Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Microsoft word - 2005 syllabus.doc
“Pediatric Pearls for Mission Trips” Roger D. Smalligan, MD, MPH Objectives 1) To discuss general cross-cultural issues related to short-term mission 2) To discuss common GI syndromes and basic treatment guidelines. 3) To review common respiratory syndromes and their treatment. 4) To present other common pediatric medical conditions encountered on mission trips. 5) To review vaccine preventable diseases that may be seen on mission Lecture Outline
I. Cultural
A. Find out about local customs regarding dress, greetings, examination of female
B. Ask about cultural beliefs and taboos. C. Go open to learning from local physicians as well as sharing how we do things in the
D. Try to find out about any unusual diseases or syndromes unique to the part of the
E. While most medications are good well beyond their expiration date, beware of taking
F. Do take along a Harriett Lane Handbook or a Palm Pilot with Epocrates or other drug
reference program with pediatric dosing information as well as The Sanford Guide to Antimicrobial Therapy (www.sanfordguide.com).
A. WHO reports 18% of childhood deaths less than 5 years of age are due to diarrhea
(2000-2003) (Lancet, 2005; 365:1147-52)
B. Remember that most diarrheal disease is self limited and does not require antibiotics
or antimotility drugs - focus on hydration status for care decisions:
Assessment of Dehydration (with estimates of fluid deficit) Variable Mild (3-5%) Moderate (6-9%) Severe ( ≥10%)
Very thirsty or too lethargic to indicate
From: “Practice Parameter: The Management of Acute Gastroenteritis in Young Children,” Pediatrics 97(3), 424, 1996.
C. Treatment of diarrhea / vomiting based on hydration status:
b) Frequent sips of oral rehydration solution (ORS) (see Figure 1) or
c) Can use medicine cup, spoon, or dropper to put in mouth every few
e) Give as much as the child will take. f) After each stool, children under 2 years of age should drink about ¼
to ½ cup of ORS and children ages 2 to 10 should drink ½ -1 cup of ORS.
a) Rehydrate using ORS / Pedialyte b) CONTINUE
c) Give as much as the child will take. d) Goal is to replace deficit plus cover ongoing losses due to diarrhea,
vomiting, sweating, insensible losses and metabolism (see approximate amounts immediately above).
e) Only contraindications are intractable vomiting / ileus / obtundation.
a) This is an emergency and will need IV placement.
(1) Can use intraosseous line in the tibia if unable to get an IV
(2) Give a 20cc/kg bolus of normal saline or Ringer’s lactate,
repeat if still has severe signs of dehydration, then calculate fluid deficit and replace over 24h.
1. If diarrhea is abundant, (yellow or whitish / watery stool) can use bismuth
subsalicylate (PeptoBismol) in liquid or tablet forms (100mg/kg/d divided into 5 doses daily for up to 5 days – tablets contain 262mg each and liquid 525mg/15cc).
2. Study in Chilean children with E. coli and rotavirus showed quicker recovery
and shorter hospital stays (Pediatrics 1991 Jan;87(1):18-27).
3. Similar results in Bangladeshi study (Acta Paediatr. 2001 Jun;90(6):601-4.) 4. Original study in Colombian children.
1. If febrile with blood or mucous in stool, can consider antibiotic therapy for
Shigella, Salmonella, toxigenic E. coli, or Campylobacter
a) Best if you have some information on resistance patterns in the area
- eg. in rural Ecuador we found high resistance rates to trimethoprim /sulfamthoxazole and amoxicillin, but high sensitivity to amoxacillin/ clavulanic acid, azithromycin, and gentamicin (5mg/kg IM qd).
1. Generally these are to be avoided as they can lead to severe paralytic ileus
A. These are common, but more associated with chronic abdominal complaints, poor
weight gain, and persistent diarrhea than acute diarrheal syndromes.
1. Extremely common in developing countries 2. Mostly asymptomatic, but if has symptoms (chronic diarrhea, abdominal pain,
wt loss) can treat with metronidazole 35-50mg/kg/day divided in 3 doses for 10 days OR tinidazole 50mg/kg in single daily dose for 3 days, OR secnidazole in a single dose (not available in USA, check on local preparations / dosing)
1. Also common in poor sanitary conditions 2. 60% asymptomatic, others may have bloating, diarrhea, abdominal pain, foul
3. Treat with metronidazole 35-50mg/kg/day divided in 3 doses for 5 days OR
tinidazole 50mg/kg in single daily dose once, OR secnidazole in a single dose (not available in USA, check on local preparations / dosing)
1. This is a worldwide, endemic problem in developing countries. 2. Patients may report having seen round worms in their stool. 3. Fecal – oral route of transmission is most common. 4. Treat with mebendazole 500mg X 1 (or 100mg bid X 3 days) or albendazole
400mg X 1 (200mg X1 in < 2yo), or Pyrantel pamoate 11mg/kg X 1.
1. Common cause of severe iron deficiency anemia. 2. A. brazilensis can cause cutaneous larva migrans; often otherwise
3. Treat with mebendazole / albendazole as for Ascaris followed by iron
1. Mostly asymptomatic or mild cutaneous or intestinal symptoms. 2. Can cause recurrent urticaria or larva currens. 3. Can see nausea, diarrhea, GI bleeding, weight loss. 4. Eosinophilia is common. 5. Find larvae in stool. 6. Treat with ivermectin 200mcg/kg qd X 2-3d, or albendazole 400mg qd X 3d
repeat in 2wks, or thiabendazole 25mg/kg bid X 2d (side effects nausea/vomiting/diarrhea/neuropsychiatric).
1. Anal itching is principal symptom, though can cause abdominal pain and
bloating if load is great - otherwise often asymptomatic.
2. Treat with mebendazole 100mg X 1 (may repeat a week later) or
albendazole 400mg X1 (200mg if under 2yo) and can repeat in a week.
1. Asymptomatic unless heavy infestation which can cause diarrhea and colitis;
2. Treat as for Ascaris – mebendazole slightly more effective than albendazole.
Taenia & Hymenolepis species (tapeworms)
1. Segmented worms – several meters long 2. Beef or pork sources 3. Adult form resides in GI tract, but larvae can invade and be found in many
4. Usually causes perianal discomfort and patients notice in stools. 5. Severe cases may include abdominal pain, nausea, weight loss, and
6. T. solium (pork tapeworm) causes neuro cysticercosis including seizures and
7. Treat GI disease with Praziquantel 10mg/kg po X 1, treat neurocysticercosis
with praziquantel 15d, or albendazole for 28d
a) Watch for inflammatory response as parasites die (may need
1. Symptoms depend on phase of migration:
(1) Diarrhea, abdominal pain, constipation and vomiting
Fever and eosinophilia, periorbital edema, splinter hemorrhages, occasionally headache and pulmonary symptoms
Myalgias, muscle edema, weakness – especially extraocular, biceps, neck, jaw, low back
2. Treat with mebendazole, albendazole or thiabendazole (effective against
enteric stage but not cysts), steroids help with myositis.
3. PREVENTION: Cooking pork until not pink or freezing at -15 C for 3 weeks
IV. Common respiratory syndromes seen in developing countries
A. WHO reports 19% of childhood deaths less than 5 years of age are due to
pneumonia / respiratory disease (2000-2003) (The Lancet, 2005; 365:1147-52)
1. If clear lungs and no respiratory distress, treat symptomatically as you would
here (always good to have vitamins and/or worm medicine so patient can go home with something).
2. Cough syrups likely not that helpful, but can try in 8 months and up.
1. If acute and no respiratory distress or high fevers, treat as URI above
1. Cough with purulent sputum (most children swallow their sputum but may
2. If prolonged (> 2 weeks duration), can treat with amoxicillin,
trimethoprim/sulfamethoxazole (in older than 2 months), cephalosporin or macrolide.
3. Otherwise symptomatic care as for URI.
1. Remember pertussis with paroxysms of cough and episodes of cyanosis
a) Treat with erythromycin or trimethoprim/sulfamethoxazole to prevent
b) Unlikely to change course of disease c) Can use trial of prednisone in severe cases d) Some children need hospitalization with oxygen
2. Think about TB in chronic cases with fevers, cough, weight loss
a) Ask about family members with chronic cough b) Can treat based on x-ray plus close family members' results of TB
(1) Best to refer to the country’s TB control program if it is
c) PPD not usually helpful as most countries use BCG vaccination in
very young and booster at 6 years of age
d) If endemic to area, think about paragonamiasis
(1) Lung fluke from eating raw crayfish or crabs from fresh water
(2) Treated with praziquantel 25mg/kg per dose tid for 2 days.
1. With lower respiratory tract symptoms & signs - higher fevers, signs of
respiratory distress (tachypnea, grunting, flaring, retractions), and/or rales on exam - think Strep and Staph (especially in tropical climates)
2. Mycoplasma and H. influenza (still common if country not vaccinating well or
3. If clinically stable and inpatient treatment not available, you can treat with a
2nd or 3rd generation cephalosporin or macrolide, amoxacillin/clavulanic acid (Augmentin), or amoxicillin, or trimethoprim/sulfa (in older than 2 months).
a) WHO guidelines state tachypnea is >60/min for 0-2 months, >50/min
for 3-12months and >40/min for 12-24months.
5. In neonates, think Group B strep, gram negatives, Chlamydia, and Listeria
6. In children under 5 years, think Strep pneumonia, H. flu (if not vaccinating),
7. In older children, think Strep pneumonia and Mycoplasma predominantly. 8. Viral pneumonia is most common in all age groups, in general, but
(1) Cool mist (2) Can try bronchodilators (inhaled albuterol / salbutamol) (3) Antibiotics not necessary
a) Think bronchospasm due to current infection vs. asthma (especially
b) GIVE 2mg/kg daily of prednisone for 5-7 days plus albuterol /
salbutamol – syrup in young children, metered dose inhaler with a spacer in 5 years old and up if available and child can cooperate
3. Asthma is common in developing countries due to smoke exposure and
4. Also remember Loffler’s syndrome (pulmonary phase of several parasites
(ascaris, ancylostoma, others) causing fluffy infiltrates, cough and wheezing).
1. Gradual onset, low grade fevers, handling secretions
(1) Can be treated with cool mist and acetaminophen
2. Abrupt onset, high fevers, difficulty with secretions, toxic appearing child
(1) Most commonly caused by H. flu (2) Needs emergency attention including IV antibiotics and
possible intubation under controlled conditions ideally.
V. Other common pediatric conditions seen on mission trips
1. Especially if traveling to Africa / Asia – less prevalent in South America –
check with local missionaries and experts regarding current identification and treatment of pediatric AIDS patients; part of prevention of vertical transmission includes zidovudine during pregnancy, intrapartum and postpartum for 6 weeks beginning 8h after birth (Connor, EM, Sperling, RS, Gelber, R, et al. Reduction of maternal-infant transmission of human immunodeficiency virus type 1 with zidovudine treatment. N Engl J Med 1994; 331:1173).
B. Parasites – (see under GI above for amebas, ascaris, ancylostoma, giardia, etc.)
a) WHO reports 8% of <5yo deaths 2000-2003 due to malaria but 18%
in Africa, The Lancet, 2005; 365:1147-52
b) Research the type of malaria you will encounter – clinically presents
with high spiking fevers, headache, anemia, and hepatosplenomegaly - if chloroquine sensitive area (P. vivax and P. ovale) can treat even small children with chloroquine (10mg base/kg PO X 1 followed by 5mg/kg PO at 12, 24 and 36h) and primaquine (0.6mg/kg/d qd 14d); otherwise treat as resistant P. falciparum with regimen recommended / available by local physicians / missionaries (quinine sulfate + doxycycline OR mefloquine OR sulfadoxine/pyrimethamine(Fansidar) OR atovaquone/proguanil (Malarone) OR halofantrine (Halfan).
a) Cutaneous and mucocutaneous – presents after sandfly bites in
endemic areas with chronic nonhealing skin ulcers that can become superinfected. Treatment is with fluconazole daily for 6 weeks or heavy metal antimonials, requires IM injections daily for 21-28 days (stibogluconate (Pentostam) or meglumine antimonite (Glucantime). Kala-azar is systemic involvement (in India / Africa) and is treated with miltefosine (not available in USA) or amphotericin B.
C. Malnutrition – marasmus - (caloric deficiency)- diminished weight and height for
age, emaciated, weak, thin, dry skin & sparse hair; kwashiorkor – (protein deficiency) – nearly normal weight and height for age, anasarca, pitting edema in the lower extremities, dry, pale hair, hepatomegaly and abdominal distension; - important to find out what food sources are available locally and brainstorm with local public health / relief workers about correcting the deficiencies.
1. Candidal diaper rash is especially common in tropical areas – nystatin cream
2. Staphylococcal pyodermatitis – can mimic candidal rash except presents with
more pustules and desquamation – if mild can treat with antibacterial soap
washes frequently, more extensive will require po antibiotics (cephalexin or erythromycin)
3. Cellulitis – very common and can be aggressive in tropical countries, caused
by staph and strep, if very localized can use mupirocin (Bactroban) ointment bid but anything more should be treated with po antibiotics (1st or 2nd generation cephalosporins or erythromycin, IV if extensive or progressing).
4. Impetigo – mupirocin or po 1st generation cephalosporin or erythromycin. 5. Scabies is ubiquitous – look for papules, burrows, and severe pruritis and
treat with whatever is available locally – permethrin, crotamiton, lindane 1% cream or lotion – all are applied neck down and washed off in 6-8 hours.
6. Tinea capitis – griseofulvin po for 6 weeks. 7. Tinea pedis / corporis – use clotrimazole cream bid – tid or other locally
8. Botfly myiasis – nonhealing papular lesion with central hole that drains
serosanguinous fluid - extract the maggot and will heal without antibiotics usually or cover for Staph with po antibiotics.
9. Viral exanthems / roseola / drug reactions – as in USA.
E. Anemia – iron deficiency is common everywhere but more severe and complicated if
poor general nutrition and parasites are involved, especially malaria and ancylostoma. Treat the underlying disease and give iron supplements as you would for iron deficiency in USA.
F. Miracle cure seeking – some people will travel far to see the foreign doctors, bringing
children with severe mental retardation and cerebral palsy or post-encephalitis syndromes, etc. hoping for the miracle cure – compassionate explanation and prayer is often appreciated. Don’t be afraid to pray in faith for the miraculous when you are at the end of your medically available means (or before!) – miracles do happen.
VI. Vaccine preventable diseases you may see on the mission field
A. H. influenzae related diseases – many developing countries cannot afford and do not
provide this vaccine (HIB) – hence you may see H. flu meningitis cases and preseptal / periorbital cellulites due to this organism. Treat with ceftriaxone, cefotaxime, or ampicillin + chloramphenicol.
B. Pertussis - see under persisitent cough (3D) above. C. Measles – worldwide estimates are 30-40 million cases per year and many countries
still only vaccinate once against measles rather than the 2 dose regimen in the USA. (World Health Organization. WHO-UNICEF joint statement on strategies to reduce measles wordwide. Wkly Epidemiology Record 77(27): 224-228, 2002.) This will be a clinical diagnosis in a developing country including: fever greater than 101.0° F (38.3° C) and viral prodrome of cough, coryza, and conjunctivitis, then 2-3 days later a generalized, nonpruritic maculopapular rash spreading from head to trunk including palms and soles (also remember Koplik’s spots – whitish spots on buccal mucosa with erythematous hue may be seen just prior to the rash). Vitamin A 100,000 – 200,000 units po given to children with measles has been shown to reduce morbidity and mortality in developing countries. (2003 Red Book: Report of the Committee on Infectious Diseases, 26th ed, p. 419).
D. Mumps – many countries use only the measles vaccine and mumps is not covered at
all – remember salivary gland swelling, most often parotid glands, usually self limited and benign, though can see aseptic meningitis, encephalitis, orchitis (in post-pubertal boys), pancreatitis. Treatment is symptomatic and supportive.
E. Neonatal tetanus – as many children are born at home with the help of family
members or traditional birth attendants, clean conditions are often not possible and
contamination of the umbilical stump can occur. Mothers in remote areas often have not been vaccinated against tetanus. Clinically may see severe muscle spasms and opisthotonus. Incubation period is 2 days to months. Treat with tetanus immune globulin if available (often expensive or unavailable) plus IV PCN G or metronidazole.
F. Congenital rubella – in countries where MMR is not used, may see this – growth
retarded infants, hepatosplenomegaly, purpuric skin lesions (“blueberry muffin” appearance), ophthalmologic, cardiac and neuro defects. Defects occur in 50% if during 1st month of gestation, 20-30% if 2nd month and 5% if after 3rd month of gestation.
References
• Bryce J, Boschi-Pinto C, Shibuya K, Black RE. WHO estimates of the causes of death in
children. Lancet, 2005; 365:1147-52.
• No authors listed. Practice parameter: The management of acute gastroenteritis in
young children. Pediatrics 1996; 97:424-435.
• Soriano-Brucher H, Avedano P, O’Ryan M, Braun SD, Manhart MD, et al. Bismuth
subsalicylate in the treatment of acute diarrhea in children: a clinical study. Pediatrics 1991; 87(1):18-27.
• Guarino A, Bruzzese E. Which place for bismuth subsalicylate in the treatment of enteric
infections? Acta Paediatr 2001; 90(6):601-604.
• Chowdhury HR, Yunus M, Zaman K, Rahman A, Faruque SM, et al. The efficacy of
bismuth subsalicylate in the treatment of acute diarrhoea and the prevention of persistent diarrhoea. Acta Paediatr 2001; 90(6):605-610.
• No authors listed. WHO-UNICEF joint statement on strategies to reduce measles
mortality worldwide. Wkly Epidemiology Record 2002; 77(27)): 224-228.
• 2003 Red Book: Report of the Committee on Infectious Diseases, 26th ed, p. 419.
• Connor, EM, Sperling, RS, Gelber, R, et al. Reduction of maternal-infant transmission of
human immunodeficiency virus type 1 with zidovudine treatment. N Engl J Med 1994; 331:1173-1180.
Figure 1 Homemade Oral Rehydration Solution. (From Werner, D. Where There is No Doctor: A Village Health Care Handbook. Hesperian Foundation, Palo Alto, CA, 1992.)
VwGH 2005/11/03, 2002/15/0124 Der Verwaltungsgerichtshof hat durch den Vorsitzenden Vizepräsident Dr. W. Pesendorfer und die Hofräte Dr. Sulyok, Dr. Fuchs, Dr. Zorn und Dr. Mairinger als Richter, im Beisein des Schriftführers MMag. Twardosz, LL.M., über die Beschwerde des Präsidenten der Finanzlandesdirektion für Wien, Niederösterreich und Burgenland gegen den Bescheid der Finanzla
RAMAH DAY CAMP in NYACK CAMPER Winter Address Summer Address PHOTO New York, NY 10027 PART I. (A parent or legal guardian should complete this page of the form) ______________________________________________________________________________________________ Camper Last Name ______________________________________________________________________________________________ Add
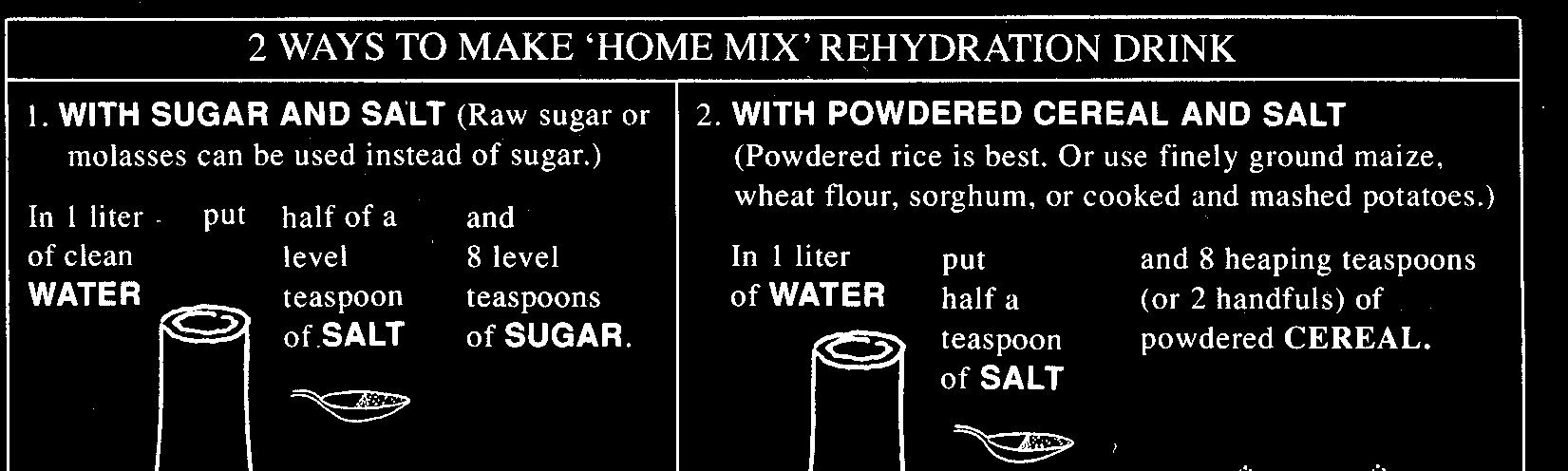
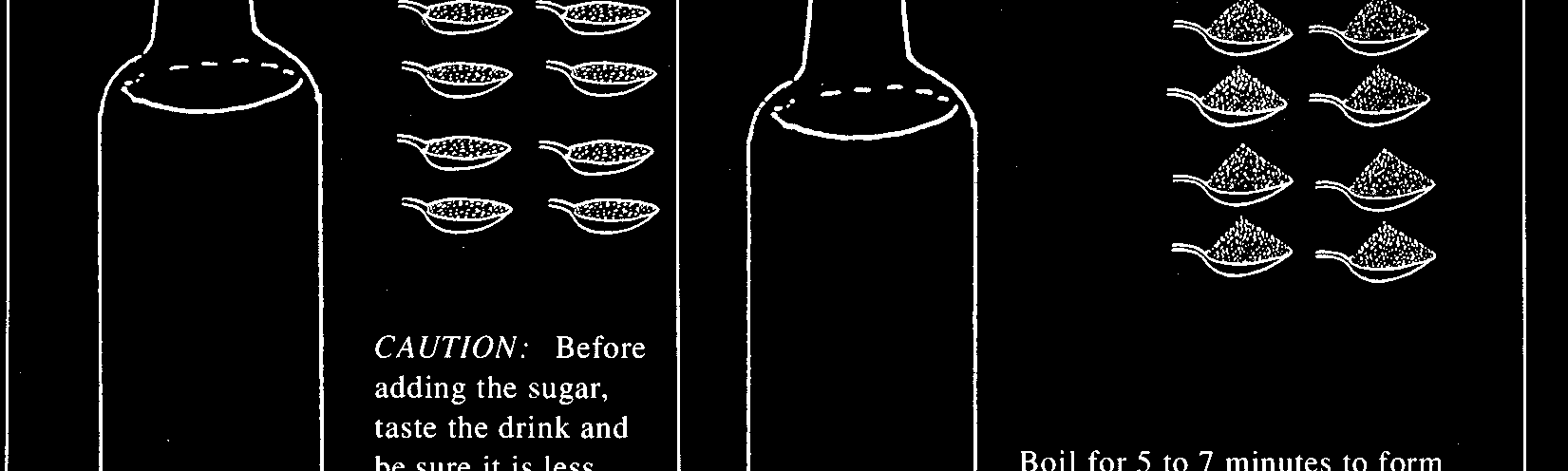
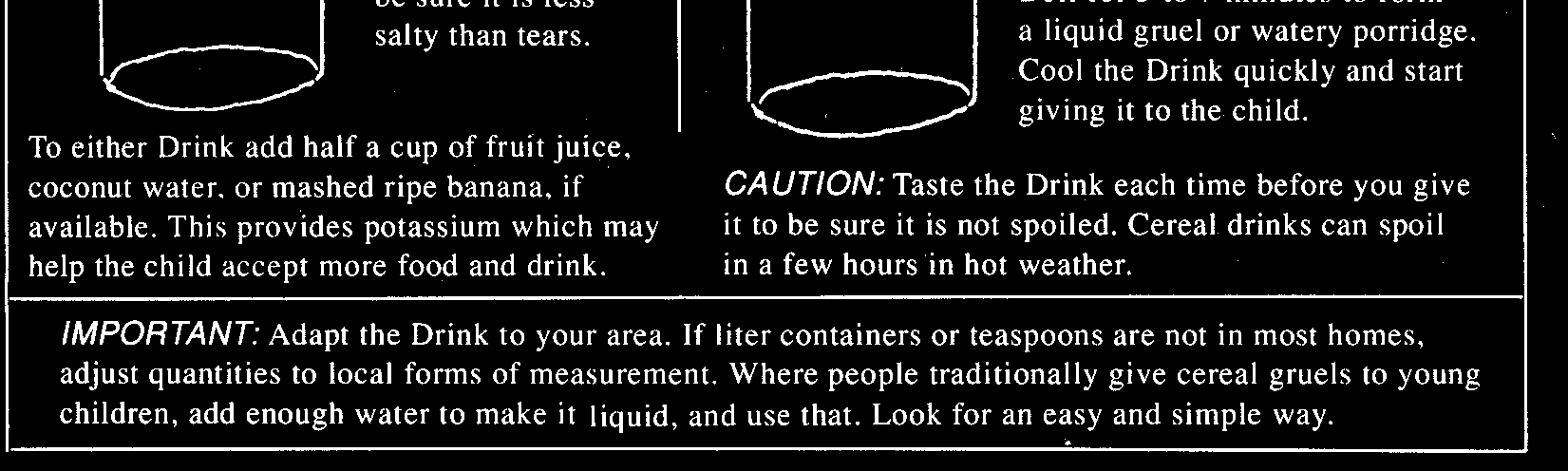 Figure 1 Homemade Oral Rehydration Solution. (From Werner, D. Where There is No Doctor: A Village Health Care Handbook. Hesperian Foundation, Palo Alto, CA, 1992.)
Figure 1 Homemade Oral Rehydration Solution. (From Werner, D. Where There is No Doctor: A Village Health Care Handbook. Hesperian Foundation, Palo Alto, CA, 1992.)