Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Pii: s0168-8510(01)00162-2
Rationalising rationing: economic and other
considerations in the debate about funding of
Elly A. Stolk *, Werner B.F. Brouwer, Jan J.V. Busschbach
Institute for Medical Technology Assessment, Erasmus Uni6ersity Rotterdam, PO Box 1738,
3000 DR Rotterdam, The Netherlands
Received 30 May 2000; accepted 10 May 2001
Abstract
Although the cost-effectiveness of Viagra for the treatment of patients with erectile
dysfunction is favourable, both public and political opinions seem to be inclined not to fund,or merely to partially fund (i.e. by reimbursing only specific patient groups) this medicine. This shows that in funding discussions, cost-effectiveness information is not solely decisive. In a theoretical framework for choices in health care that was developed in The Netherlands(the Dunning report, 1991), two other criteria besides cost-effectiveness were put forward asbeing important for rationing decisions: ‘necessary care’ and ‘individual responsibility’. Overlooking the Viagra discussion, many of the arguments put forward seemed to be relatedto these two criteria. However, a clear operationalisation of the criteria necessary care andindividual responsibility is lacking, which makes it difficult to use the arguments in fundingdecisions. In this paper, we try to demonstrate how these criteria were presented in theViagra discussion and we will indicate how these criteria can be operationalised in relationto the outcomes of a cost-effectiveness analysis. 2002 Elsevier Science Ireland Ltd. Allrights reserved. Keywords: Viagra; Funding discussion; Necessity; Private responsibility; Policy making; Economics;Ethics
* Corresponding author. Tel.: + 31-10-408-8654; fax: + 31-10-408-9094. E-mail address: (E.A. Stolk).
0168-8510/02/$ - see front matter 2002 Elsevier Science Ireland Ltd. All rights reserved.
PII: S 0 1 6 8 - 8 5 1 0 ( 0 1 ) 0 0 1 6 2 - 2
E.A. Stolk et al. / Health Policy 59 (2002) 53 – 63
1. Viagra: an exceptional case in debates on rationing
In September 1998, Viagra was introduced on the European market, where it was
an immediate success: the sales figures in the first months after introduction wereextraordinarily high, especially given the fact that Viagra was a new, non-fundedmedicine. The question then became whether or not governments should fundViagra in a public health care system. After all, the budgetary impact of funding ofViagra could be substantial, given this high demand.
In such funding decisions, economic evaluation plays an important role in
indicating the relative efficiency of the health intervention under consideration. Recently, several studies demonstrated that erectile dysfunction limits quality of lifeconsiderably. Hence, the use of an indisputably effective medicine such as Viagraresults in a substantial gain in quality of life [1,2]. These gains are reached at fairlylow costs, therefore, the cost-effectiveness of Viagra is very favourable (Table 1)[3 – 5].
Table 1 demonstrates that on basis of arguments of cost-effectiveness alone,
Viagra is eligible for funding. However, cost-effectiveness information is not theonly grounds for basing this decision. Compare this case with another from thetable — heart transplants, for example. Heart transplants have much higher cost perQALY, yet their reimbursement is not a matter of debate. In contrast, funding ofViagra is fiercely disputed, indicating that other factors must also play a role in theallocation of health care resources. Previous experiences with reimbursement deci-sions already indicated the role of additional arguments, for instance in the case of
Table 1Outcomes of Dutch studies in terms of incremental cost per QALY
Surgical correction of congenital anorectal malformation
The costs are valued for the year 1995. This table is adapted from Rutten [6].
a Although the treatments differ substantially in type of health gain and size of the treatment costs, in
terms of cost per QALY they can be compared. For instance, Viagra does not save life years, butincreases quality of life (0.11% for each year that treatment is continued). In contrast, a liver transplantsaves life years (5 years survival is 59%). Obviously, the health gain of Viagra is smaller, but as the costsare also much lower (about $560 per year, compared to initial treatment costs of over $100 000 for aliver transplant) its cost-effectiveness ratio is more favourable [5,27]. Please note that differences inmethodology (e.g. derivation of QALY scores) may exist between studies. E.A. Stolk et al. / Health Policy 59 (2002) 53 – 63
lung-transplants, where unfavourable cost-effectiveness information was notenough reason not to fund them. Viagra, however, is an exceptional case in thatdespite a favourable cost-effectiveness ratio, its funding remains in dispute.
The public debate about the desirability of funding for Viagra provides us with
the rare opportunity to study those arguments favouring denial of reimbursementfor a cost-effective medicine. This paper will therefore focus on the additionalcriteria, besides cost-effectiveness, that play a role in funding decisions. The papermainly demonstrates that economic evaluation as it stands now, cannot explainwhy funding is denied or granted in different situations. However, if economicevaluations were broadened to include several societal preferences that are dis-cussed in the paper, it would be a more useful tool in and better predictor offunding decisions. The paper therefore is an effort to contribute to a broadermedical technology assessment framework, which incorporates elements other thanmerely costs and unweighed effects, bridging the gap between current cost-effective-ness analysis and the decision-making process. We will indicate how these criteriamay be further operationalised and related to the outcomes of economic evalua-tions in health care. 2. Main arguments against funding Viagra
In the Viagra discussion, two main arguments are put forward, both in the
political and in the public discussion, that object to funding the new drug [7 – 9]. First, erectile dysfunction is often accepted as normal part of ageing. Consequen-tially, treatment can be viewed as an unnecessary luxury, which should not interferewith providing necessary medical interventions (e.g. lifesaving interventions). Sec-ond, it is argued that funding of treatment of erectile dysfunction may be denied onthe basis of an ‘private choice, private responsibility’ argument. Having sex inadvanced stages of life is perceived to be a personal choice, related more to lifestylethan to health problems. Viagra is thus considered to be a lifestyle drug, not eligiblefor public funding. In Germany, similarly, it was argued that when only someelderly individuals choose to have sex, while others forgo this pleasure, it isinappropriate to pay collectively for their ‘pleasure’.
Although these criteria of necessity and individual responsibility have an intuitive
appeal, they lack clear operationalisation. Definitions of for instance luxury healthcare and serious conditions were not provided in the public or political debate. Also, it was not made clear why Viagra would be an unnecessary medicine. Although erectile dysfunction is not lifethreatening, clinical need becomes obviouslyapparent when put in terms of quality of life [2,10 – 13]. But how does a quality oflife score relate to necessity of treatment? A possible answer to that question will beprovided in the subsequent sections.
The argument of individual responsibility also lacks a clear operationalisation.
How to distinguish between lifestyle purposes and legitimate medical use of Viagrais debated vigorously [14]. In The Netherlands ‘in vitro fertilisation’ has also beenlabelled as a lifestyle treatment. Nevertheless, the wish to have children is generally
E.A. Stolk et al. / Health Policy 59 (2002) 53 – 63
widespread and not related to a particularly deviant lifestyle [15]. Furthermore,those persons wishing to undergo IVF experience great distress and discomfort,leading to an obvious loss of well being or quality of life. Their only wish seems tobe to live and function normally, just like ‘everybody else’. In that sense, it seemsrather odd to claim that it is a lifestyle choice to have children. Similar commentscan be made about many drugs, which have been labelled ‘lifestyle drugs’ [14].
In short, the arguments used in the public debate to support denial of funding for
Viagra, are unsatisfactory and seem to be used only in an unconvincingly oppor-tunistic manner. The arguments lack generalisability towards other conditions andother therapies, hampering consistency and transparency in decision making. Toprogress further in developing a decision-making framework for choices in healthcare, we need to define the criteria necessary care and private responsibility in amore applicable manner, as done in the next section. 3. Operationalisation of other arguments
In spite of their poor current operationalisation, the here discussed arguments of
necessity and individual responsibility have intuitive appeal and seem to be basedon widely shared underlying moral principles.
The criterion of necessary care seems to reflect the idea that patients in a poor
state of health are more entitled to health care (if this can provide them withimprovement or relief) than those in a better health state. The example of lungtransplants may help to illustrate this. Patients eligible for a lung transplantnormally are in such poor health states (i.e. low on a QALY scale), that a high costper QALY is considered acceptable in order to provide them with a ‘last resortmedicine’. This phenomenon may be especially pronounced for lifesaving interven-tions. In contrast, erectile dysfunction is generally considered to be a minor healthproblem (i.e. occurring high on a QALY scale).
Apparently, the severity of a condition, in terms of its absolute QALY score,
determines (at least partly) the necessity of treatment. Necessity of treatment seemsto increase when the patient is lower on the QALY scale. In current economicevaluation, however, QALYs are weighed equally regardless of the absolute posi-tion of patients on the QALY scale. Thus, only the number of QALYs gaineddetermine priority, while in the decision-making process QALYs that are gainedlower on the scale may be given more weight. QALYs are apparently weighted onthe basis of necessity, leading to an acceptance of higher cost per QALY in moresevere conditions. The process of weighing QALYs will (implicitly) change theranking of the different programs in Table 1. The QALYs gained in lung trans-plants, for instance, may be considered highly necessary and therefore, be weighedthree times higher than is currently done [16], resulting in a higher priority for lungtransplants. Such weighing seems to reflect an important social preference, as has
E.A. Stolk et al. / Health Policy 59 (2002) 53 – 63
been argued elsewhere. Especially, Erik Nord has devoted much attention to thisphenomenon, trying to estimate the social weights for different QALY gains[17 – 19]. If we would use such weights in economic evaluation, perhaps, the resultswould better reflect societal preferences concerning the necessity of treatments. Inthe case of Viagra, this would mean that the QALY gains would receive a relativelylow weight in the decision-making process, since the average patient scores rela-tively high on the QALY scale (increasing the cost-effectiveness ratio indicated inTable 1). Note that in specific patient groups (e.g., patients with erectile dysfunctiondue to spinal cord injuries) such an argument does not hold and different conclu-sions about the necessity of treatment may be drawn.
3.2. Indi6idual responsibility
Even if the argument suggests that a condition at the upper end of the scale
should have a more favourable cost per QALY to be eligible for treatment thaninterventions lower on the scale, it could still be argued that Viagra should beeligible for funding, since the costs per QALY are extraordinarily low. Anotherconsideration, however, still might prohibit this funding, namely, the choice be-tween individual and collective responsibility for the costs of a treatment.
The aforementioned argument that erectile dysfunction should be accepted as a
part of normal ageing is another prevalent claim that argues against funding ofViagra. This argument seems to reflect some social reference point for health andfunctioning at certain ages or stages of life [9]. It implies that, while QALY gainshigh on the QALY scale may be considered less necessary than those low on theQALY scale, it may even be possible to determine certain thresholds, below whichQALY gains are seen as necessary and above which, unnecessary. In these terms,the choice between individual and collective responsibility could depend on thequestion of whether or not the health gain is viewed as ‘pleasure seeking’ (or ‘luxuryhealth care’), which may — like necessity — be related to the place on the QALYscale where the health gains occur.
To get a better understanding of these thresholds, the theory of Scitovsky could
be helpful. The economist Scitovsky distinguishes between two types of utility gain:pleasure seeking and ‘pain avoiding’ [20]. It may be assumed that pleasure seekingin medicine, for instance cosmetic facelifts or liposuction, are those treatments thatpeople want to undergo in order to strive above a (societal) reference point forhealth at a certain age or lifestage. The societal reference point can be seen as somepoint below perfect health. Pleasure seeking treatments could be left to privateresponsibility and our collective responsibility refers to pain avoidance, which refersto treatments that are aimed at QALY gains in persons that are below their societalreference point of health and functioning. For instance, treatments to slow downcancer or treatment of hernia to reduce pain or other discomforts are likely to beclassified as pain avoiding treatments.
The classification of Viagra as pleasure seeking explains the objection to collec-
tive funding of this medication and the urge to let patients pay for their own‘pleasures’. After all, it is likely that collective resource allocation to pain avoiding
E.A. Stolk et al. / Health Policy 59 (2002) 53 – 63
treatments is preferred over pleasure seeking treatments, e.g., because funding thelatter in a situation where not all ‘pain avoidance’ is accounted for will onlyincrease the individual differences in health status. Then, someone’s eligibility fortreatment may be defined as the difference between actual health state and asocietal reference point, which can both be quantified in terms of quality of life. Note that also for pleasure seeking interventions (such as Viagra for erectiledysfunction) the burden of disease can still be expressed in terms of QALYs. Hence,pleasure seeking or pain avoiding is not defined by absence or presence of burdenof illness; the classification of pleasure seeking is thus solely determined by thereference point.
Different reference points may be used for different patient groups and these
societal reference points may shift over time (presumably upwards), as for instancethe availability of new treatments will change the perspective on diseases (in 15 or20 years, having sex at an older age shall perhaps be perceived as normal). Also,society probably uses different reference points for health for the elderly than foryounger persons [21 – 23], e.g., poorer health states are more acceptable in olderpersons than they are in younger persons. This is easily illustrated in terms ofmobility; only being able to walk a maximum of 3 miles, slowly, may be acceptedat the age of 80 but not at the age of 20. For Viagra, this could mean that erectiledysfunction is considered normal or acceptable in older patients, for whomtreatment could therefore be classified as pleasure seeking, while it is not normaland unacceptable in younger patients (e.g. younger patients with erectile dysfunc-tion due to diabetes), for whom treatment would be classified as pain avoidance. Finally, the reference points for health may be different for different dimensions ofquality of life: experiencing pain may be considered equally unacceptable foreverybody, while a decline in mobility after a certain age can be considered moreacceptable. In Fig. 1, this framework is summarised.
The choice between individual and collective responsibility for the costs of a
treatment probably depends on three (related) elements. The first element has beendiscussed extensively above (consisting of the question whether or not the healthgain can be seen as pleasure seeking, which is determined by the place on theQALY scale: above or beyond the reference point). However, whether or not toleave the costs of medication up to the patient is probably also related to thepossibility to pay the related costs ‘out of the patient’s pocket’ as well as uponwhether or not the individual could have prevented the condition requiring themedical attention.
If the costs of an intervention are low, one may choose to shift these costs from
the collective to the private responsibility. A major problem in such a shift is thatthere always will be patients for whom even low costs are hard to pay. Shiftingcosts would then create differences in health care use between higher and lowerincome groups, which is considered unacceptable in many countries. An importantreason why such a shift could be considered acceptable regardless of the possible
E.A. Stolk et al. / Health Policy 59 (2002) 53 – 63
Fig. 1. Hypothetical decision-making framework.
differences between income groups that will be a result from the shift, is that theintervention is not considered very important (or necessary). The reason is thatby origin the health care system aims to protect people against unforeseeableevents with large consequences (either in financial terms or in terms of healtheffects). The other way around, events with only small consequences do notappeal very much to our feelings of solidarity with those at risk. Also, one maychoose not to be insured against relatively affordable (and preferably foreseeable)expenditures.
Another argument favouring individual responsibility is derived from the wish
to penalise unhealthy behaviour. The origin of the condition can be important incases where the patient is responsible for the condition. For example, societymay be more inclined to pay for Viagra for somebody with an erectile dysfunc-tion due to a spinal cord injury resulting from a traffic accident, than forsomeone with an erectile dysfunction due to excessive smoking and drinking. However, although this argument is heard frequently for many types of treat-ment (e.g. lung cancer due to smoking), it is very difficult to put into practice. Also, when the consequences of our actions are severe, it is questionable whethersuch an argument can or should be decisive. E.A. Stolk et al. / Health Policy 59 (2002) 53 – 63
4. Implications for decision making
The arguments regarding necessary care and individual responsibility, in combi-
nation with information about cost-effectiveness, seem to outline a decision-makingframework in which QALY maximisation is not the only goal. Necessity andindividual responsibility also play a role. Below we explore how these findings canchange the Dutch model for choices in health care.
The criteria necessary care and individual responsibility have been discussed
before. For example, they were put forward, together with effectiveness andcost-effectiveness, in a theoretical framework for choices in health care that wasdeveloped in The Netherlands (the Dunning report, 1991) [24]. Basically, in theDunning report, the four criteria functioned as a funnel with four sieves, developedto separate care that should receive funding from care that should not be funded. Any intervention that does not make it through all the sieves will not be includedin the basic benefit package of health care services (Fig. 2).
The Dunning report has played a key role in the Dutch discussion on rationing
health care. Nevertheless, the success of the funnel in terms of removing servicesfrom the public health plan or keeping new services out of it has been limited. This
Fig. 2. The Dunning system for priority setting. E.A. Stolk et al. / Health Policy 59 (2002) 53 – 63
may be a result of the poor operationalisation of the criteria necessary care andindividual responsibility in the Dunning report. By not relating the criteria to realand measurable outcomes or quantities, working with them becomes rather difficult. Even more so, because all the sieves should lead to a yes or no answer for funding,while decision makers probably weigh the criteria, as we have argued above.
In the operationalisation of the criteria outlined here, the criteria necessary care
and individual responsibility no longer function as sieves. Instead, decisions aremostly based on multiple criteria, together guiding the decision. Most interventionswill be necessary to some extent (or for certain patient groups) and only thosetreatments used by patients to strive beyond a societal reference point, may be seenas unnecessary or, in other words, as lifestyle interventions. All other interventionsare, in principle, eligible for funding, with necessity being related to the severity ofa condition, and higher costs per QALY being allowed in patients who are moreseriously ill. 5. Conclusions
It becomes apparent from the Viagra funding discussion, that cost-effectiveness
information alone cannot provide sufficient information to guide reimbursementdecisions. Economic considerations need to be supplemented with the criterianecessary care and individual responsibility. The way these criteria are used in theViagra debate may suggest that QALY gains are valued differently, depending onthe place on the QALY scale where they occur compared to some societal referencepoint for health. This could explain why funding of Viagra is being denied forseveral patient groups despite its favourable cost-effectiveness. In short, economicevaluation may benefit from incorporating especially the following preferencesseemingly present in society: QALY gains should be weighted for severity. QALY gains should be weighted for necessity in terms of discrepancy between
a(n age related) reference point for health and real health state.
These and other mentioned reflections are a result of analysing the debate on
funding only of one particular drug, namely Viagra and therefore, are only a firstattempt to get a firmer grip on the arguments underlying funding debates and theirrelation to cost-effectiveness analyses. It will be interesting to see whether the samecriteria will be applied in future debates on new drugs. An important feature of theViagra case, which may blur the interpretation somewhat, is that this debate maynot only reflect attitudes towards rationing in general, but may also incorporatesome also ‘Calvinistic’ attitudes towards sexuality.
Valuing QALYs gains differently on the basis of their place on the QALY scale
is not common practice in formal economic evaluations, but it may already beperformed implicitly by decision makers [25]. In this respect, it should also be notedthat in the health economics and medical literature, there is increasing attention foralternatives for simple health maximisation in which all QALY gains are treated thesame [16,26]. E.A. Stolk et al. / Health Policy 59 (2002) 53 – 63
Both the public and the political debate on rationing and the ongoing research
efforts of scientists (from various disciplines) indicate the need for a more transpar-ent way of rationing health care that is related to societal preferences for healthgains in different patient groups. Developing a publicly supported framework forchoices in health care, therefore, is an important goal, though difficult to achieve. In this paper, we have tried to indicate how (a part of) such a framework might beconstructed, and indicated some implications of such a framework for the alloca-tion of scarce resources in health care, if it would be consistently used. We hopethat this paper may further stimulate the debate on transparent and consistentrationing in health care. Acknowledgements
We would like to thank an anonymous referee for his valuable comments on an
References
[1] Volk RJ, Cantor SB, Spann SJ, Cass AR, Cardenas MP, Warren MM. Preferences of husbands and
wives for prostate cancer screening. Archives of Family Medicine 1996;6:72 – 6.
[2] Stolk EA, Busschbach JJV, Caffa M, Meuleman EJH, Rutten FFH. The cost-utility of Viagra® in
the Netherlands, IMTA-Report 99.49. Rotterdam: Institute for Medical Technology Assessment,1999.
[3] Smith KJ, Roberts MS. The cost-effectiveness of sildenafil. Annals of Internal Medicine
[4] Kwok YS, Kim C. Valuing Viagra: what is restoring potency worth? Effective Clinical Practice
[5] Stolk EA, Busschbach JJV, Caffa M, Meuleman EJH, Rutten FFH. Cost utility of sildenafil
compared to papaverine-phentolamine injections. British Medical Journal 2000;320:1165.
[6] Rutten FFH. Interpretation and use of cost-effectiveness analysis. In: Rutten-van Mo¨lken MPMH,
Busschbach JJV, Rutten FFH, editors. From cost to effects: a manual for evaluation studies inhealth care, 2000.
[7] Brooks A. Viagra is licensed in Europe but rationed in Britain. British Medical Journal
[8] Ramsey-Baggs P, Gaskell P. Rationing. British Medical Journal 1998;317:1527. [9] Letters to the editor. Rationing of sildenafil. British Medical Journal 1999;318:1620.
[10] Jønler M, Moon T, Brannan W, Stone NN, Heisey D, Bruskewitz RC. The effect of age, ethnicity
and geographical location on impotence and quality of life. British Journal of Urology1995;75:651 – 5.
[11] Litwin MS, Nied RJ, Dhanani N. Health-related quality of life in men with erectile dysfunction.
Journal of General Internal Medicine 1998;13:159 – 66.
[12] Wilke RJ, Glick HA, McCarron TJ, Erdre MH, Althof SE, Linet AO. Quality of life effects of
alprostadil therapy for erectile dysfunction. Journal of Urology 1997;157:2124 – 8.
[13] Gheorghiu S, Godschaik M, Gentili A, Mulligan T. Quality of life in patients using self-adminis-
tered intracavernous injections of prostaglandin E1 for erectile dysfunction. Journal of Urology1996;156:80 – 1.
[14] Gilbert D, Walley T, New B. Lifestyle medicines. British Medical Journal 2000;321:1341 – 4. E.A. Stolk et al. / Health Policy 59 (2002) 53 – 63
[15] De Graaf: Pil en IVF horen niet in het ziekenfonds (newspaper correspondent). In: Volkskrant
[16] Waugh N, Scott D. How should different life expectancies be valued. British Medical Journal
[17] Nord E, Richardson J, Street A, Kuhse H, Singer P. Maximising health benefits vs egalitarinism: an
Australian survey of health issues. Social Science and Medicine 1995;41(10):1429 – 37.
[18] Nord E, Street A, Richardson J, Kuhse H, Singer P. The significance of age and duration of effect
in social evaluation of health care. Health Care Analysis 1996;4:103 – 11.
[19] Nord E, Pinto JL, Richardson J, Menzel P, Ubel P. Incorporating societal concerns for fairness in
numerical valuations of health programmes. Health Economics 1999;8:25 – 39.
[20] Scitovsky T. The joyless economy. An inquiry into human satisfaction and consumer dissatisfac-
tion. New York: Oxford University Press, 1977:310.
[21] Williams A. Intergenerational equity: an exploration of the ‘fair innings’ argument. Health
[22] Tsuchiya A. QALYs and ageism: philosophical theories and age weighting. Health Economics
[23] Busschbach JJV, Hessing DJ, De Charro FT. The utility of health at different stages in life; a
quantitative approach. Social Science and Medicine 1993;37(2):153 – 8.
[24] Government Committee on Choices in Health Care. Choices in Health Care. Zoetermeer: Ministry
of Welfare, Health and Cultural Affairs, 1992.
[25] Williams A, Cookson C. Equity in health. In: Culyer AJ, Newhouse JP, editors. Handbook of
health economics. Amsterdam: Elsevier, 2000.
[26] Brouwer WBF, Van Hout BA. How should different life expectancies be valued? Diminishing
marginal utility and discounting future effects have similar consequences. British Medical Journal1998;317:1155.
[27] Michel BC, Bonsel GJ, Stouthard MEA, McDonnell J, Habbema JDF. Cost-effectiveness analysis
of long-term liver transplantation; the liver transplantation program of Groningen 1979 – 1991. NedTijdschr Geneeskd 1993;137(19):963 – 9.
Drug Profile Montelukast * Dr. Paul Samuel Montelukast is a selective and orally active Pharmacokinetics leukotriene receptor antagonist that specificallyMontelukast is rapidly and nearly completelyinhibits the cysteinyl leukotriene CystLT1 receptor. absorbed following oral administration. MonelukastIt is available as montelukast sodium. is more than 99% bound to plasma proteins.
M. Votava · M. Krsˇiak · J. Podhorná · K.A. Miczek Alprazolam withdrawal and tolerance measured in the social conflict test in mice Abstract Rationale: It is difficult to assess withdrawal locomotion while aggression tended to be increased. from benzodiazepines, and preclinical assessment of be- Conclusions: Tolerance to the alprazolam effects on ag-haviour during social conflict
 Rationalising rationing: economic and other
considerations in the debate about funding of
Elly A. Stolk *, Werner B.F. Brouwer, Jan J.V. Busschbach
Institute for Medical Technology Assessment, Erasmus Uni6ersity Rotterdam, PO Box 1738,
3000 DR Rotterdam, The Netherlands
Received 30 May 2000; accepted 10 May 2001
Abstract
Rationalising rationing: economic and other
considerations in the debate about funding of
Elly A. Stolk *, Werner B.F. Brouwer, Jan J.V. Busschbach
Institute for Medical Technology Assessment, Erasmus Uni6ersity Rotterdam, PO Box 1738,
3000 DR Rotterdam, The Netherlands
Received 30 May 2000; accepted 10 May 2001
Abstract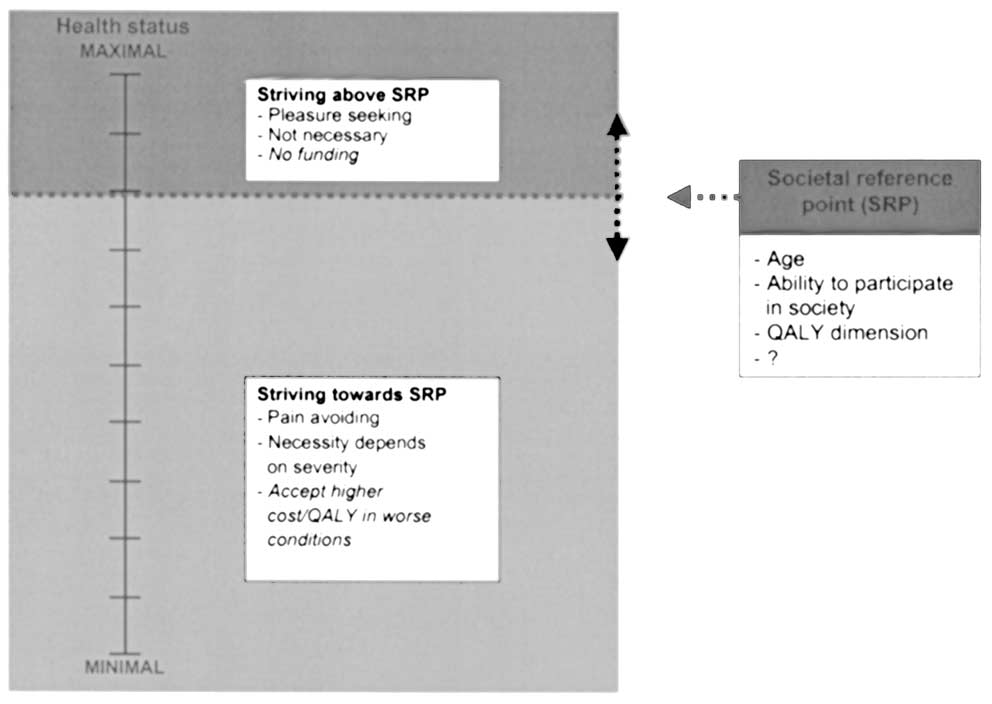 E.A. Stolk et al. / Health Policy 59 (2002) 53 – 63
Fig. 1. Hypothetical decision-making framework.
E.A. Stolk et al. / Health Policy 59 (2002) 53 – 63
Fig. 1. Hypothetical decision-making framework.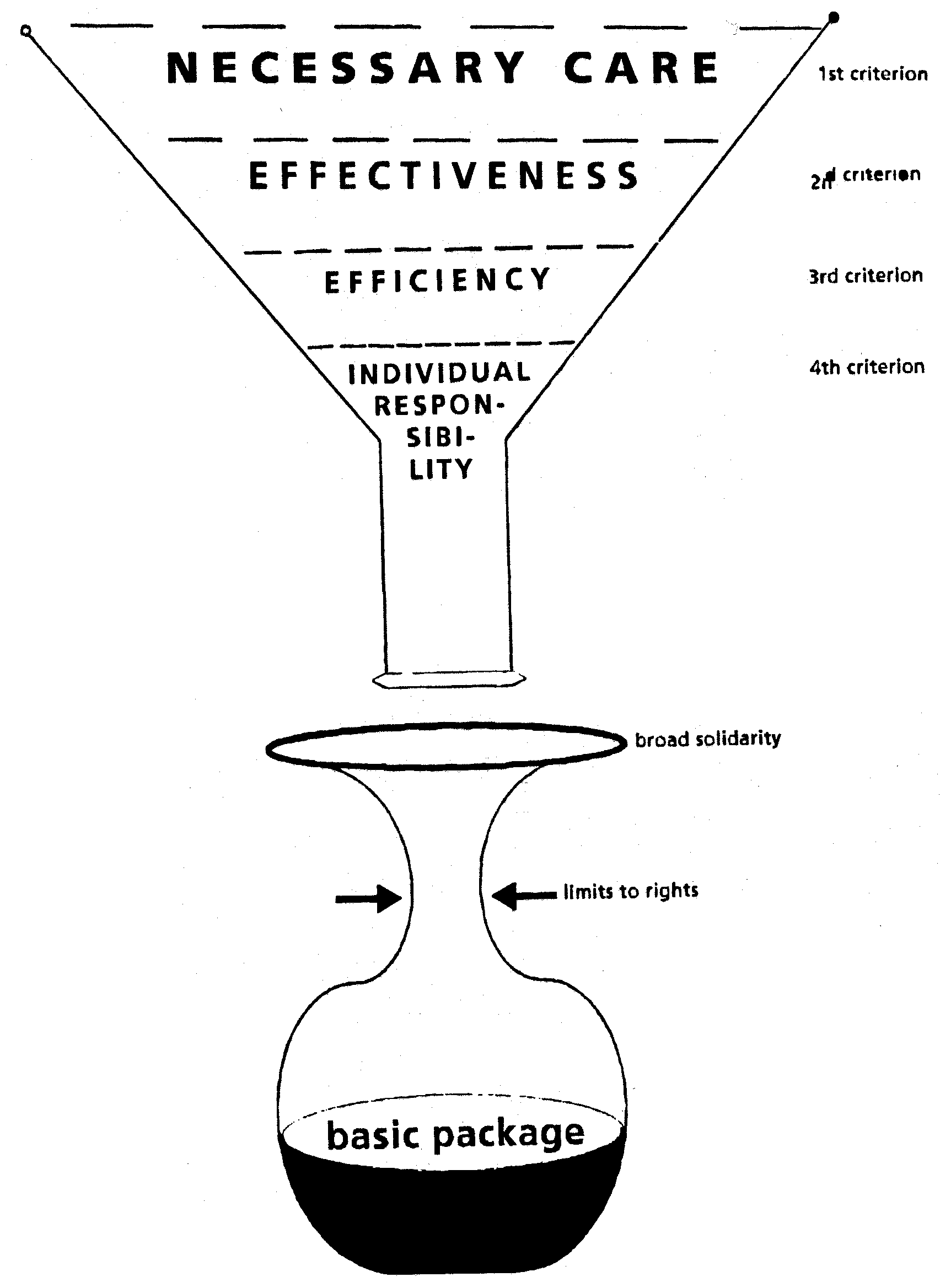 E.A. Stolk et al. / Health Policy 59 (2002) 53 – 63
4. Implications for decision making
E.A. Stolk et al. / Health Policy 59 (2002) 53 – 63
4. Implications for decision making