Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Ukpubmedcentral.ac.uk
Science, medicine, and the future New pacing technologies for heart failure Anthony W C Chow, Rebecca E Lane, Martin R Cowie
Heart failure is a sizeable problem in elderly populations, and although pharmacological treatmenthas improved, outcome generally remains poor. New pacing technologies have been developed totreat heart failure, with promising results
The prevalence of heart failure in the general popula-
tion is estimated to be 1-2% and increases rapidly with
Summary box
age.1 In developed countries heart failure is a leading
cause of admission to hospital among elderly patients
New pacing technologies may now be used to
and accounts for 1-2% of healthcare expenditure.2
treat selected patients with heart failure
Although several pharmacological treatments have
improved outcome,3–5 the prognosis of patients with
Atrio-biventricular pacing has been shown to
pharmacological approaches including cardiac trans-
hospital in patients with left bundle branch block
plantation have been limited by availability of organs,
and the use of artificial left ventricular assist devices
The results of randomised trials powered to test
Recently, several promising new developments
mortality benefits from biventricular pacing will
have taken place in pacing technology to treat selected
patients with heart failure. These include atrio-
biventricular pacing to correct abnormal patterns of
Implantable defibrillators reduce mortality in
left ventricular contraction and implantable cardiac
survivors of sudden cardiac death and patients
defibrillators for treatment of malignant ventricular
with ventricular arrhythcardiac and poor left
arrhythmias. As the scale of the problem becomes
ventricular function; recent clinical trials show
apparent new treatments that have been shown to
that indications for the use of these devices will be
improve morbidity and possibly mortality in patients
with chronic heart failure will undoubtedly have a
major impact on clinical practice and healthcare
The use of combined implantable defibrillators
and atrio-biventricular pacemakers for patientswith heart failure is likely to increase—clear
indications for such devices are beginning toemerge
Sources and search criteria We systematically searched PubMed for publications on chronic heart failure and biventricular pacing,
in these patients.7 The prognosis for people with heart
cardiac resynchronisation, and implantable cardio-
failure remains poor. In clinical trials, death is most
verter defibrillators for the years 1985-2003.
commonly due to either malignant ventriculartachyarrhythmias or progressive pump failure. Popula-
The heart failure population
tion based studies report a mortality of close to 40%
In the developed world the underlying cardiac
within one year of diagnosis and around 10% per year
abnormality for most patients with heart failure is
thereafter.7 For patients who remain symptomatic at
impaired left ventricular systolic function due to
rest despite maximal medical treatment annual
ischaemic heart disease or idiopathic dilated cardiomy-
opathy.6 Despite maximal drug treatment manypatients still experience symptoms on minimal
Ventricular dyssynchrony
exertion or even at rest (New York Heart Association
An estimated 30% of patients with chronic heart fail-
class III-IV), and this functional limitation often has a
ure have evidence of abnormal interventricular
marked impact on their quality of life. Recurrent and
conduction on the 12 lead electrocardiogram, most
prolonged hospital admissions for periods of decom-
often in the form of left bundle branch block. The
pensation of the heart failure syndrome are common
resultant abnormal activation of the myocardium
BMJ VOLUME 326 17 MAY 2003
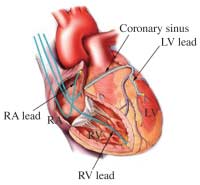
activation. With a greater understanding of the conse-quences of deranged ventricular conduction came theproposal of using more sophisticated pacing configu-rations in an attempt to correct or normalise electricalactivation and improve cardiac performance. This hasevolved to form the basis of the concepts for cardiacresynchronisation. Cardiac resynchronisation Cardiac resynchronisation or biventricular pacing entails inserting pacing leads via the cephalic or subclavian veins into the right atrium and right ventri- cle, as in conventional dual chamber permanent pacing. In addition, however, a third pacing lead is used to pace the left ventricle. In early studies this was achieved by performing a thoracoscopic procedure with placement of the electrode on the epicardial left ventricular free wall.11 12 This necessitated general anaesthesia and therefore carried appreciable risk in a Fig 1 The anterior walls of the right atrium and ventricle have been removed to show the lead arrangements used in biventricular pacing.
high risk group of patients. In 1998 Daubert et al pub-
Tributaries that drain the left ventricle form the coronary sinus,
lished the results of a study of a fully transvenous per-
which opens posteriorly into the right atrium. The left ventricular
manent biventricular pacing system,13 which revolu-
lead shown is positioned in the antero-lateral cardiac vein, with
tionised the technique (fig 1). Specially designed
conventional pacing leads in the right atrial appendage and rightventricular apex (RA=right atrium; RV=right ventricle; LV=left
catheters are inserted through the subclavian vein and
ventricle). Used with permission from the authors (AWCC)
passed down into the right atrium, from where the leftventricular coronary venous circulation can beaccessed. The coronary venous system consists of a
causes deranged ventricular contraction or dyssyn-
series of tributaries overlying the ventricular myocar-
chrony, with regions of early and late contraction.
dium. They drain into the coronary sinus that opens
Typically, the interventricular septum contracts early
into the right atrium. This network of coronary venous
relative to the delayed contraction of the lateral free
branches can be visualised by performing a coronary
wall of the left ventricle. In its most severe form
sinus venogram (fig 2) and used to guide the
dyssynchrony can result in contraction of the septum
placement of the left ventricular pacing lead. The
while the lateral wall is relaxing and vice versa. If
three pacing electrodes are then connected to the
opposing ventricular walls fail to contract together, a
artificial pacemaker to allow biventricular pacing
sizeable proportion of blood is simply shifted in the
ventricular cavity instead of being ejected into thecirculation, thereby reducing cardiac output. The pro-
Effects of biventricular pacing
portion of the cardiac cycle available for left ventricu-
Biventricular pacing aims to restore synchronous
lar filling and ejection is reduced by dyssynchronous
cardiac contraction. Studies have shown that when
contraction, which further contributes to a decrease in
ventricular dyssynchrony is reduced the heart is able to
the pumping ability of the heart. Even in structurally
contract more efficiently and increase left ventricular
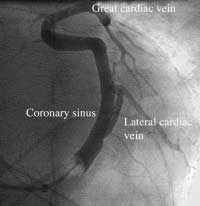
normal hearts the presence of left bundle branchblock impairs cardiac ejection fraction. In patientswith chronic heart failure and poor systolic functionventricular dyssynchrony further compromises car-diac performance and may exacerbate symptoms ofheart failure. Pacing for the treatment of heart failure Permanent pacing has been used for many years to treat symptomatic bradycardia and may alleviate heart failure when associated with heart block. Several stud- ies have examined the use of conventional dual cham- ber atrio-right ventricular pacing for the treatment of heart failure, in the absence of symptomatic bradycar- dia or heart block, in an attempt to enhance cardiac performance, but results have been inconsistent.9 10 In most studies, right ventricular pacing produced no haemodynamic benefit or had detrimental effects on left ventricular function. This probably reflects the fact that right ventricular apical pacing (which creates a left bundle branch block pattern) induces ventricular dyssynchrony, with detrimental effects on overall Fig 2 Coronary sinus venogram taken with a veno-occlusive balloon
pump function of the heart. Many centres now
(V) inflated. Left ventricular tributaries from the great cardiac vein
advocate pacing from the right ventricular septum to
and a lateral cardiac vein are shown draining into the coronary sinus.
provide a more physiological pattern of ventricular
Used with permission from the authors (AWCC)
BMJ VOLUME 326 17 MAY 2003
reduced by 50% in the group receiving biventricularpacing, and a staggering 77% reduction of total hospi-tal days saved for treating heart failure was observed inthe paced group compared with the control group. Asthe clinical trial lasted only six months it is still uncer-tain whether the benefits of biventricular pacing will besustained or increased with a longer period of followup. Thus the benefits seen with biventricular pacing notonly seem to improve the quality of life for individualpatients but also indicate that important andsubstantial economic savings may arise from using thistechnology.
As yet no definitive published data are available on
the effects of biventricular pacing on mortality, but sev-eral studies with end points of cardiac and all cause
Fig 3 Fluoroscopy showing final lead positions of an atrio-biventricular implantable cardiac defibrillator in an
mortality remain in progress.17 18 The cardiac resyn-
antero-posterior projection (RA=right atrial lead; RV ICD=right
chronisation in heart failure (CARE-HF) study has
ventricular implantable defibrillator lead; LV=left ventricular coronary
recently completed recruitment of patients, whereas
sinus lead). Used with permission from the authors (AWCC)
the preliminary findings of the comparison of medicaltreatment, pacing, and defibrillation in chronic heart
ejection fraction and cardiac output while working less
failure (COMPANION) study, which randomised over
and consuming less oxygen.14 In addition, reintroduc-
1600 patients to medical treatment alone, to biven-
ing left ventricular synchrony can increase left
tricular pacing, and to biventricular implantable
ventricular filling times, decrease pressure on the
cardiac defibrillators have been announced. This study
pulmonary capillary wedge, and reduce mitral regurgi-
was halted prematurely because of a 20% reduction in
tation (box 1). More advanced devices now enable
all cause mortality and all cause admissions to hospital
manipulation of both atrioventricular and interven-
in the groups receiving biventricular pacing. The most
tricular pacing intervals and the potential to further
notable benefits were seen in the arm of the study in
optimise individual haemodynamic and functional
which patients received biventricular implantable
cardiac defibrillators, where a 40% reduction of allcause mortality was achieved. Publication of the full
Clinical trials of biventricular pacing
report is eagerly awaited, but these preliminary data
Clinical trials have shown that biventricular pacing is
indicate that biventricular pacing may confer impor-
effective in the treatment of heart failure patients with
left bundle branch block (table). Several randomisedcontrolled clinical trials have compared biventricularpacing with medical treatment on its own. Both themultisite stimulation in cardiomyopathies (MUSTIC)
Box 2: Who should be considered for
and the multicentre insync randomised clinical evalua-
biventricular pacing
tion (MIRACLE) studies, which enrolled 68 and 524
heart failure patients, respectively, in a randomised
crossover trial of biventricular pacing showed signifi-
• Highly symptomatic (New York Heart Association
cant improvements in quality of life scores, exercise
tolerance, New York Heart Association functional class,
peak oxygen uptake, and cardiac ejection fraction
during biventricular pacing.15 16 What was particularly
Left bundle branch block wide QRS >130 ms/echo assessment
impressive was the reduction in admissions to hospital
Induced by right ventricular apical pacing
for worsening heart failure seen in the MIRACLE
study. At six months the relative risk of decompensated
heart failure requiring admission to hospital was
Limitations and complications of biventricular Box 1: Haemodynamic effects of biventricular
The electrocardiogram is used as the screening tool for
• Increased left ventricular ejection fraction and
predicting ventricular dyssynchrony and hence suit-
ability for biventricular pacing. Up to 20% of patients
fulfil the criteria for biventricular pacing (box 2), yet
• Prolonged diastole and left ventricular filling time
derive little or no clinical benefit from resynchronisa-
• Reduced left ventricular end diastolic and end
tion.19 In the future, more sensitive and specific
non-invasive screening tests will be required to
• Increased left ventricular synchrony and pulse
improve the selection of patients. This will probably be
in the form of echocardiography guided techniques
such as tissue Doppler echocardiography, which facili-
• Decreased pulmonary capillary wedge pressure
tates the quantification of dyssynchrony20 and thus
may provide more accurate prediction of a favourableclinical response with biventricular pacing. BMJ VOLUME 326 17 MAY 2003
Clinical trials of atrio-biventricular pacing
No of patients randomised Inclusion criteria End points
Increased*(Similar benefits seen withCRT and univentricular (LV)stimulation)
Left ventricular ejection fraction <35%
owing to survival benefits withcardiac resynchronisation andICD arms. Full results expected 2003
New York Heart Association scoreQuality of life scoreNeurohormonal
In all trials, patients were having optimal medical treatment; outcomes were compared with baseline. *P<0.05.
Even with improvements in delivery systems and
Implantable cardioverter defibrillators
pacing lead technology the site of left ventricular
Severe left ventricular dysfunction is now known to be
pacing is often limited by the individual’s coronary
an independent predictor of cardiac mortality. Death is
venous anatomy. Implantation of ventricular pace-
usually attributable to progressive heart failure or the
makers can be technically challenging and is associated
development of malignant ventricular arrhythmias.
with small risks. Inability to deploy the left ventricular
Several large randomised controlled trials have found
lead accounts for most of the 8% reported implant fail-
a sizeable reduction in mortality among patients with
ures.16 Commonly encountered complications over
ischaemic heart disease, impaired left ventricular func-
and above those associated with any permanent pace-
tion, and failed sudden death or evidence of ventricular
maker insertion are usually related to the insertion of
arrhythmias who had an implantable cardiac defibrilla-
the left ventricular lead. These include inability to
tor compared with patients treated with antiarrhythmic
intubate the coronary sinus or a venous tributary,
drugs.21 22 This compelling evidence has formed the
dissection of the coronary sinus, displacement of the
basis for guidance from the National Institute for
left ventricular lead, and diaphragmatic stimulation
Clinical Evidence (NICE) on widespread use of these
(box 3). Complications are largely minimised by the
devices in individuals at high risk.23 The role of
operator’s experience, meticulous technique, stringent
implantable cardiac defibrillators in patients with non-
testing at implantation, and careful programming of
ischaemic cardiomyopathy is less certain but should be
addressed by the ongoing sudden cardiac death inheart failure trial, which includes patients with bothischaemic and non-ischaemic cardiomyopathy. In the
Box 3: Limitations of the technique
most recently published multicentre automatic defi-
• Selection of patients and prediction of patients’
brillator implantation II (MADIT II) trial,24 no formal
assessment of arrhythmic risk was required; the
inclusion criteria were based on the presence of
ischaemic heart disease and poor left ventricular
function alone. The trial was stopped early because of
a relative risk reduction of 31% in all cause mortality
seen in the group treated with implantable cardiac
defibrillators compared with controls over a 20 month
follow up period. The implications of this trial
alone may expand the recommended indications forimplantation of these devices in the future. BMJ VOLUME 326 17 MAY 2003
Pitt B, Zannad F, Remme WJ, Cody R, Castaigne A, Perez A, et al. Theeffect of spironolactone on morbidity and mortality in patients with
Additional educational resources
severe heart failure. Randomized Aldactone Evaluation Study Investiga-tors. N Engl J Med 1999;341:709-17.
• The website of the North American Society of
Cowie MR, Fox KF, Wood DA, Metcalfe C, Thompson SG, Coats AJ, et al.
Pacing and Electrophysiology (www.naspe.org) gives
Hospitalization of patients with heart failure: a population-based study. Eur Heart J 2002;23:877-85.
useful general information on recent developments
Cowie MR, Wood DA, Coats AJ, Thompson SG, Suresh V, Poole-Wilson
and current guidelines for heart failure devices
PA, et al. Survival of patients with a new diagnosis of heart failure: a
• www.docguide.com is a general website citing recent
population based study. Heart 2000;83:505-10.
Cohn JN, Johnson GR, Shabetai R, Loeb H, Tristani F, Rector T, et al.
literature, which has several links for cardiac
Ejection fraction, peak exercise oxygen consumption, cardiothoracic
ratio, ventricular arrhythmias, and plasma norepinephrine as determi-
• The official website of the National Institute for
nants of prognosis in heart failure. The V-HeFT VA Cooperative StudiesGroup. Circulation 1993;87:VI5-16.
Clinical Excellence (www.nice.org) provides full and
Hochleitner M, Hortnagl H, Ng CK, Hortnagl H, Gschnitzer F, Zechmann
abbreviated guidelines for the use of implantable
W. Usefulness of physiologic dual-chamber pacing in drug-resistant idio-
pathic dilated cardiomyopathy. Am J Cardiol 1990;66:198-202.
10 Linde C, Gadler F, Edner M, Nordlander R, Rosenqvist M, Ryden L.
• www.medtronic.com/physician/cardiology.html is an
Results of atrioventricular synchronous pacing with optimized delay in
extensive website of a major device company, with
patients with severe congestive heart failure. Am J Cardiol 1995;75:919-
sections for doctors and patients, and covers all aspects
11 Cazeau S, Ritter P, Lazarus A, Gras D, Backdach H, Mundler O, et al.
of current pacing technologies used for heart failure
Multisite pacing for end-stage heart failure: early experience. Pacing ClinElectrophysiol 1996;19:1748-57.
12 Auricchio A, Stellbrink C, Block M, Sack S, Vogt J, Bakker P, et al. Effect of
pacing chamber and atrioventricular delay on acute systolic function ofpaced patients with congestive heart failure. The Pacing Therapies for
In the light of trials showing a reduction in
Congestive Heart Failure Study Group. The Guidant Congestive Heart
mortality with implantable cardiac defibrillators and
Failure Research Group. Circulation 1999;99:2993-3001.
13 Daubert JC, Ritter P, Le Breton H, Gras D, Leclercq C, Lazarus A, et al.
improvement in left ventricular function with biven-
Permanent left ventricular pacing with transvenous leads inserted into
tricular pacing in patients with heart failure it seems
the coronary veins. Pacing Clin Electrophysiol 1998;21:239-45.
14 Nelson GS, Berger RD, Fetics BJ, Talbot M, Spinelli JC, Hare JM, et al. Left
logical that combined biventricular pacing and
ventricular or biventricular pacing improves cardiac function at
implantable cardiac defibrillators devices may be com-
diminished energy cost in patients with dilated cardiomyopathy and leftbundle-branch block. Circulation 2000;102:3053-9.
plementary in selected patients. The early indications
15 Cazeau S, Leclercq C, Lavergne T, Walker S, Varma C, Linde C, et al.
from the COMPANION trial support this theory, with
Effects of multisite biventricular pacing in patients with heart failure andintraventricular conduction delay. N Engl J Med 2001;344:873-80.
the greatest reduction in mortality observed with com-
16 Abraham WT, Fisher WG, Smith AL, Delurgio DB, Leon AR, Loh E, et al.
bined devices. Although final reports are yet to be pub-
Cardiac resynchronization in chronic heart failure. N Engl J Med2002;346:1845-53.
lished on prospective trials incorporating combined
17 Bristow MR, Feldman AM, Saxon LA. Heart failure management using
biventricular pacing and implantable cardiac defibrilla-
implantable devices for ventricular resynchronization: comparison of
tors devices, the use of combined devices to provide
medical therapy, pacing, and defibrillation in chronic heart failure(COMPANION) trial. COMPANION Steering Committee and COM-
both cardiac resynchronisation with defibrillation are
PANION Clinical Investigators. J Card Fail 2000;6:276-85.
18 Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D,
Kappenberger L, et al. The CARE-HF study (CArdiac REsynchronisationin Heart Failure study): rationale, design and end-points. Eur J Heart Fail2001;3:481-9.
19 Reuter S, Garrigue S, Barold SS, Jais P, Hocini M, Haissaguerre M, et al. Conclusion
Comparison of characteristics in responders versus nonresponders withbiventricular pacing for drug-resistant congestive heart failure. Am J Car-
Evidence is now compelling that pacing technologies
20 Yu CM, Lin H, Zhang Q, Sanderson JE. High prevalence of left ventricu-
can improve morbidity and mortality in patients with
lar systolic and diastolic asynchrony in patients with congestive heart fail-
heart failure. The indication for using these devices is
ure and normal QRS duration. Heart 2003;89:54-60.
21 The AVID Investigators. A comparison of antiarrhythmic drug therapy
likely to expand in the future. Clinicians at all levels
with implantable defibrillators in patients resuscitated from near fatal
should have a fundamental knowledge of the
ventricular arrhythmias. N Engl J Med 1997;337:1576-83.
indications and function of these devices. The growth
22 Moss AJ, Jackson-Hall W, Cannom DS, Daubert JP, Higgins SL, Klein H,
et al. Improved survival with an implanted defibrillator in patients with
in these technologies will also have serious economic
coronary disease at high risk for ventricular arrhythmia. N Engl J Med
implications for those planning and delivering health
23 National Institute for Clinical Excellence. Guidance on the use of implantablecardioverter defibrillators for arrhythmias. Technology appraisal guidance 11. London: NICE, 2000.
24 Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, et al. Pro-
Competing interests: AWCC has received reimbursement from
phylactic implantation of a defibrillator in patients with myocardial
many companies for attending conferences. REL receives a
infarction and reduced ejection fraction. N Engl J Med 2002;346:877-83.
research fellowship from Medtronic Inc and has received reim-
bursement from many companies for attenting conferences. MRC is the clinical adviser for the national clinical guidelines onthe management of heart failure, commissioned by the National
Institute for Clinical Excellence, but the opinions in this revieware his own and will not necessarily reflect those in theforthcoming guideline. MRC has received honorariums for
Human dignity
advisory boards and lectures related to treatments mentioned in
Among other living things, it is man’s dignity to
value certain ideals above comfort, and even abovelife. This human trait makes of medicine aphilosophy that goes beyond exact medical
Cowie MR, Mosterd A, Wood DA, Deckers JW, Poole-Wilson PA, SuttonGC, et al. The epidemiology of heart failure. Eur Heart J 1997;18:208-25.
sciences, because it must encompass not only man
Berry C, Murdoch DR, McMurray JJ. Economics of chronic heart failure.
as a living machine but also the collective
Eur J Heart Fail 2001;3:283-91.
Kjekshus J, Swedberg K, Snapinn S. Effects of enalapril on long-termmortality in severe congestive heart failure. CONSENSUS Trial Group.
René Jules Dubos (1901-81), French/American
microbiologist, in Mirage of Health
Packer M, Fowler MB, Roecker EB, Coats AJ, Katus HA, Krum H, et al. Effect of carvedilol on the morbidity of patients with severe chronic heart
Robert Richardson, medical historian, Chichester
failure: results of the carvedilol prospective randomized cumulativesurvival (COPERNICUS) study. Circulation 2002;106:2194-9. BMJ VOLUME 326 17 MAY 2003
Diário da República, 2.ª série — N.º 114 — 15 de Junho de 2007do disposto no artigo 241.º da Constituição da República Portuguesa,do artigo 64.º, n.º 7, alínea a) da Lei n.º 169/99, de 18 de Setembroe do artigo 55.º da Lei n.º 2/2007, de 15 de Janeiro. O RTEDUL tem por objectivo o ordenamento da utilização da viapública, quer na circulação, quer no parqueamento de veíc
Clinical Infectious Diseases Advance Access published September 9, 2012 Clinical Practice Guideline for the Diagnosisand Management of Group A StreptococcalPharyngitis: 2012 Update by the InfectiousDiseases Society of AmericaaStanford T. Shulman,1 Alan L. Bisno,2 Herbert W. Clegg,3 Michael A. Gerber,4 Edward L. Kaplan,5 Grace Lee,6Judith M. Martin,7 and Chris Van Beneden81Department of Pediat
 activation. With a greater understanding of the conse-quences of deranged ventricular conduction came theproposal of using more sophisticated pacing configu-rations in an attempt to correct or normalise electricalactivation and improve cardiac performance. This hasevolved to form the basis of the concepts for cardiacresynchronisation.
activation. With a greater understanding of the conse-quences of deranged ventricular conduction came theproposal of using more sophisticated pacing configu-rations in an attempt to correct or normalise electricalactivation and improve cardiac performance. This hasevolved to form the basis of the concepts for cardiacresynchronisation.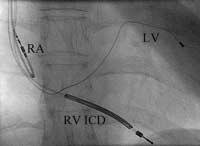 reduced by 50% in the group receiving biventricularpacing, and a staggering 77% reduction of total hospi-tal days saved for treating heart failure was observed inthe paced group compared with the control group. Asthe clinical trial lasted only six months it is still uncer-tain whether the benefits of biventricular pacing will besustained or increased with a longer period of followup. Thus the benefits seen with biventricular pacing notonly seem to improve the quality of life for individualpatients but also indicate that important andsubstantial economic savings may arise from using thistechnology.
reduced by 50% in the group receiving biventricularpacing, and a staggering 77% reduction of total hospi-tal days saved for treating heart failure was observed inthe paced group compared with the control group. Asthe clinical trial lasted only six months it is still uncer-tain whether the benefits of biventricular pacing will besustained or increased with a longer period of followup. Thus the benefits seen with biventricular pacing notonly seem to improve the quality of life for individualpatients but also indicate that important andsubstantial economic savings may arise from using thistechnology.