Effect of caffeine on metabolism, exercise endurance,and catecholamine responses after withdrawal
M. H. VAN SOEREN1 AND T. E. GRAHAM21School of Nursing, Faculty of Health Sciences, University of Western Ontario, London,Ontario N6A 5C1; and 2Human Biology and Nutritional Sciences, University of Guelph,Guelph, Ontario, Canada N1G 2W1Van Soeren, M. H., and T. E. Graham. Effect of caffeine
assumptions that prior caffeine use alters hormonal
on metabolism, exercise endurance, and catecholamine re-
and metabolic responses to acute caffeine ingestion and
sponses after withdrawal. J. Appl. Physiol. 85(4): 1493–1501,
that this process is reversible. If epinephrine is a
1998.—In this study the effects of acute caffeine ingestion on
critical element in the ergogenic effect after caffeine
exercise performance, hormonal (epinephrine, norepineph-
consumption, then attenuation of caffeine-induced in-
rine, insulin), and metabolic (free fatty acids, glycerol, glu-
creases in plasma epinephrine in habitual caffeine
cose, lactate, expired gases) parameters during short-termwithdrawal from dietary caffeine were investigated. Recre-
consumers may also dampen the performance and
ational athletes who were habitual caffeine users (n ϭ 6)
metabolic effects of caffeine during exercise.
(maximum oxygen uptake 54.5 Ϯ 3.3 ml · kgϪ1 · minϪ1 and
In vivo, the major mechanism through which caffeine
daily caffeine intake 761.3 Ϯ 11.8 mg/day) were tested under
acts is as an adenosine-receptor antagonist (1), and all
conditions of no withdrawal and 2-day and 4-day withdrawal
tissues with adenosine receptors may be affected by
from dietary caffeine. There were seven trials in total with a
caffeine exposure. Chronic exposure to caffeine results
minimum of 10 days between trials. On the day of the exercise
in increases in both available adenosine receptors
trial, subjects ingested either dextrose placebo or 6 mg/kg
and/or receptor-mediated activity in humans and ani-
caffeine in capsule form 1 h before cycle ergometry to exhaus-
mals (4, 8). Thus, during periods of short-term with-
tion at 80–85% of maximum oxygen uptake. Test substances
drawal from dietary caffeine, acute caffeine ingestion
were assigned in a random, double-blind manner. A finalplacebo control trial completed the experiment. There was no
may result in an enhancement of the caffeine-induced
significant difference in any measured parameters among
responses, such as increases in plasma epinephrine,
days of withdrawal after ingestion of placebo. At exhaustion
during exercise. We (32) previously demonstrated that
in the 2- and 4-day withdrawal trials, there were significant
increased epinephrine responses occur during submaxi-
increases in plasma norepinephrine in response to caffeine
mal exercise in habitual caffeine users with or without
ingestion. Caffeine-induced increases in serum free fatty
acute ingestion of caffeine. Others have reported con-
acids occurred after 4 days and only at rest. Subjects re-
flicting epinephrine responses in subjects whose prior
sponded to caffeine with increases in plasma epinephrine
caffeine usage was known (2, 18, 30). A single study has
(P Ͻ 0.05) at exhaustion and prolonged exercise time in all
specifically addressed the issue of habituation to caf-
caffeine trials compared with placebo, regardless of with-
feine during exercise and found no change in substrate
drawal from caffeine. It is concluded that increased endur-ance is unrelated to hormonal or metabolic changes and that
utilization after a 48-h withdrawal from caffeine (21).
it is not related to prior caffeine habituation in recreational
However, these authors did not measure methylxanthines,
catecholamines, or endurance, all of which may be criti-cally altered after withdrawal from dietary caffeine.
norepinephrine; epinephrine; methylxanthines; performance;
The present study was designed to test the hypoth-
esis that caffeine-induced changes in metabolic andcatecholamine responses and in exercise performanceare less pronounced during periods of chronic caffeine
ACUTE INGESTION OF CAFFEINE before exercise has been
ingestion, thus influencing the ergogenic response to
shown to prolong exercise endurance, increase plasma
caffeine ingestion. It is anticipated that this dampening
epinephrine and serum free fatty acids (FFAs), and
of responses will be reversed after short-term with-
spare muscle glycogen (14, 18, 29). Research has been
drawal from caffeine. Recreational athletes were tested
directed toward establishing a causal relationship be-
during exercise to exhaustion under conditions of no
tween these parameters on the basis of the hypothesis
withdrawal and 2 and 4 days of withdrawal from all
that caffeine ingestion resulted in a rise in circulating
dietary caffeine. Caffeine-induced hormonal and meta-
catecholamines, which mobilized FFAs from adipo-
bolic responses and exercise endurance were examined to
cytes, thus increasing the amount of fat available for
determine the effect of habituation and withdrawal in
active muscle (10, 14, 22). The ergogenic effect was
caffeine users during high-intensity cycling exercise under
thought to be a result of utilization of fat and a resulting
conditions of placebo or acute caffeine ingestion (6 mg/kg).
sparing of muscle glycogen (14). These concepts weretested into the 1990s (18, 29), but more recent research has
failed to support this hypothesis (7, 19).
In humans at rest, Robertson et al. (27) found that
moderate prolonged caffeine use was sufficient to
Six recreational male athletes agreed to participate in the
dampen the caffeine-induced epinephrine response.
study after being informed of the nature of the experiments.
There are few exercise studies (2, 21, 32) that test the
Subjects were nonsmokers and had been actively cycling
8750-7587/98 $5.00 Copyright 1998 the American Physiological Society
CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
and/or running five times per week for at least 1 yr (n ϭ 5) or
five times per week for 3 mo (n ϭ 1). Subjects were 36.7 Ϯ 4.2(SE) yr of age, weighed 75.1 Ϯ 1.6 kg, and had an average
The protocol for each trial was identical. Trials were held at
daily caffeine consumption from all sources equivalent to
the same time of day for each subject and typically started at
761.3 Ϯ 11.8 mg/day [based on self-reporting and using
0900. Before each trial, a venous catheter was inserted into
amounts recommended by Conlee (9)]. Their primary source
the antecubital vein and was kept patent with a saline
of dietary caffeine was from coffee. Each subject signed a
infusion. The subject then rested in a supine position for 15
consent form that outlined possible risks of the procedure.
min before any further testing. A resting blood sample of 12
The protocol was approved by the University of Guelph Ethics
ml was then collected, and the subject ingested the trial
substance in gelatin capsules with water (Ϫ60 min). After 1 hof rest, during which time the subject was allowed to sit or lie
quietly, another resting blood sample was obtained (0 min). Subjects then exercised to exhaustion at 80–85% V
Subjects reported to the laboratory before the start of the
cycle ergometer. Each subject completed a 5 min warm-up at
experiment for an incremental maximum oxygen uptake
a lower power output, which was identical for all trials and
˙ O2max) test on a cycle ergometer from which a power output was not considered as part of the total exercise time.
Samples for expired air were taken every 5 min during the
was 54.5 Ϯ 3.3 ml · kgϪ1 · minϪ1. They returned for at least one
initial 20 min of exercise, and blood samples (12 ml) were
additional trial ride of 30-min duration to confirm the power
taken at 5 and 20 min after the warm-up period. A final blood
˙ O2max and to habituate and an expired air sample were taken within 2 min before the
point of exhaustion. No samples were taken between 20 min
Subjects were requested to maintain similar exercise pat-
and exhaustion so that subjects could not count samples as a
terns throughout the duration of the experiments, to follow
crude timing device. Exhaustion was determined by the
constant activity patterns for the 3 days before each test, and
investigator when cadence could no longer be maintained at a
to abstain from exercise 24 h before each trial. They were
rate of 90% of the subject’s set rate. When the researchers
requested to consume similar diets for 48 h before each
thought the subject was close to exhaustion, a sample was
experiment, and each maintained a diet record for this period.
taken. If the subject did not demonstrate decreased cadence
When they were required to abstain from caffeine (i.e.,
within 2 min of that sample, another sample was taken, and
withdrawal), they were cautioned to avoid sources of methyl-
the former was discarded. Water was given ad libitum during
xanthines such as tea, coffee, chocolate, cola drinks, and
exercise. Subjects did not have access to any indication of
caffeine-containing over-the-counter pharmaceuticals, and
time after the initial 20-min sampling period during the
they were asked to report any deviations from these instruc-
tions. For the no-withdrawal trials they were allowed toconsume products containing caffeine up to the morning of
the trial. Subjects were requested to consume a small meal2–4 h before the experiment, which was identical for each
Expired gas samples were analyzed for fractions of O2 and
trial. Dietary consistency was confirmed through self-
CO2 with an Applied Electrochemical S-3A O2 analyzer and
reported diet records and questioning before each trial.
Sensor Medics LB-2 CO2 detector, respectively. Expired vol-
Subjective withdrawal symptoms were recorded for each
ume was determined with a Parkinson-Cowan volumeter.
The analyzers were calibrated with gases of known concentra-
Seven exercise trials to exhaustion were completed by all
tions, previously determined by micro-Scholander technique.
subjects. A minimum of 10 days between all trials was
The volume meter was calibrated with a Tissot spirometer.
established to minimize any possible effects of the abstinence
Blood samples were immediately separated into two ali-
from normal caffeine intake. The first two trials were com-
quots: 3 ml were transferred to a nontreated tube for serum,
pleted without any withdrawal from dietary caffeine, and
and 7 ml were transferred into a sodium heparinized tube.
subjects were assigned randomly either dextrose placebo (Pl
Hematocrit was immediately measured in triplicate from the
0d) or caffeine (Caf 0d; 6 mg/kg body wt; Caffeine US
latter tube by using high-speed centrifugation. Hemoconcen-
Pharmaceutical/Federal Commerce Comission catalog no.
tration occurred in all the exercise samples, but there was no
C-0905, A&C American Chemicals). It was believed that the
difference between trials. An aliquot of 100 µl heparinized
tests under normal habituation would most likely mimic the
blood was added to 500 µl of 0.3 M perchloric acid. A solution
responses in other comparable studies, and therefore the
containing 120 µl of 0.24 M EGTA and reduced glutathione
protocol was designed with these tests before withdrawal was
was then added to the remaining heparinized whole blood.
commenced. Subsequent exercise trials were conducted after
The EGTA and glutathione treated plasma was analyzed
periods of either a 2- or 4-day withdrawal from dietary
for epinephrine and norepinephrine (NE) concentration by
caffeine and are designated as Pl 2d and Pl 4d, for the placebo
using HPLC (Waters) as described by Weiker et al. (34).
2- and 4-day withdrawals, respectively, and as Caf 2d and Caf
Plasma caffeine was analyzed by using fully automated
4d for the caffeine 2- and 4-day withdrawals, respectively.
HPLC (Waters). For the latter procedure, plasma samples
Both the sequence of days of withdrawal and the receipt of
were subjected to centrifugal filtration by using Ultrafree-MC
caffeine or placebo were assigned in a random, double-blind
polysulfone filter units (Millipore UFC3TGC). Filtered plasma
manner for all trials. After these experiments all subjects
and the internal standard -hydroxyethyltheophylline were
participated in a placebo-repeat trial (Pl R) (administered in a
injected onto a resolve Radial-Pak cartridge (Waters 84624)
single-blind manner) without any period of withdrawal from
by using a Radial Compression Module 8 ϫ 10 pressure
caffeine as a control to test for a training effect after the 3- to
module. Caffeine was measured at 254-nm wavelength and
6-mo period required to complete the trials. At the completion
sensitivity range of 0.01 absorbance units full scale. Reagents
of each exercise trial, subjects were asked to complete a
for standards were obtained from Sigma Chemical.
questionnaire inquiring whether they could determine which
The whole-blood acid extracts were analyzed enzymatically
drug they had received and to describe the basis on which
in triplicate for lactate and glucose as described by Berg-
meyer (3). Serum was analyzed enzymatically in triplicate for
CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
FFAs (26) and glycerol (16). Plasma insulin was analyzed by
6.7 vs. 59.5 Ϯ 8.4 min), and the 4-day withdrawal
using 125I radioimmunoassay kit (Diagnostic Products Code-a-
(81.5 Ϯ 6.4 vs. 63.6 Ϯ 5.6 min). In contrast to the Pl 0d
Count Insulin kit). Diet analysis was completed as described
trial, the time to exhaustion in the Pl R trial was not
significantly different than in the Caf 0d trial. This
increase in time for the Pl R trial is heavily influencedby a single subject whose time increased from 70 to 124
Statistical analysis of respiratory, exercise, and blood data
min (Pl 0d vs. Pl R, respectively). When this subject’s
was conducted by using repeated-measures analysis of vari-
data are removed from the analyses, the Pl R and Caf
ance for drug and withdrawal. Bonferroni corrected t-tests
0d trials are significantly different, because all other
were used to adjust ␣ levels to limit the possibility of a type I
subjects performed similarly in both Pl trials.
error. A one-way analysis of variance was used to test thedifference between Pl 0d and Pl R data as well as Caf 0d and
Pl R data. Experimental significance is described as P Ͻ 0.05,and all data are reported as means Ϯ SE. Because of the small
Ingestion of caffeine resulted in a significant increase
number of subjects, observed power calculations were com-
in plasma epinephrine concentration in all trials at
pleted and were found to be ϳ0.500 for all nonsignificant
exhaustion compared with that of placebo regardless of
the days of withdrawal (F ϭ 11.090, P ϭ 0.007; Fig. 2).
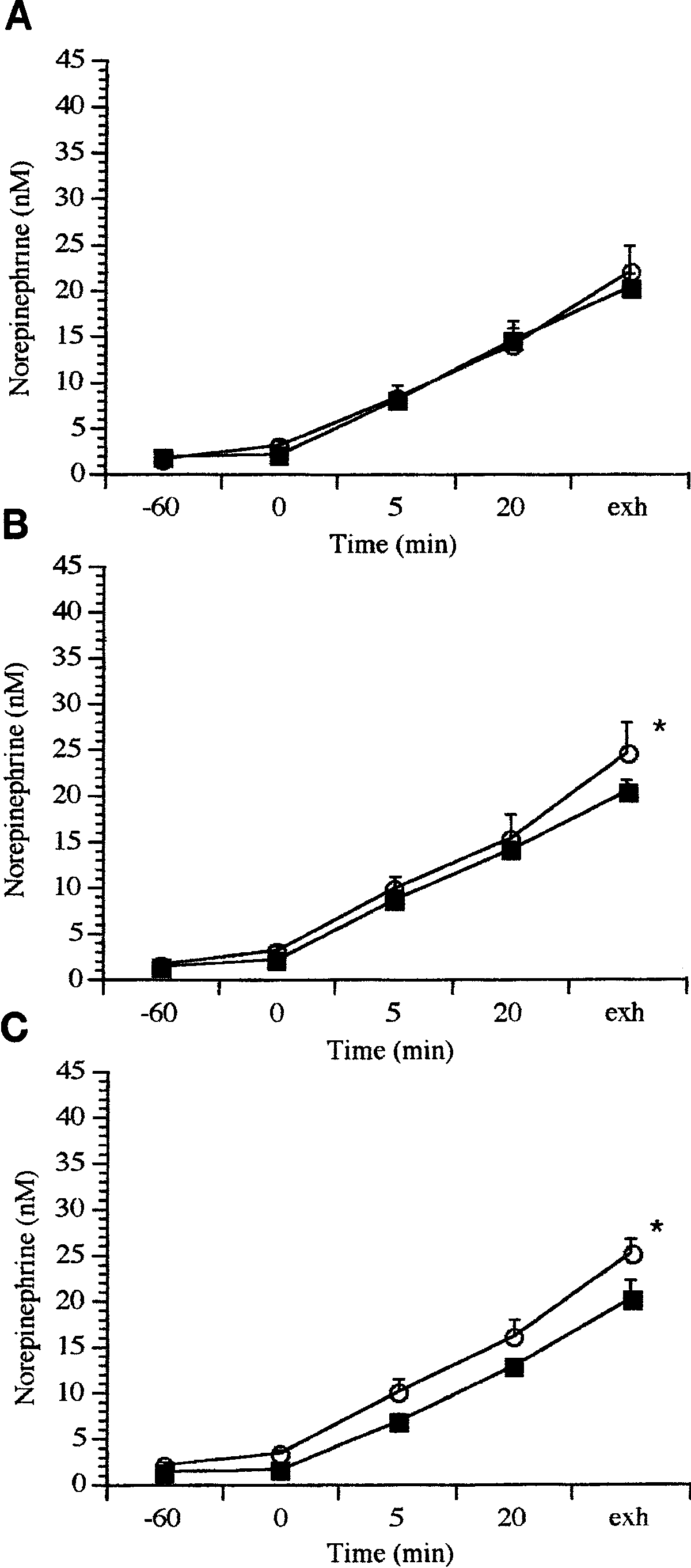
There was an effect of withdrawal on NE responses tocaffeine. Caffeine ingestion resulted in significantly
There was no significant difference between the Pl 0d
elevated plasma NE concentrations over the placebo
and the Pl R trials in any of the measured parameters.
conditions at exhaustion in the 2- and 4-day with-
Although the original purpose of the Pl R trial was for
drawal trials, but NE levels were similar to placebo in
use as a comparison with the Pl 0d trial, statistical
the no-withdrawal trial (F ϭ 8.793, P ϭ 0.006; Fig. 3).
comparison of the Pl R and Caf 0d data was completed. These data followed a similar pattern of significance as
did the Pl 0d vs. Caf 0d data, with the exception of thetime data. Therefore, the Pl R data will be shown only
Insulin concentration declined with exercise, and
with respect to time to exhaustion (Fig. 1).
there were no significant differences in any of the trialsafter ingestion of caffeine (data not shown). Initial
values for the no-withdrawal trials were 9.0 Ϯ 3.0 and10.6 Ϯ 3.6 µU/ml at Ϫ60 min, which decreased to 2.7 Ϯ
Time to exhaustion was significantly increased over
0.4 and 5.5 Ϯ 2.4 µU/ml at exhaustion, for placebo and
placebo in all caffeine trials regardless of the period of
withdrawal (Fig. 1). Ingestion of caffeine significantlyincreased the time to exhaustion in all subjects after no
withdrawal (74.8 Ϯ 8.8 vs. 59.0 Ϯ 3.7 min for caffeinevs. placebo, respectively), the 2-day withdrawal (81.1 Ϯ
FFAs. There is a significant effect of caffeine inges-
tion on FFA concentrations (F ϭ 25.100, P ϭ 0.004). This significant increase occurred in the 4-day trialafter caffeine ingestion when FFA concentration in-creased at rest from 0.22 Ϯ 0.04 mM (Ϫ60 min) beforecaffeine ingestion to 0.45 Ϯ 0.12 mM (0 min) comparedwith the Pl 4d data. At no other time or treatment wereFFA concentrations significantly altered by caffeine orwithdrawal (Table 1). Glycerol. Regardless of whether the treatment was
placebo or caffeine, serum glycerol concentration in-creased gradually during the initial exercise period andwas elevated at exhaustion in all trials (F ϭ 46.219, P ϭ0.0001) (Table 1). After the 4-day withdrawal fromcaffeine ingestion, there was an increase in glycerolconcentration compared with that in the placebo trial,but this was not significant. Glucose. Blood glucose concentration was not altered
by either days of withdrawal or caffeine ingestion(Table 2). A low initial glucose concentration at Ϫ60min in the Caf 0d trial was demonstrated in four of the
Fig. 1. Time to exhaustion in all exercise trials. Trials are groupedaccording to drug treatment [placebo (Pl) vs. caffeine (Caf; 6 mg/kg
six subjects despite their reported similar diet and
body wt)] and days of withdrawal [no withdrawal (0 days; 0d) or 2-day
activity pattern before experimentation.
(2d) or 4-day withdrawal (4d)]. Pl 0d, initial-placebo, no-withdrawal
Lactate. Blood lactate increased in response to exer-
exercise trial; Pl R, placebo-repeat, no-withdrawal exercise trial,
cise in all trials (Fig. 4). After the 2 days of withdrawal,
which was performed on completion of all other withdrawal periods.
acute ingestion of caffeine resulted in a tendency
Bars are mean data, and vertical lines indicate SE. a Significantdifference from Pl 0d, P Ͻ 0.05.
toward an increase in lactate concentration at exhaus-
CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
amounts of residual caffeine may be detected in plasma. When there was no withdrawal, the initial mean plasmacaffeine concentration was 7.11 Ϯ 2.26 (caffeine) and10.99 Ϯ 3.09 (placebo) µM. In the Pl 0d trial, thecaffeine concentration was significantly higher than inother placebo trials. Despite the higher initial value inthe Caf 0d trial, there was no significant difference inmaximal concentrations measured in the caffeine tri-als. Expired gases. There was no significant difference
found in any of the measured parameters of oxygen
Plasma epinephrine concentration during exercise under
conditions of no withdrawal (A) and 2-day (B) and 4-day withdrawal(C) from dietary caffeine. Lines are mean data, and vertical bars areSE; n ϭ 6 subjects. Time indicates sampling time: Ϫ60, preingestion;0, 1 h of rest postingestion at start of exercise; 5 and 20, timefrom start of exercise; exhaustion (exh), end of exercise when subjectcould no longer maintain a power output of 85% maximum oxygenuptake. j, Placebo; s, caffeine. * Significant difference from placebo,P Ͻ 0.05.
tion compared with that at Pl 2d, and after the 4-daywithdrawal this trend increased to include increases atboth 20 min and exhaustion. However, this was notstatistically significant.
Fig. 3. Plasma norepinephrine concentrations during exercise under
Plasma caffeine. Mean plasma caffeine data are
conditions of no withdrawal (A) and 2-day (B) and 4-day withdrawalfrom dietary caffeine (C). Lines are mean data, and vertical bars are
presented in Table 3. These data indicate that, after a
SE; n ϭ 6 subjects. j, Placebo; s, caffeine. Organization is as in
period of even up to 4 days of withdrawal, trace
Fig. 2. * Significant difference from placebo, P Ͻ 0.05.
CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
Table 1. Serum free fatty acids and glycerol
0.22Ϯ0.04 0.45Ϯ0.12* 0.25Ϯ0.02 0.34Ϯ0.08 0.60Ϯ0.10
Values are means Ϯ SE given in mM for 6 subjects for placebo (Pl)
and caffeine (Caf) trials; 0d, no withdrawal; 2d, 2-day withdrawal; 4d,4-day withdrawal. Time points indicate before 4d ingestion (Ϫ60),after 1 h rest (0), after 5 and 20 min of exercise, and at exhaustion(Exh) when power output could no longer be maintained. FFA, freefatty acids. * Significantly different from Pl within same protocol,P Ͻ 0.05.
consumption, carbon dioxide production, V
not shown), or respiratory exchange ratio (RER)(Table 4). Each subject achieved ϳ85% V
0.05 ml · kgϪ1 · minϪ1) by the 20-min time point duringexercise as calculated from the initial V
maintained this power output until near exhaustion. Diet. On the basis of self-reported diet records, there
were no significant differences between subjects andbetween trials for a given subject with respect to thepercentage of dietary fat, carbohydrate, and protein. Subjects consumed a mixed diet of 30–35% fat, 50–54%carbohydrate, and 12–14% protein. Subjects reportedthat they maintained the same diet immediately beforeeach trial. Perception of trial substance. When asked by question-
naire to identify which substance they had received,subjects generally correctly identified the trial sub-stances, with some exceptions. One subject was unableto discriminate between caffeine and placebo on mostoccasions (incorrect in 5 of 7 trials). Another subject dididentify caffeine correctly but was unable to definitelyidentify placebo during periods of withdrawal. The
Whole-blood lactate concentration during exercise under
subjects’ justification for guessing caffeine included
conditions of no withdrawal (A) and 2-day (B) and 4-day withdrawal(C) from dietary caffeine. Lines are mean data, and vertical bars are
feelings of alertness, less fatigue during exercise, caf-
SE; n ϭ 6 subjects. j, Placebo; s, caffeine. Organization is as inFig. 2.
feine-induced diuresis, and talkativeness. The with-
drawal symptoms varied in severity among subjectsand between similar withdrawal periods. DISCUSSION
4.40Ϯ0.57 3.68Ϯ0.28 4.25Ϯ0.26 4.45Ϯ0.37 4.25Ϯ0.50
4.26Ϯ0.57 3.23Ϯ0.53 3.48Ϯ0.38 3.50Ϯ0.52 3.44Ϯ0.47
In this study the effects of short-term withdrawal
Ϯ0.41 3.67Ϯ0.47 3.41Ϯ0.14 3.71Ϯ0.21 3.42Ϯ0.28
2.97Ϯ0.53 3.99Ϯ0.54 3.23Ϯ0.56 3.47Ϯ0.43 2.96Ϯ0.62
from dietary caffeine during high-intensity exercise on
3.38Ϯ0.12 3.37Ϯ0.42 3.40Ϯ0.29 3.89Ϯ0.22 3.61Ϯ0.20
hormonal, metabolic, and endurance responses with or
3.53Ϯ0.45 4.31Ϯ0.45 4.12Ϯ0.66 4.62Ϯ0.29 3.55Ϯ0.62
without acute ingestion of caffeine were examined. The
Values are means Ϯ SE in mM for 6 subjects.
present study is the first to investigate the effect of
CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
Table 3. Mean plasma caffeine data
Values are means Ϯ SE in µM for 6 subjects. Ingestion of caffeine resulted in significantly greater concentration vs. placebo.
withdrawal from dietary caffeine over the critical 4-day
days) and then were tested by using standardized
period in which tolerance to caffeine and withdrawal
exercise trials. Exercise performance data throughout
symptoms are reported (27), and it is unique in the
all days of withdrawal in the placebo trials were
examination of the influence that prior caffeine use
similar, indicating changes in the caffeine trials were a
may have on epinephrine and ergogenic responses
result of acute caffeine ingestion and were not a product
during high-intensity exercise. Under the placebo con-
dition, days of withdrawal, i.e., 0, 2, or 4 days, did not
In many exercise studies, the pharmacological prop-
alter the basic responses in any measured parameters.
erties of caffeine regarding tolerance to the metabolic
Withdrawal from caffeine resulted in caffeine-induced
effects have not been considered. Adenosine receptors
changes in serum FFAs at 4 days and in plasma NE
are widely distributed throughout the body in the
responses at 2 and 4 days. The significance of the
brain, adipose tissue, smooth and cardiac muscle, and
changes in concentration of these metabolites after
adrenal gland. If caffeine acts primarily as an adenosine-
acute caffeine ingestion is uncertain because with-
receptor antagonist in vivo, then short-term with-
drawal from dietary caffeine did not alter either the
drawal should result in significant enhancement (upreg-
ergogenic or the epinephrine response.
ulation) (24), suggesting that adenosine-mediated
When the exercise literature is reviewed, there is
effects will be more pronounced. In contrast to findings
inconsistency found regarding the ergogenic effect of
in resting subjects, we demonstrate here an increase in
caffeine that may be attributable to lack of control of
plasma epinephrine in response to exercise and caffeine
prior caffeine use in the subjects. In two studies in
regardless of the state of habituation or withdrawal.
which a positive ergogenic effect is reported (18, 29), a
Robertson et al. (27) found that prior caffeine use
48-h withdrawal from dietary caffeine was used before
resulted in attenuation of the caffeine-induced increase
testing. In other studies, when prior caffeine use is not
in plasma epinephrine concentration, and a 4-day
reported, some authors found no effect (6, 13, 28) and
period of abstinence was used to restore the expected
others a positive response (10, 14, 22). The similar
epinephrine increase after acute caffeine ingestion. On
longer exhaustion times in the caffeine trials in all
the basis of this literature and other research involving
subjects reported here suggests that withdrawal from
adenosine-receptor-mediated responses (4), we deter-
caffeine before testing was not a factor in this variation.
mined that a 2- and a 4-day withdrawal would be
The mean time to exhaustion in the Pl R trial com-
adequate to observe any metabolic and hormonal
pleted in this study was not significantly different from
changes that occur during the transition from habitua-
that in the Caf 0d as a result of one subject almost
tion through withdrawal. The lack of epinephrine re-
doubling his exercise time during the Pl R trial vs. the
sponse to withdrawal after acute caffeine ingestion
Caf 0d. This suggests that variation in this time to
reported here both at rest and during exercise may be
exhaustion in studies in which a small number of
due to the exercise intensity. It appears that the strong
subjects were used may have influenced previous re-
sympathetic stimulus of exhaustive exercise during
sults. To minimize confounding variables, our subjects
habituation and withdrawal acts to surmount tolerance
regulated their diet and exercise activity for 48 h before
to the caffeine stimulus, which contributed to the
testing during all phases of withdrawal (0, 2, and 4
uniform rise in plasma epinephrine at exhaustion
Values are means Ϯ SE for 6 subjects. RER, respiratory exchange ratio.
CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
regardless of dietary caffeine use before experimenta-
rather than through secondary stimulation via the
An alternative explanation for the changes in epi-
The complexity of the metabolic responses to acute
nephrine and NE concentrations at exhaustion in the
caffeine ingestion during exercise makes dissociation of
caffeine trials would include a linear relationship be-
the possible causal effects difficult to distinguish. Distri-
tween time to exhaustion and increases in plasma
bution of adenosine receptors throughout the periph-
catecholamines rather than a caffeine effect. In the
eral tissues and the central nervous system suggests
present study, it is impossible to determine whether the
that caffeine may act directly or indirectly through
effect on catecholamines is merely a result of a longer
multiple mechanisms (4, 17, 25, 31). Additional support
duration of exercise. However, in examining the data,
for the direct action of caffeine on specific tissues can be
epinephrine concentrations are similar between the
found in several studies (25, 32). Lopes et al. (25) used
Caf 0d trial and the Caf 4d trial, despite the latter
electrical stimulation of the adductor pollicis after
lasting 7 min longer. The changes in NE are more
ingestion of caffeine to dissociate both metabolic and
difficult to interpret because of the similarity of time
centrally mediated effects from increases in time to
between 2- and 4 day trials. Because of the uncertainty
fatigue. Subsequent research is needed to determine
of interpreting catecholamine data from this study,
whether it is peripheral vs. centrally mediated effects
further research will be needed to determine the rela-
that are significant in the caffeine-mediated ergogenic
tionship between caffeine-induced changes in epineph-
rine concentration during exercise and time to exhaus-
To investigate whether our results could be influ-
tion. Regardless, the number of days of withdrawal
enced by variations in available plasma concentrations
from caffeine did not influence the ergogenic effects of
of methylxanthines, the measurements of caffeine con-
acute caffeine ingestion, and the mechanism for this
centrations before and during exercise in this study
may be related to a number of factors.
were used to confirm compliance to the protocol and as
These data indicate that acute caffeine ingestion
an indication of the similarity of drug stimulus between
during short-term withdrawal alters mobilization of
trials. Despite high plasma caffeine concentrations in
serum FFA. The changes in serum concentrations after
the Pl 0d trial (ϳ10 µM), changes in performance did
withdrawal from caffeine may not have altered uptake
not occur until greater concentrations (Ͼ30 µM) were
or oxidation because there was no significant impact on
achieved in the caffeine trials. Graham and Spriet (19)
RER, but without arteriovenous data this remains
report that plasma caffeine concentrations of 18 µM
speculative. Our data are in agreement with those
(after ingestion of 3 mg/kg caffeine) result in ergogenic
reported by Hetzler et al. (21), who found that acute
effects. Whether there is a critical concentration be-
withdrawal from caffeine did not alter substrate utiliza-
tween 10 and 18 µM that represents a threshold of
tion during submaximal exercise. However, these inves-tigators limited their study to a 48-h interval to test
caffeine activity during exercise is not known.
withdrawal, which we believed was not sufficient be-
Withdrawal from dietary caffeine did not alter the
cause there is considerable variability in the reported
maximal plasma caffeine concentration during exercise
time course of symptoms of withdrawal from 12 to 48 h
despite the presence of higher initial concentrations in
(20). In a study by Biaggioni et al. (4), a 60-h with-
the no-withdrawal trial. This is consistent with the
drawal was required to alter adenosine-mediated plate-
data available regarding caffeine metabolism in the
let response to methylxanthines in human subjects.
liver. The cytochrome P-450 isoform 1A2, which repre-
This proved to be the case with respect to serum FFA
sents the major pathway for caffeine 1-and 7-demethyl-
responses in our subjects, in whom there was a signifi-
ations (23), is saturable (12), and steady-state concen-
cant caffeine effect after a 4-day withdrawal, which would
trations were achieved over the time course in the
have been missed if only 2 days were investigated.
present study. Factors that would alter the activity of
To counteract the possibility of a statistical error due
the P450 1A2 enzyme include smoking, oral contracep-
to multiple comparisons, the Bonferroni corrected t-test
tive use, ingestion of cruciferous vegetables, and physi-
was applied, increasing the rigor of acceptance of the
cal fitness (5, 33). Subjects in the present experiment
null hypothesis. Therefore, the significant changes in
did not smoke or use oral contraceptives, and diet
both FFA at rest and NE during exercise in the present
analysis indicated no use of cruciferous vegetables.
study are likely a result of withdrawal from caffeine.
They maintained the same level of fitness throughout
Whether the absence of enhanced substrate utilization
the experiment. Therefore, these factors would have
would have continued over 4 days in the work of
minor, if any, effect on available plasma concentrations
Hetzler et al. (21) is not known, and the lack of
of caffeine and are unlikely to have influenced findings
methylxanthine data in their research makes interpre-
in this study. Subjects arrived after a 4-day withdrawal
tation of prior caffeine status impossible to establish.
from caffeine with small, but measurable, caffeine
However, these data, coupled with the present findings,
concentrations, which is consistent with the wide vari-
suggest that the mechanism through which caffeine
ability in caffeine half-life (1.5–9.5 h) (21). The minor
acts to enhance exercise performance may not be linked
increase of 15–20% in plasma caffeine concentration in
to changes in adipose lipolysis. The increase in lipolysis
the Caf 0d vs. the Caf 2d or Caf 4d trials did not
may be related to the direct systemic effects of caffeine
influence results reported here, which is in agreement
ingestion (31) through action on adenosine receptors
with Graham and Spriet (19), who found no difference
CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
in performance between ingestion of 3 vs. 6 mg/kg of
unlikely to be through changes in available metabolic
substrates or catecholamines but rather is through
The ability to discriminate caffeine has been tested in
some direct action of caffeine on tissues as yet to be
humans and animals (20, 24). Because of the effects of
caffeine in humans on arousal and awareness, we
The authors acknowledge the technical support of Premila Satha-
recorded our subjects’ observations of their trial sub-
sivam for analysis of catecholamine and caffeine data.
stances. The majority of subjects correctly identified
This study was supported by grants from National Science and
caffeine by the effects of arousal and alertness, and,
Engineering Research Council of Canada and Sport Canada and byGatorade Sports Science Student Awards.
therefore, it is difficult to claim that they did not know
Address for reprint requests: M. van Soeren, NP/CNS ICU, St.
which trial substance had been given. The effect on
Joseph’s Health Centre, 268 Grosvenor St., London, Ontario, Canada
their performance, therefore, may have been influenced
N6A 4V2 (E-mail: [email protected]).
in some way by knowledge that they had received
Received 20 August 1997; accepted in final form 1 June 1998.
caffeine; however, the consistently longer exercise times
REFERENCES
to exhaustion in the caffeine trials for all subjects, eventhose who guessed incorrectly, suggests that this was
1. Ammon, H. P. Biochemical mechanism of caffeine tolerance. Arch. Pharm. (Weinheim) 324: 261–267, 1990.
not a significant factor in these results.
2. Bangsbo, J., K. Jacobsen, N. Nordberg, N. J. Christensen,
All of the subjects tested in the present study subjec-
and T. E. Graham. Acute and habitual caffeine ingestion and
tively reported withdrawal symptoms lasting from 2 to
metabolic responses to steady-state exercise. J. Appl. Physiol. 72:
4 days. These included severe headaches, fatigue, leth-
argy, and flulike symptoms, indicating that they were
3. Bergmeyer, H. U. (Editor). Methods for determination of metabo-
lites. In: Methods in Enzymatic Analysis. New York: Academic,
experiencing a reversal of the effects of habituation to
caffeine. In animals and humans, the symptoms of
4. Biaggioni, I., S. Paul, A. Puckett, and C. Arzubiaga. Caffeine
withdrawal are thought to be associated with upregula-
and theophylline as adenosine receptor antagonists in humans.
tion of adenosine receptors after prolonged caffeine
J. Pharmacol. Exp. Ther. 258: 588–593, 1991.
5. Boel, J., L. B. Anderson, B. Rasmussen, S. H. Hansen, and
administration (4, 24). Therefore, it would be expected
M. Dossing. Hepatic drug metabolism and physical fitness. Clin.
that metabolic and hormonal responses in humans
Pharmacol. Ther. 36: 121–126, 1984.
mediated through adenosine receptors would be altered
6. Casal, D. C., and A. S. Leon. Failure of caffeine to affect
during short-term withdrawal from caffeine. The signifi-
substrate utilization during prolonged running. Med. Sci. SportsExerc. 17: 174–179, 1985.
cant increase in serum FFAs at rest and the increased
7. Chesley, A., E. Hultman, and L. L. Spriet. Effects of epineph-
plasma NE responses after a 2- and 4-day withdrawal,
rine infusion on muscle glycogenolysis during intense aerobic
and the trend for increases in whole-blood lactate
exercise. Am. J. Physiol. 268 (Endocrinol. Metab. 31): E127–
during withdrawal are indicative of an alteration in
8. Chou, D. T., S. Khan, J. Forde, and K. R. Hirsh. Caffeine
sensitivity in the metabolic responses to acute caffeine
tolerance: behavioral, electrophysiological and neurochemical
ingestion during withdrawal. Whether the ergogenic
evidence. Life Sci. 36: 2347–2358, 1985.
response after caffeine ingestion is mediated by in-
9. Conlee, R. K. Amphetamine, caffeine and cocaine. In: Ergogen-
creases in plasma epinephrine has yet to be deter-
ics: Enhancement of Performance in Exercise and Sport. India-
mined. However, the dissociation between these meta-
napolis, IN: Brown & Benchmark, 1991, p. 285–330.
10. Costill, D. L., G. P. Dalsky, and W. J. Fink. Effects of caffeine
bolic and plasma epinephrine responses suggests that
ingestion during prolonged running. Med. Sci. Sports Exerc. 10:
caffeine acts directly on specific tissues rather than
through epinephrine-mediated responses. Several re-
11. Denaro, C. P., C. R. Brown, M. Wilson, P. Jacob III, and N. L.
searchers (7, 31) have demonstrated a dissociation
Benowitz. Dose-dependency of caffeine metabolism with re- peated dosing. Clin. Pharmacol. Ther. 48: 277–285, 1990.
between caffeine-induced epinephrine and FFA re-
12. Dibbee, J., and T. E. Graham. A longitudinal study of changes
sponses, and the data reported here support these
in aerobic fitness, body composition and energy intake in primi-
findings. However, care must be taken in interpreting
gravid patients. Am. J. Obstet. Gynecol. 147: 908–914, 1983.
the results presented here because of the relative
13. Erickson, M. A., R. J. Schwarzkoff, and R. D. McKenzie.
Effects of caffeine, fructose, and glucose ingestion on muscle
insensitivity of venous blood measurements, and turn-
glycogen utilization during exercise. Med. Sci. Sports Exerc. 19:
over data would be necessary to fully understand this
relationship. Despite the need for more detailed data,
14. Essig, D., D. L. Costill, and P. J. Van Handel. Effects of
there are reasonable internally consistent data to sug-
caffeine ingestion on utilization of muscle glycogen and lipid
gest that a possible change in sensitivity at the level of
during leg ergometer cycling. Int. J. Sports Med. 1: 86–90, 1980.
15. Fredholm, J. Adenosine actions and adenosine receptors after 1
peripheral or central adenosine receptors is the mecha-
week treatment with caffeine. Acta Physiol. Scand. 115: 283–
nism of action for the ergogenic response to acute
16. Garland, P. B., and P. J. Randle. A rapid enzymatic analysis
In summary, variable periods of short-term with-
for glycerol. Nature 196: 987–988, 1962.
17. Graham, T. E., J. W. E. Rush, and M. H. van Soeren. Caffeine
drawal from dietary caffeine had no effect on caffeine-
and exercise: metabolism and performance. Can. J. Appl. Physiol.
induced increases in endurance during high-intensity
exercise compared with no withdrawal. There were
18. Graham, T. E., and L. L. Spriet. Performance and metabolic
variable responses to acute caffeine ingestion during
responses to a high caffeine dose during prolonged exercise. J.
withdrawal on FFAs and NE but no effect on plasma
Appl. Physiol. 71: 2292–2298, 1991.
19. Graham, T. E., and L. L. Spriet. Impact of various doses of
epinephrine or RER. We conclude the mechanism
caffeine on catecholamines and metabolism during exercise. J.
through which caffeine acts as an ergogenic aid is
Appl. Physiol. 78: 867–874, 1995.
CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
20. Griffiths, R. R., and P. P. Woodson. Caffeine physical depen-
28. Sasaki, H., J. Maeda, S. Usui, and T. Ishiko. Effect of caffeine
dence: a review of human and laboratory animal studies. Psycho-
ingestion on performance of prolonged strenuous running. Int. J.pharmacology (Berl.) 94: 437–451, 1988. Sports Med. 8: 261–265, 1987.
21. Hetzler, R. K., N. Warhaftig-Glynn, D. L. Thompson, E.
29. Spriet, L. L., D. A. MacLean, D. J. Dyck, E. Hultman, G. Dowling, and A. Weltman. Effects of caffeine withdrawal on Cederblad, and T. E. Graham. Caffeine ingestion and muscle
habituated male runners. J. Appl. Physiol. 76: 1043–1048, 1994.
metabolism during prolonged exercise in humans. Am. J. Physiol.
22. Ivy, J. L., D. L. Costill, W. J. Fink, and R. W. Lower. Influence
262 (Endocrinol. Metab. 25): E891–E898, 1992.
of caffeine and carbohydrate feedings on endurance performance.
30. Tarnopolsky, M. A., S. A. Atkinson, J. D. MacDougall, D. G. Med. Sci. Sports Exerc. 11: 6–11, 1979. Sale, and J. R. Sutton. Physiological responses to caffeine
23. Kalow, W., and B. K. Tang. The use of caffeine for enzyme assays: a
during endurance running in habitual caffeine users. Med. Sci.
critical appraisal. Clin. Pharmacol. Ther. 53: 503–514, 1993. Sports Exerc. 21: 418–424, 1989.
24. Kaplan, G. B., D. J. Greenblat, M. A. Kent, and M. M.
31. Van Soeren, M. H., T. Mohr, M. Kjaer, and T. E. Graham. Cotreau-Bibbo. Caffeine treatment and withdrawal in mice:
Acute effects of caffeine ingestion at rest in humans with
relationships between dosage, concentrations, locomotor activity
impaired epinephrine responses. J. Appl. Physiol. 80: 999–1005,
and A1 adenosine receptor binding. J. Exp. Pharmacol. Exp.Ther. 266: 1563–1572, 1993.
32. Van Soeren, M. H., P. Sathasivam, L. L. Spriet, and T. E.
25. Lopes, J. M., M. Aubier, J. Jardim, J. V. Aranda, and P. T. Graham. Caffeine metabolism and epinephrine responses dur- Macklem. Effect of caffeine on skeletal muscle function before
ing exercise in users and nonusers. J. Appl. Physiol. 75: 805–812,
and after fatigue. J. Appl. Physiol. 54: 1303–1305, 1983.
26. Miles, J., R. Glasscock, J. Aitkens, J. Gerich, and M. A.
33. Vistisen, K., H. E. Poulsen, and S. Loft. Foreign compound Haymond. A microfluorometric method for the determination of
metabolism capacity in man measured from metabolites of
FFA in plasma. J. Lipid Res. 24: 96–99, 1983.
dietary caffeine. Carcinogenesis 13: 1561–1568, 1992.
27. Robertson, D., D. Wade, R. Workman, R. L. Woosley, and
34. Weiker, H., M. Feraudi, H. Hagele, and R. Pluto. Electro- J. A. Oates. Tolerance to the humoral and hemodynamic effects
chemical determination of catecholamines in urine and plasma
of caffeine in man. J. Clin. Invest. 67: 1111–1117, 1981.
separations with HPLC. Clin. Chim. Acta 141: 17–25, 1984.
Nuclear Instruments and Methods in Physics Research B 188 (2002) 78–83Study of the irradiation damage in SiC by ion channelingM. Kokkoris a,*, S. Kossionides a, A. Kyriakis a, K. Zachariadou a,G. Fanourakis a, R. Vlastou b, Th. Paradellis aa Laboratory for Material Analysis, Institute of Nuclear Physics, NCSR ‘Demokritos’, GR-153 10 Aghia Paraskevi, Athens, Greeceb Department of Phy
Science, medicine, and the future New pacing technologies for heart failure Anthony W C Chow, Rebecca E Lane, Martin R Cowie Heart failure is a sizeable problem in elderly populations, and although pharmacological treatmenthas improved, outcome generally remains poor. New pacing technologies have been developed totreat heart failure, with promising resultsThe prevalence of heart failure in t
 Effect of caffeine on metabolism, exercise endurance,and catecholamine responses after withdrawal
M. H. VAN SOEREN1 AND T. E. GRAHAM21School of Nursing, Faculty of Health Sciences, University of Western Ontario, London,Ontario N6A 5C1; and 2Human Biology and Nutritional Sciences, University of Guelph,Guelph, Ontario, Canada N1G 2W1
Van Soeren, M. H., and T. E. Graham. Effect of caffeine
Effect of caffeine on metabolism, exercise endurance,and catecholamine responses after withdrawal
M. H. VAN SOEREN1 AND T. E. GRAHAM21School of Nursing, Faculty of Health Sciences, University of Western Ontario, London,Ontario N6A 5C1; and 2Human Biology and Nutritional Sciences, University of Guelph,Guelph, Ontario, Canada N1G 2W1
Van Soeren, M. H., and T. E. Graham. Effect of caffeine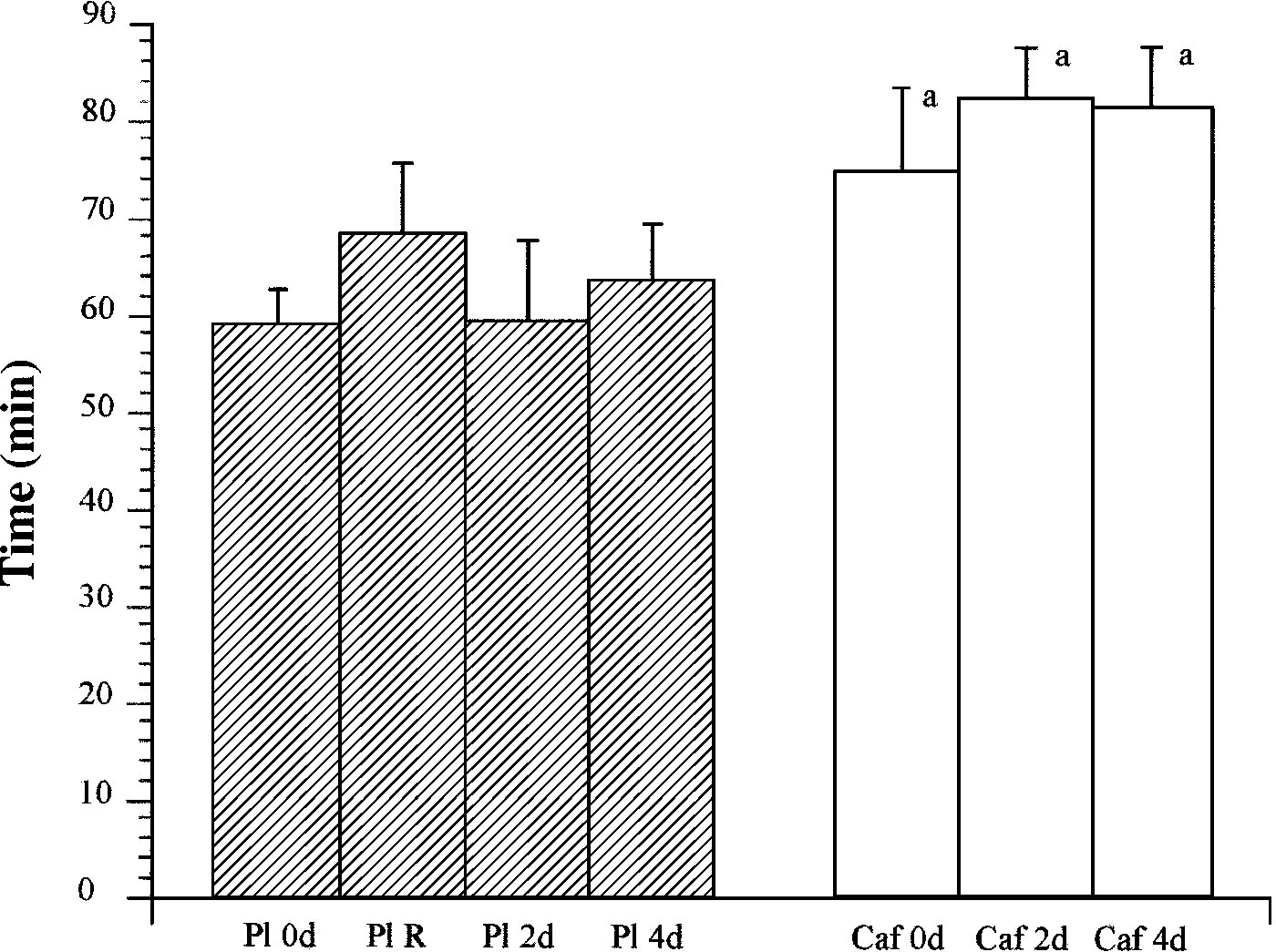 CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
FFAs (26) and glycerol (16). Plasma insulin was analyzed by
6.7 vs. 59.5 Ϯ 8.4 min), and the 4-day withdrawal
using 125I radioimmunoassay kit (Diagnostic Products Code-a-
(81.5 Ϯ 6.4 vs. 63.6 Ϯ 5.6 min). In contrast to the Pl 0d
Count Insulin kit). Diet analysis was completed as described
trial, the time to exhaustion in the Pl R trial was not
significantly different than in the Caf 0d trial. This
increase in time for the Pl R trial is heavily influencedby a single subject whose time increased from 70 to 124
Statistical analysis of respiratory, exercise, and blood data
min (Pl 0d vs. Pl R, respectively). When this subject’s
was conducted by using repeated-measures analysis of vari-
data are removed from the analyses, the Pl R and Caf
ance for drug and withdrawal. Bonferroni corrected t-tests
0d trials are significantly different, because all other
were used to adjust ␣ levels to limit the possibility of a type I
subjects performed similarly in both Pl trials.
CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
FFAs (26) and glycerol (16). Plasma insulin was analyzed by
6.7 vs. 59.5 Ϯ 8.4 min), and the 4-day withdrawal
using 125I radioimmunoassay kit (Diagnostic Products Code-a-
(81.5 Ϯ 6.4 vs. 63.6 Ϯ 5.6 min). In contrast to the Pl 0d
Count Insulin kit). Diet analysis was completed as described
trial, the time to exhaustion in the Pl R trial was not
significantly different than in the Caf 0d trial. This
increase in time for the Pl R trial is heavily influencedby a single subject whose time increased from 70 to 124
Statistical analysis of respiratory, exercise, and blood data
min (Pl 0d vs. Pl R, respectively). When this subject’s
was conducted by using repeated-measures analysis of vari-
data are removed from the analyses, the Pl R and Caf
ance for drug and withdrawal. Bonferroni corrected t-tests
0d trials are significantly different, because all other
were used to adjust ␣ levels to limit the possibility of a type I
subjects performed similarly in both Pl trials.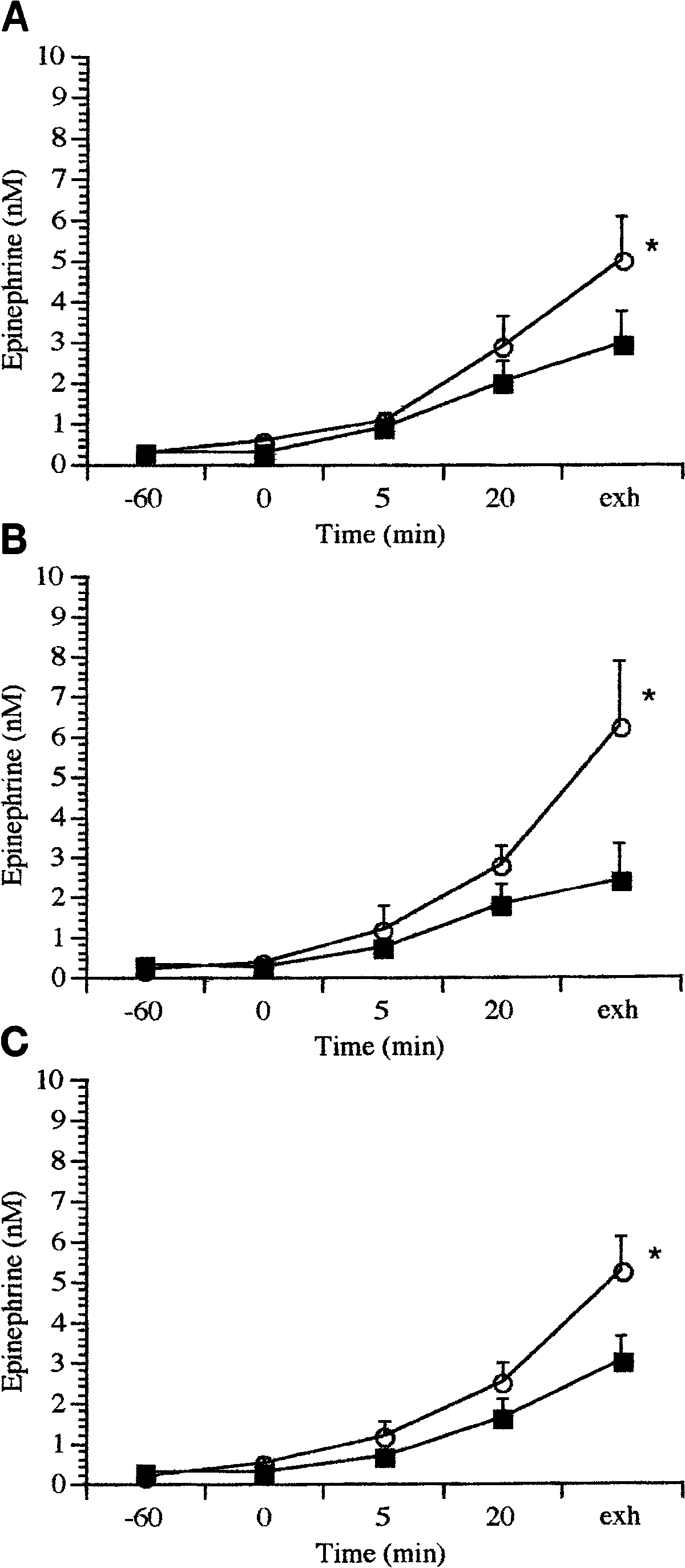
 CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
amounts of residual caffeine may be detected in plasma.
CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
amounts of residual caffeine may be detected in plasma.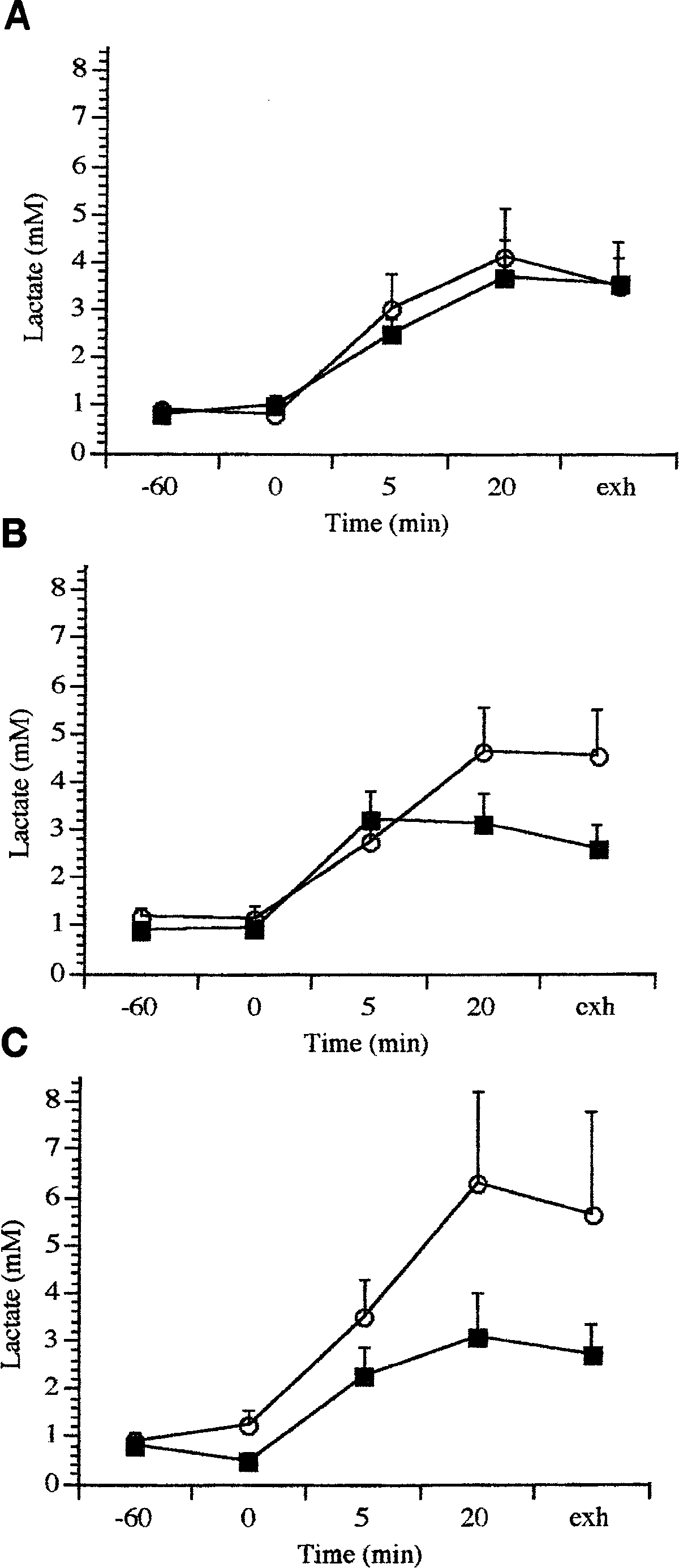 CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
Table 1. Serum free fatty acids and glycerol
0.22Ϯ0.04 0.45Ϯ0.12* 0.25Ϯ0.02 0.34Ϯ0.08 0.60Ϯ0.10
Values are means Ϯ SE given in mM for 6 subjects for placebo (Pl)
and caffeine (Caf) trials; 0d, no withdrawal; 2d, 2-day withdrawal; 4d,4-day withdrawal. Time points indicate before 4d ingestion (Ϫ60),after 1 h rest (0), after 5 and 20 min of exercise, and at exhaustion(Exh) when power output could no longer be maintained. FFA, freefatty acids. * Significantly different from Pl within same protocol,P Ͻ 0.05.
CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
Table 1. Serum free fatty acids and glycerol
0.22Ϯ0.04 0.45Ϯ0.12* 0.25Ϯ0.02 0.34Ϯ0.08 0.60Ϯ0.10
Values are means Ϯ SE given in mM for 6 subjects for placebo (Pl)
and caffeine (Caf) trials; 0d, no withdrawal; 2d, 2-day withdrawal; 4d,4-day withdrawal. Time points indicate before 4d ingestion (Ϫ60),after 1 h rest (0), after 5 and 20 min of exercise, and at exhaustion(Exh) when power output could no longer be maintained. FFA, freefatty acids. * Significantly different from Pl within same protocol,P Ͻ 0.05. CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
20. Griffiths, R. R., and P. P. Woodson. Caffeine physical depen-
CAFFEINE, WITHDRAWAL, AND EXERCISE METABOLISM
20. Griffiths, R. R., and P. P. Woodson. Caffeine physical depen-