distention of the colon than do control patients. TCAs,including doxepin, desipramine, amitriptyline, and trimipra-
mine, ameliorate enhanced nociception and may treat the
Overall, none of the trials of antidiarrheal agents (e.g.,
chronic pain of IBS patients. By decreasing the experience
loperamide) demonstrated high-quality methodology.
of abdominal pain, TCAs enhance the patient’s sense of
Trial results indicate that loperamide is an effective
well-being and decrease their distress from their IBS symp-
treatment for diarrhea, but loperamide is not more effec-
toms. For the management of chronic pain, TCAs were
tive than placebo for treatment of global IBS symptoms or
prescribed in doses that were subtherapeutic for the treat-
abdominal pain. Adverse event data are sparse. Given the
ment of depression but were appropriate for the manage-
mechanisms of action of loperamide, it should not be usedin IBS patients with constipation, and it should be used
Seven RCTs evaluated the effectiveness of TCAs in the
with caution in IBS patients alternating between diarrhea
treatment of IBS (1–7). One RCT was eliminated from
analysis because the dropout rate was 45% (7). Of the sixremaining trials (Table 2.9.1), all were of low quality (qual-ity scores of 5– 6 of possible 14) based on ROME committee
REFERENCES: SECTION 2.8
criteria for the design of treatment trials of functional GIdisorders. None of the studies used ROME committee cri-
1. Vassallo MJ, Camilleri M, Phillips SF, et al. Colonic tone and
teria to identify IBS patients, measured compliance, or pre-
motility in patients with IBS. Mayo Clin Proc 1992;67:725–31.
sented sample size calculations. Most trials had small sam-
2. Camilleri M. Review article: Clinical evidence to support cur-
rent therapies of IBS. Aliment Pharmacol Ther 1999;13(suppl
ple sizes (Յ31 patients) in each arm, and no trial was more
than 8 weeks in duration. In addition to these limitations in
3. Cann PA, Read NW, Holdsworth CD, et al. Role of loperamide
study design, primary and secondary study endpoints were
and placebo in management of irritable bowel syndrome (IBS).
poorly defined. Frequently, results were not presented in a
straightforward fashion. These additional flaws made inter-
4. Hovdenak N. Loperamide treatment of the irritable bowel syn-
pretation of study results difficult. This is not surprising, as
drome. Scand J Gastroenterol Suppl 1987;130:81– 4.
5. Efskind PS, Bernklev T, Vatn MH. A double-blind placebo-
almost all of these studies were performed prior to the
controlled trial with loperamide in irritable bowel syndrome.
publication of standards for the design of treatment trials for
Scand J Gastroenterol 1996;31:463– 8. ACG Functional GI Disorders Task Force
Two studies examined the effectiveness of desipramine
methods and results. The second meta-analysis indicated
(1, 5). In the first study (1), global improvement of IBS
that TCAs improve the symptoms of functional GI disor-
symptoms was not measured, although 92% (12/13) of
ders, although it may not have adequately accounted for the
desipramine-using patients noted improvement in interfer-
limitations in design of these studies and the flaws in re-
ence of IBS symptoms with daily life compared with 60%
(9/15) of placebo-using patients (p Ͼ 0.05). In the second
In these trials, TCAs were not used in therapeutic doses
trial (5), a p value was not reported for analysis of global
for treatment of depression but were used at lower doses for
improvement in IBS symptoms, although 54% (15/28) of
the management of chronic pain. Overall, trials of therapy
desipramine-using patients had global improvement com-
with TCAs were of short duration and examined small
pared with 18% (5/28) of placebo-using patients and 21%
numbers of patients and study designs were suboptimal.
(6/28) of atropine-using patients. Abdominal pain was im-
Evidence is inadequate to support the effectiveness of TCAs
proved with desipramine in both studies, achieving statisti-
for improvement of global IBS symptoms. There is, however,
cal significance in one (5) among patients with IBS with
limited evidence that TCAs may decrease abdominal pain.
diarrhea only. In the single study of amitriptyline (2), “im-
Adverse event data with TCAs indicate that these agents
provement” in symptoms was noted more often with drug
may cause constipation and should be used with caution in
than placebo, but the p value was 0.08 and the supporting
tables were not interpretable. There were no significantdifferences in improvement of individual symptoms be-
REFERENCES: SECTION 2.9
tween amitriptyline and placebo. Two studies from one
1. Heefner JD, Wilder RM, Wilson ID. Irritable colon and de-
group of investigators assessed trimipramine (3, 4). In the
pression. Psychosomatics 1978;19:540 –7.
first, patients taking trimipramine had significantly greater
2. Steinhart MJ, Wong PY, Zarr ML. Therapeutic usefulness of
improvement in scores for vomiting, sleeplessness, depres-
amitriptyline in spastic colon syndrome. Int J Psychiatry Med
sion, and mucus in stools. There was no significant differ-
ence in scores for pain, belching, headache, and tiredness.
3. Myren J, Groth H, Larssen S-E, et al. The effect of trimipra-
mine in patients with irritable bowel syndrome. Scand J Gas-
Overall symptom improvement occurred in 25/30 (83%)
patients taking drug compared with 21/31 (68%) taking
4. Myren J, Lovland B, Larssen S-E, et al. A double-blind study
placebo, but no p value was reported. In the follow-up study,
of the effect of trimipramine in patients with irritable bowel
trimipramine was given in three different doses. Scores for
syndrome. Scand J Gastroenterol 1984;19:835– 43.
abdominal pain were significantly better than placebo only
5. Greenbaum DS, Mayle JE, Vanegeren LE, et al. Effects of
desipramine on irritable bowel syndrome compared with at-
for the 50-mg dose. The single study of doxepin reported
ropine and placebo. Dig Dis Sci 1987;32:257– 66.
significant overall clinical improvement for drug compared
6. Vij JG, Jiloha RG, Kumar N, et al. Effect of antidepressant
to placebo (11/21 [55%] vs 5/23 [21%]). Abdominal pain
drug (doxepin) on irritable bowel syndrome patients. Indian
improved in 56% of patients taking doxepin compared with
7. Rajagopalan M, Kurian G, John J. Symptom relief with ami-
triptyline in the irritable bowel syndrome. J Gastroenterol
Adverse events were sporadically reported in these trials.
Constipation was significantly worse for desipramine-using
8. Creed FH, Fernandes L, Guthrie E, et al. The cost-effective-
patients than for atropine-using patients in one trial (5).
ness of psychotherapy and SSRI antidepressants for severe
“Tiredness” was significantly worse in trimipramine-using
irritable bowel syndrome. Gastroenterology 2001;120:A115.
patients compared with control patients during the first two
9. Tanum L, Malt UF. A new pharmacologic treatment of func-
tional GI disorders: A double-blind placebo-controlled study
with mianserin. Scand J Gastroenterol 1996;31:318 –25.
This review was limited to trials published in full manu-
10. Clouse RE, Prakash C, Anderson RJ, et al. Antidepressants for
script form and to medications available in the United
functional gastrointestinal symptoms and syndromes: A meta-
States. One abstract (8) evaluated the effectiveness of par-
analysis. Gastroenterology 2001;120:A642.
oxetine, an SSRI, for the treatment of IBS and reportedly
11. Jackson JL, O’Malley PG, Tomkins G, et al. Treatment of
functional gastrointestinal disorders with antidepressant
demonstrated improvement in symptoms; however, the
medications: A meta-analysis. Am J Med 2000;108:65–72.
methodology and full results of this trial are not available,precluding evidence-based recommendations about the ef-
2.10 EFFECTIVENESS OF THE 5HT (SEROTONIN)
fectiveness of SSRIs. Mianserin, which blocks noradrena-
RECEPTOR AGONIST TEGASEROD IN THE MANAGEMENT
line re-uptake, is another antidepressant that has been eval-
OF IRRITABLE BOWEL SYNDROME
uated for treatment of functional GI disorders (9), but it isnot available in the United States. Meta-analyses did not
The 5HT receptor agonist tegaserod is more effective than
serve as the basis for evidence-based recommendations,
placebo at relieving global IBS symptom in female IBS
although two meta-analyses (10, 11) have evaluated the
patients with constipation (Grade A recommendation).
effectiveness of TCAs to improve symptoms in functional
Currently, the only available 5HT (serotonin) receptor
GI disorders. One meta-analysis (10) has only been pub-
agonist is tegaserod. This agent stimulates the peristaltic
lished in abstract form, precluding a full evaluation of its
reflex, increases intestinal and colonic transit, reduces the
Management of IBS Table 2.10.1. Trial Characteristics: 5-HT Receptor Agonist Tegaserod
Muller-Lissner Tegaserod vs placebo 6 mg b.i.d. Parallel
Tegaserod vs placebo 6 mg b.i.d. Parallel
Tegaserod vs placebo 6 mg b.i.d. Parallel
Tegaserod vs placebo 6 mg b.i.d. Parallel
* Study 307 (9) did not treat patients with the approved dosage (6 mg b.i.d.) throughout the trial. Therefore, it is not included in this analysis.
firing rate of rectal afferent nerves, and reduces visceral
All four trials of tegaserod 6 mg b.i.d. (1, 4 – 8) demon-
sensitivity (1–3). Tegaserod is the only FDA-approved
strated statistically significant improvement in global IBS
agent for the treatment of IBS patients with constipation.
symptoms for tegaserod-using patients compared with pla-
The recommended dosage is 6 mg b.i.d., and the following
cebo-using patients. Based on the prescribed endpoint, ap-
analysis will be limited to results achieved with this dose.
proximately 5–19% more tegaserod-using patients had sig-
Four RCTs have evaluated the effectiveness of tegaserod
nificant improvement in global IBS symptoms compared
6 mg b.i.d. in the management of IBS (1, 4 – 8) (Table
with placebo-using patients (Figure 2.10.1). In subgroup
2.10.1). All of these trials were high-quality trials (quality
analysis, tegaserod-using patients experienced less bloating,
scores of 12–13 of possible 14) based on ROME committee
less abdominal discomfort, and improved satisfaction with
criteria for the design of treatment trials for functional
their bowel habits compared with placebo-using patients (1,
gastrointestinal disorders. Trial duration was 12 weeks in all
4, 6). The magnitude of these improvements varied across
trials. The patient population in these trials was Ͼ80%
trials as a result of the use of different scales to measure
women and Ͼ80% Caucasian and had a mean age of ap-
individual symptoms in different trials.
proximately 45 years and mean duration of IBS symptoms
Diarrhea is the most common adverse event associated
of more than 10 years (6). Patients met ROME I criteria for
with tegaserod use and was reported as an adverse event in
the diagnosis of IBS. Most patients met criteria for IBS with
9 –10% of tegaserod-using patients vs 4 –5% of placebo-
constipation, although a minority of patients had IBS with
using patients (1, 4 –7, 9). Approximately 1–2% of tegas-
bowel habits alternating between constipation and diarrhea.
erod-using patients discontinued medication because of this
A comprehensive evaluation of the tegaserod data reveals
adverse event. Among tegaserod-using IBS patients and
some variability in study methodology. The definition of
placebo-using IBS patients, the rates of abdominal surgery
global IBS symptom improvement was changed after data
and ovarian cyst formation were similar.
analysis of the first clinical trial (5) because this definition
When prescribing tegaserod, physicians should remem-
was not sensitive enough to detect changes in global IBS
ber that the FDA-approved indication for tegaserod is
symptoms (1). Therefore, the first clinical trial (5) used a
“for the short-term treatment of women with IBS whose
retrospectively defined study endpoint. Global IBS symp-
primary bowel symptom is constipation.” Secondary
tom improvement was determined based on IBS symptoms
analysis demonstrated significant increase in frequency of
during the last 4 weeks of 12-week trials, although numer-ically larger differences between tegaserod and placebowere seen with 12-week longitudinal analyses or analyses ofIBS symptoms during the first 4 weeks. In the most recentstudy (8), improvement in global IBS symptoms was mea-sured during the first 4 weeks of the trial with a binaryendpoint (i.e., IBS symptoms improved vs IBS symptomsnot improved). This trial produced the largest numericalbenefit observed with tegaserod. Thus, the definition ofglobal IBS symptom improvement appears to influence themagnitude of benefit observed with tegaserod. Finally, oneRCT (9) is not presented in this analysis as this was adose-ranging trial and no patients took the approved dosage
Figure 2.10.1. Percentage of patients with improvement in global
of tegaserod (6 mg b.i.d.) throughout the trial. ACG Functional GI Disorders Task Force
bowel movements for tegaserod-using male patients com-
2.11. EFFECTIVENESS OF THE 5HT (SEROTONIN)
pared with placebo-using male patients and a nonstatis-
RECEPTOR ANTAGONIST ALOSETRON IN THE
tically significant trend for improvement in global IBS
MANAGEMENT OF IRRITABLE BOWEL SYNDROME
symptoms. Because of the relatively small sample of menin these trials, this finding could represent a Type II error. The 5HT receptor antagonist alosetron is more effective
Randomized controlled trial data demonstrate effective-
than placebo at relieving global IBS symptoms in female IBSpatients with diarrhea (Grade A recommendation).
ness of tegaserod up to 12 weeks. Given the episodic and
Currently, the only available 5HT (serotonin) receptor
fluctuating course of IBS, intermittent therapy appears
antagonist is alosetron. This agent slows colonic transit and
appropriate. The effectiveness of long-term maintenance
decreases discomfort during distension of the colon (1, 2).
therapy requires further study. Finally, some patients
Alosetron is the only FDA-approved agent for the treatment
with IBS alternating between diarrhea and constipation
of IBS patients with diarrhea. In November 2000, distribu-
were included in these trials, but the effectiveness of
tion of alosetron was halted because of concerns about
tegaserod in this subgroup of IBS patients has not been
ischemic colitis and serious complications of constipation.
In June 2002, the FDA approved restricted marketing of
Overall, the trials of tegaserod consistently demonstrate
alosetron for “the treatment of women with severe, diarrhea-
high-quality study methodology and effectiveness for the
predominant IBS who have failed to respond to conven-
treatment of IBS with constipation. The ability to generalize
tional IBS therapy.” The recommended dosage is 1 mg
trial results to male IBS patients and IBS “alternators” is
b.i.d., and the following analysis will be limited to results
not adequately defined. As diarrhea is the most commonadverse event associated with tegaserod use, it may be
Four RCTs have evaluated the effectiveness of alosetron
prudent to advise patients to temporarily discontinue tega-
1 mg b.i.d. in the management of IBS (3– 6) (Table 2.11.1). serod if significant diarrhea occurs.
All of these trials were high-quality trials (quality scores of12 of possible 14) based on ROME committee criteria forthe design of treatment trials for functional GI disorders. Patients met ROME I or ROME II criteria for the diagnosisof IBS. Most patients had IBS with diarrhea, and a minority
REFERENCES: SECTION 2.10
had IBS with bowel habits alternating between diarrhea andconstipation. The patient population in these trials was
1. Camilleri M. Review article: Tegaserod. Aliment Pharmacol
Ͼ90% women and Ͼ90% Caucasian and had a mean age of
2. Prather CM, Camilleri M, Zinsmeister AR, et al. Tegaserod
A comprehensive evaluation of the alosetron data reveals
accelerates oro-cecal transit in patients with constipation-pre-dominant irritable bowel syndrome. Gastroenterology 2000;
several methodologic issues. First, three of these trials (3–5)
were conducted before publication of ROME committee
3. Degen L, Matzinger D, Merz M, et al. Tegaserod, a 5-HT
recommendations about the design of treatment trials for
receptor partial agonist, accelerates gastric emptying and gas-
functional GI disorders. Thus, only one trial (6) used global
trointestinal transit in healthy male subjects. Aliment Pharma-
IBS symptom improvement as a secondary endpoint. Im-
provement in abdominal pain or improvement in fecal ur-
4. Muller-Lissner S, Fumagalli I, Bardhan KD, et al. Tegaserod, a
gency was the primary endpoint in these trials, although
5-HT4 receptor partial agonist, relieves symptoms in irritablebowel syndrome patients with abdominal pain, bloating, and
individual IBS symptoms of stool consistency, stool fre-
constipation. Aliment Pharmacol Ther 2001;15:1655– 66.
quency, and satisfaction with bowel habits were examined
5. Whorwell PJ, Krumholz S, Muller-Lissner S, et al. Tegaserod
in all trials. The definition of a “responder” for symptom
has a favorable safety and tolerability profile in patients with
improvement was not consistent across trials, limiting com-
constipation-predominant and alternating forms of irritable
parisons between trials. One RCT (4) compared alosetron
bowel syndrome. Gastroenterology 2000;118:A1204.
with an active control, mebeverine. One additional RCT (7)
6. Schoenfeld P, Chey W, Drossman D, et al. Effectiveness and
is not presented in this analysis as this was a dose-ranging
safety of tegaserod in the treatment of irritable bowel syndrome:a meta-analysis of randomized controlled trials. Gastroenterol-
trial and no patients took the approved dose of alosetron (1
7. Novick J, Miner P, Krause R, et al. A randomized, double-
All four trials (3– 6) demonstrated statistically significant
blind, placebo-controlled trial of tegaserod in female patients
improvement in the primary study endpoint (i.e., improve-
suffering from irritable bowel syndrome with constipation. Al-
ment in abdominal pain or improvement in fecal urgency)
iment Pharmacol Ther 2002;16:1877– 88.
for alosetron-using patients vs control patients. Based on the
8. Kellow J, Lee O, Chang F, et al. Tegaserod is an effective
prescribed definition for improvement in abdominal pain,
therapy for non-diarrheal IBS in an Asian-Pacific population. Gut (in press) (Abstract).
approximately 10 –27% more alosetron-using patients had
9. Study #307. Data on file. Novartis Pharmaceuticals Corpora-
significant improvement in abdominal pain compared with
control patients (Figure 2.11.1). In the single study measur-
Management of IBS Table 2.11.1. Trial Characteristics: 5-HT Receptor Antagonist Alosetron
Camilleri (3) Alosetron vs placebo 1, 2, 4 or 8 mg b.i.d. Parallel
Camilleri (5) Alosetron vs placebo 1 mg b.i.d.
symptoms, global IBSsymptom improvement,adverse events
* Primary outcome measure was relief of abdominal pain in three trials (3–5) and was relief of fecal urgency in one trial (6).
ing global IBS symptom improvement (6), approximately
pected ischemic colitis and 113 cases of suspected serious
32% more alosetron-using patients noted significant im-
constipation complications associated with alosetron use.
provement in global IBS symptoms compared with control
Based on available data, the proportion of IBS patients with
patients (76% vs 44%, respectively; p Ͻ 0.01). In analysis
diarrhea who develop ischemic colitis or serious constipa-
of individual IBS symptoms, alosetron-using patients con-
sistently demonstrated significant improvement in stool fre-
When prescribing alosetron, physicians should consider
quency, stool consistency, and fecal urgency compared with
the following issues. Since three of the four RCTs examined
control patients. The magnitude of these improvements var-
only women, the effectiveness of this agent in men is un-
ied across trials owing to the use of different scales to
clear. RCT data on the effectiveness of alosetron are only
measure individual symptoms in different trials.
available from 12-week trials. The appropriate duration of
Constipation is the most common adverse event associ-
treatment with alosetron is uncertain. Although global IBS
ated with use of alosetron. In these trials (3– 6), constipation
symptom improvement was not the primary study endpoint
was reported as an adverse event in 22–39% of alosetron-
in these trials, all of these trials assessed improvement in
using patients vs 3–14% of control patients, and approxi-
multiple IBS symptoms, and alosetron was consistently
mately 10% of alosetron-using patients discontinued medi-
better than control agents for improvement in all of these
cation because of this adverse event. Two cases of ischemic
symptoms. As constipation is the most common adverse
colitis were reported in these trials, although pathologic
event associated with alosetron use, it may be prudent to
examination of the surgical specimen in one case revealed
advise patients to temporarily discontinue alosetron if sig-
that the cause of colitis was Escherichia coli O157:H7.
nificant constipation occurs. Physicians should follow FDA
Another trial (4) reported a case of “colitis/sigmoiditis,” but
guidelines for use of alosetron: 1) alosetron is prescribed for
it was unclear if this case was consistent with ischemic
“women with severe, diarrhea-predominant IBS who have
colitis. In March 2002, the FDA reported 84 cases of sus-
failed conventional IBS therapy”; 2) physicians must edu-cate patients about the potential risks of alosetron use; and,3) patients should assess the risk-benefit ratio before decid-ing to use alosetron. Overall, the trials of alosetron consistently demonstratehigh-quality study methodology and effectiveness for thetreatment of IBS with diarrhea in women. Physicians shouldfollow the FDA-approved indication for alosetron: “womenwith severe, diarrhea-predominant IBS who have failed torespond to conventional IBS therapy.” Therefore, given therisk of serious adverse events with alosetron, physician andpatient judgment will guide selection of patients who areappropriate candidates for alosetron. Physicians shouldeducate patients about the potential risks of alosetron andinstruct patients to discontinue alosetron if constipationFigure 2.11.1. Percentage of patients with improvement in abdom- inal pain. ACG Functional GI Disorders Task Force REFERENCES: SECTION 2.11 Table 2.12.1. Behavioral Therapies for Treatment of IBS
1. Relaxation therapy: Based on the hypothesis that stress
1. Forster JM, Houghton LA, Whorwell PJ. Alosetron slows co-
stimulates the autonomic nervous system and exacerbates IBS
lonic transit in patients with irritable bowel syndrome. Gastro-
symptoms. Patients learn techniques to release tension and relax.
enterology 1996;110:A630 1996;110:A630 (abstract).
2. Biofeedback: Patients learn to sense changes in rectal
2. Delvaux M, Louvel D, Mamet JP, et al. Effect of alosetron on
distention and to regulate bowel habits using biofeedback
responses to colonic distension in patients with irritable bowel
syndrome. Aliment Pharmacol Ther 1998;12:849 –55.
3. Hypnotherapy: Based on the hypothesis that hypnotherapy
3. Camilleri M, Mayer E, Drossman D, et al. Improvement in pain
may induce a lasting state of relaxation and may positively
and bowel function in female irritable bowel syndrome patients
affect gut motility and intestinal smooth muscle contraction.
with alosetron, a 5HT3 receptor antagonist. Aliment Pharmacol
4. Cognitive therapy: Based on the hypothesis that patient’s
learned resposne to stressful events exacerbates IBS
4. Jones R, Holmann G, Rodrigo L, et al. Alosetron relieves pain
symptoms. In cognitive therapy, patients accept responsibility
and improves bowel function compared with mebeverine in
for their IBS symptoms, learn to identify stressful events and
female non-constipated irritable bowel syndrome patients. Al-
actively seek solutions to these events.
iment Pharmacol Ther 1999;13:1419 –27.
5. Psychotherapy: Based on the hypothesis that IBS symptoms
5. Camilleri M, Northcutt AR, Kong S, et al. The efficacy and
may be a manifestation of traumatic life events.
safety of alosetron in female patients with irritable bowel
Psychotherapy provides insight about these life events and
syndrome: A randomized, placebo controlled study. Lancet
the association between these events and IBS symptoms.
Through this insight, patients may experience long-term
6. Lembo T, Wright RA, Bagby B, et al. Alosetron controls bowel
urgency and provides global symptom improvement in womenwith diarrhea-predominant irritable bowel syndrome. Am JGastroenterol 2001;96:2662–70.
7. Bardhan K, Bodemar G, Geldor H, et al. A double-blind pla-
of these studies enrolled an inadequate sample of patients.
cebo-controlled study to evaluate the efficacy of alosetron in the
Generally, sample sizes were small with almost all studies
treatment of irritable bowel syndrome. Aliment Pharmacol Ther
Previous reviews have noted multiple biases unique to
2.12 EFFECTIVENESS OF BEHAVIORAL THERAPY IN THE
behavioral therapy studies (3). Attention from health careproviders may produce therapeutic benefits (3). These ben-
MANAGEMENT OF IRRITABLE BOWEL SYNDROME
efits may derive from: 1) the empathic attitude of the pro-
Behavioral therapy is more effective than placebo at reliev-
vider toward patient’s symptoms and life stresses; 2) the
ing individual IBS symptoms (Grade B recommendation).
enthusiasm of the provider about the effectiveness of the
Psychological disorders, especially depression and anxi-
therapy; and, 3) the quality and quantity of contact time with
ety disorders, are comorbid conditions in most IBS patients
the provider; however, only two studies (12, 15) attempted
who actively seek subspecialist medical care. Of IBS pa-
to control for differences in attention from health care pro-
tients who actively sought subspecialist medical care, 54 –
viders. Expectancy of improvement with behavioral therapy
94% met DSM-III-R criteria for a primary (Axis I) psycho-
may also influence results and should be measured pre- and
logical disorder (1), but only 18% of IBS patients in a
post-therapy (3) (i.e., if a patient expects that behavioral
population-based study met DSM-III criteria for a primary
therapy will improve IBS symptoms, then this expectation
psychiatric disorder (2). Comorbid psychological disorders
will bias the patient’s assessment of IBS symptom improve-
may influence health-care seeking behaviors of IBS patients,
ments). Controlling for patient expectations is particularly
but these psychological disorders are not the cause of IBS
important in unblinded trials, but only two trials (12, 13)
symptoms. Given the overlap between psychological disor-
assessed patients’ expectations of improvement with behav-
ders and IBS, behavioral therapies (Table 2.12.1) have been
ioral therapy. Future behavioral therapy studies of IBS pa-
tients should adhere to published recommendations for the
Sixteen RCTs have evaluated the effectiveness of behavioral
therapies in the management of IBS (4 –19) (Table 2.12.2).
Eleven studies reported that behavioral therapy improved
Multiple studies combined different types of behavioral ther-
individual IBS symptoms (5–11, 16 –19), and five studies (4,
apy (e.g., relaxation therapy plus biofeedback) into a multi-
12–15) did not demonstrate a statistically significant im-
component behavioral therapy (Table 2.12.2). Behavioral ther-
provement in IBS symptoms between treatment and control
apy trials were of intermediate quality (quality scores 7–10 of
groups (Table 2.12.2). Results provided some support of
possible 14) based on ROME committee criteria for the design
effectiveness with all types of behavioral therapy, including
of treatment trials for functional GI disorders. In most trials,
relaxation therapy, biofeedback, hypnotherapy, cognitive
more than 80% of patients had a concurrent psychological
therapy, psychotherapy, and different combinations of these
disorder with IBS. None of these trials used adequate blinding,
behavioral therapies (Table 2.12.2). Improvement in indi-
although complete blinding in behavioral therapy studies is
vidual IBS symptoms correlated with improvement in psy-
difficult. None of the trials evaluated improvement in global
chological symptoms in most trials. As noted above, atten-
IBS symptoms, and all trials evaluated individual IBS symp-
tion from health care providers may positively affect
toms. Only two studies (12, 13) reported sample sizes, and one
patient’s symptoms, but only two trials (12, 15) adequately
Management of IBS Table 2.12.2. Trial Characteristics: Behavioral Therapy ACG Functional GI Disorders Task Force Table 2.12.2. Trial Characteristics: Behavioral Therapy (continued)
* Study outcome: (ϩ) indicates that treatment patients demonstrated significantly more improvements in IBS symptoms compared with controls; (Ϫ) indicates that treatmentpatients did not demonstrate significantly more improvement in IBS symptoms compared with controls.
controlled for this variable. Neither of these trials showed a
6. Greene B, Blanchard EB. Cognitive therapy for irritable bowel
significant difference in IBS symptom improvement be-
syndrome. J Consult Clin Psychol 1994;62:576 – 82.
tween treatment patients and control patients, although IBS
7. Guthrie E, Creed F, Dawson D, et al. A randomized controlled
trial of psychotherapy in patients with refractory irritable
symptoms improved from baseline in both groups. This
bowel syndrome. Br J Psychiatry 1993;163:315–321.
finding suggests that IBS symptom improvement may result
8. Lynch PM, Zamble EA. Controlled behavioural treatment study
from attention given by health care providers and may not
of irritable bowel syndrome. Behav Ther 1989;20:509 –23.
result from specific behavioral therapy (20).
9. Shaw G, Srivistava ED, Sadlier M, et al. Stress management
No adverse events were reported with hynotherapy, psy-
for irritable bowel syndrome: A controlled trial. Digestion1991;50:36 – 42.
chotherapy, cognitive therapy, or biofeedback using a bal-
10. Svedlund J, Sjodin I, Ottoson JO, et al. Controlled study of
psychotherapy in irritable syndrome. Lancet 1983;2:589 –92. Psychological disorders and IBS are frequently comorbid
11. Whorwell PJ, Prior A, Farragher EB. Controlled trial of hyp-
conditions among patients who actively seek subspecialist
notherapy in the treatment of severe refractory irritable bowel
medical care for IBS. None of the trials of behavioraltherapies demonstrated high-quality methodology. These
12. Blanchard EB, Schwarz SP, Suls JM, et al. Two controlled
evaluations of multicomponent psychological treatment of ir-
trials lacked adequate blinding and rarely corrected for
ritable bowel syndrome (study 1). Behav Res Ther 1992;30:175–
differences in attention from health care providers. Trialresults suggest that relaxation therapy, hypnotherapy,
13. Blanchard EB, Schwarz SP, Suls JM, et al. Two controlled
biofeedback, cognitive therapy, and psychotherapy may im-
evaluations of multicomponent psychological treatment of irrita-
prove individual IBS symptoms. Behavioral therapy im-
ble bowel syndrome (study 2). Behav Res Ther 1992; 30:175– 89.
14. Corney RH, Stanton R, Newell R, et al. Behavioural psycho-
proved both IBS symptoms and psychological symptoms
therapy in the treatment of irritable bowel syndrome. J Psy-
among patients with comorbid psychological disorders;however, given the limitations of trial design, “no trial has
15. Harvey RF, Hinton RA, Gunary RM, et al. Individual and
provided unequivocal evidence that psychological treatment
group hypnotherapy in treatment of refractory irritable bowel
is efficacious in irritable bowel syndrome” (3).
syndrome. Lancet 1989;1(8635):424 –5.
16. Rumsey N. Group stress management programmes vs phar-
REFERENCES: SECTION 2.12
macological treatment in the treatment of irritable bowel syn-drome. In: Heaton KW, Creed F, Goeting NLM, eds. Towards
1. Whitehead W, Palsson O, Jones KR. Systematic review of the
confident management of irritable bowel syndrome: Current
comorbidity of irritable bowel syndrome with other disorders:
approaches. London: Duphar Medical Relations, 1991:33–5.
What are the causes and implications? Gastroenterology 2002;
17. Galovski T, Blanchard E. The treatment of irritable bowel
syndrome with hypnotherapy. Appl Psychopathophysiol
2. Walker EA, Katon WJ, Jemelka R, et al. Comorbidity of
gastrointestinal complaints, depression and anxiety in the Ep-
18. Heymann-Monnikes I, Arnold R, Florin I, et al. The combi-
idemiologic Catchment Area (ECA) Study. Am J Med 1992;
nation of medical treatment plus multicomponent behavioral
therapy is superior to medical treatment alone in the therapy of
3. Talley N, Owen B, Boyce P, et al. Psychological treatments
irritable bowel syndrome. Am J Gastroenterol 2000;95:981–
for irritable bowel syndrome: A critique of controlled treat-
ment trials. Am J Gastroenerol 1996;91:277– 86.
19. Payne A, Blanchard E. A controlled comparison of cognitive
4. Bennett P, Wilkinson SA. Comparison of psychological and
therapy and self-help support groups in the treatment of irri-
medical treatment of the irritable bowel syndrome. Br J Clin
table bowel syndrome. J Consult Clinical Psychology 1995;
5. Blanchard EB, Greene B, Scharff L, et al. Relaxation training
20. Blanchard E, Schwarz SP, Neff D. Two-year follow-up of
as a treatment for irritable bowel syndrome. Biofeedback Self
behavioral treatment of irritable bowel syndrome. Behav Ther
Doxycycline Fact Sheet What is doxycycline? Doxycycline is an antibiotic medicine belonging to the Doxycycline and other members of the tetracycline class called "tetracyclines." It is used to treat bacterial class of antibiotics are not generally approved for infections in many different parts of the body. It does not treating patients under 8 years old. These antibio
microbiology specialists inc. Curriculum Vitae Alice Schauer Weissfeld, PhD, D (ABMM) Position President and CEO Microbiology Specialists Incorporated Houston, Texas Mailing Address Microbiology Specialists Incorporated 8911 Interchange Drive Houston, Texas 77054-2507 713-663-6888 Birthplace Birth Date Education B.A., Biology, Boston University, 1970 M.S., Micro
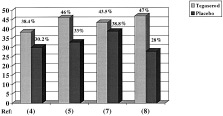 Management of IBS
Management of IBS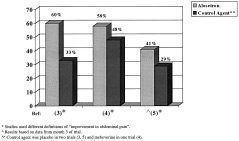 Management of IBS
Management of IBS