Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Tosinfo.com
RADIOLOGY ROUNDS RADIOLOGY ROUNDS MARTIN QUAN, MD Department Editor A man with worsening sacroiliac pain 3 months after a fall James D. Collins, MD
A 72-year-old man came to the outpatient clinic
with complaints of severe left sacroiliac pain. He hadfallen about 3 months earlier, and the pain he incurredthen had worsened over the past 2 weeks. He had a10-year history of myasthenia gravis for which he hadbeen treated with pyridostigmine bromide (Mestinon)that provided symptomatic relief.
Findings of the physical examination were general-
ly within normal limits. He reported pain over his leftfirst rib and left sacroiliac region. He had no abdomi-nal masses, and digital rectal examination showed thathis prostate was of normal size.
In the first stage of the workup, radiographs were
done of the chest, pelvis, and left first rib. Because oflytic defects in the sacrum and left posterior first rib, abone scan and percutaneous biopsies under fluoro-scopic control were ordered. Scheduled laboratorystudies included a urinalysis, acid phosphatase and
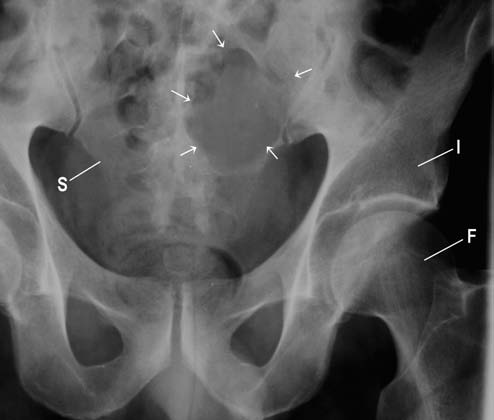
Figure 1 This anterior posterior radiograph of the pelvis displays
prostate-specific antigen (PSA) levels, and, if indicated,
lytic destruction (arrows) of the left sacrum (S). F = femur; I = ilium. The radiographic findings
An anteroposterior (AP) radiograph of the pelvis
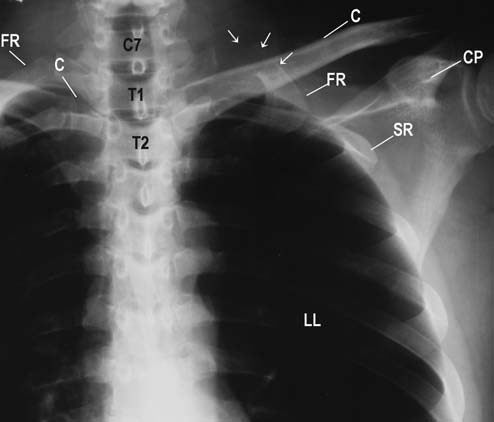
displayed a large lytic defect in the left sacrum (Figure1). A coned-down posteroanterior (PA) chest radio-graph of the left shoulder revealed near complete lyticdestruction of the proximal left first rib (Figure 2). Abone scan (Figure 3) demonstrated increased isotopeuptake in the region of left posterior first rib and mini-mal but increased activity in the area of the left sacrumand at approximately the level of T12. Such scans areoften used to indicate the safest site for percutaneousbiopsy.1 A prone pelvic radiograph, with the Craigbiopsy needle in place, displayed a compression frac-ture at L4 (Figure 4). The left pedicle of L4 is destroyed,with an associated loss of height of the vertebral body. Figure 2 This coned-down anteroposterior chest radiograph dis-
Dr. Collins is professor, department of radiology, David Geffen School of
plays lytic destruction (arrows) of the left first rib (FR). C = clavicle;
Medicine at UCLA. Dr. Quan is professor of family medicine, departmentof family medicine, David Geffen School of Medicine at UCLA. He is also
CP = coracoid process; C7 = 7th cervical vertebra; LL = left lung; SR
editor in chief of Family Practice Recertification.
= second rib; T1 and T2 = 1st and 2nd thoracic vertebrae. 14 • FAMILY PRACTICE RECERTIFICATION RADIOLOGY ROUNDS Figure 4 This prone posteroanterior radiograph documents Figure 3 In this technetium 99m methylene diphosphonate (99m Tc MDP)
the fixed position of a Craig biopsy needle (N) over the lat-
whole-body bone scan, the upper level displays anterior images; the lower level,
eral margin of the lytic lesion (large arrows) in the left
posterior images. Observe landmark anatomy of the bladder (B) in the upper
sacrum, and lytic destruction of the left pedicle (small ar-
level and increased uptake over the region of the left first rib (FR) and 12th tho-
rows) of the compressed 4th lumbar vertebra (L4). F =
racic vertebra (T12), and tumor destruction (T) of the left sacrum (S) in the lower.
femur; I = ilium; L3 and L5 = 3rd and 5th lumbar vertebrae.
The differential diagnosis included metastatic carci-
noma to bone, with prostate carcinoma as the most
• Prostate Unlike breast metastases, nearly all from
probable primary site, or metastasis from primary
renal cell carcinoma. The histologic picture was most
• Lung Second to prostate as the source of metastases
consistent with metastatic adenocarcinoma from pri-
in men, these lesions are almost always osteolytic.
mary prostatic carcinoma, which was the opinion of
• Kidney Metastases of renal cell carcinoma are typi-
the consulting pathologists and is rapidly fatal. PSA
cally osteolytic and may cause marked expansion of
the affected area. They are usually responsible for soli-tary (and no more than six) bone metastases. Discussion
Most bony metastases found during routine exam-
Take-home message
inations originate in the breast or prostate. Metastases
This patient’s disease was not suspected, and he did
in bone from the kidney are also common, but these
not have a prostatic disease workup, which is usually
primary tumors are relatively rare. The lungs are the
done soon after the diagnosis of prostate cancer to de-
source of the third most common primary tumors
termine the risk of metastases or to stage metastatic
metastasizing to bone. Other cancers likely to metas-
prostate disease. His pain required a baseline plain
tasize to bone are thyroid and kidney. Metastatic tu-
film that detected lytic lesions. The technitium bone
mors are more common than primary tumors in bone.
scan was selected because it is the most reliable and
The appearance of metastases is variable. They may
least expensive choice to detect lesions not displayed
be osteoblastic, osteolytic, or a combination of the two.
The great majority of metastases are osteolytic; thosefrom the prostate and bladder are usually osteoblastic. REFERENCES
A summary of common metastatic characteristics2:
1. Collins JD, Bassetet L, Main GD, et al. Percutaneous biopsy
following positive bone scans. Radiology 1979;132:439-442.
• Breast Nearly all are osteolytic, with lesions almost
2. Meschan I. Radiolucent bone diseases of multiple extremeties
invariably multiple and several centimeters in diame-
or regions. In: Synopsis of Analysis of Roentgen Signs in Gen-
ter. About 10% of breast carcinoma metastases are os-
eral Radiology. Phildelphia, Pa: WB Saunders; 1976:79.
VOL. 29, NO. 6, JUNE 2007 • 15
Collagen Induction Therapy ~ Consent FormYou must be 18 years of age to be treated with Collagen Induction Therapy (CIT) , or have a parent or legal guardian sign the form with you, giving consent for the treatment. Please initial that you have read each of the below statements:_____ You have the right to be informed about this treatment and decide whether or not to proceed. _____ Photos may
ICHD-II 7. Cefalea attribuita a disturbi della cefalea di tipo tensivo o della cefalea a grappolo. intracranici non vascolari Quando una cefalea primaria preesistente peggiora instretta relazione temporale con un disturbo intracrani-7.1 Cefalea attribuita a ipertensione liquoraleco, ci sono due possibilità diagnostiche, a seconda del7.1.1 Cefalea attribuita a ipertensione intracran
 RADIOLOGY ROUNDS
RADIOLOGY ROUNDS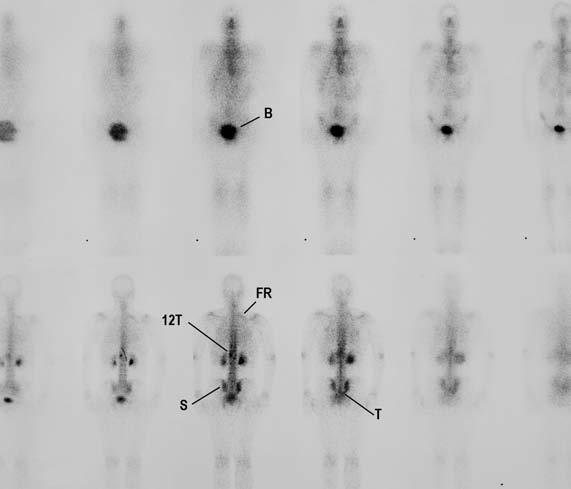
 RADIOLOGY ROUNDS
RADIOLOGY ROUNDS