Relative bioavailability of topiramate administered rectally
Jeannine M. Conway , Angela K. Birnbaum , Robert L Kriel , James C. Cloyd
a Experimental and Clinical Pharmacology, Epilepsy Research and Education Program, College of Pharmacy,University of Minnesota, 7-170 WDH 308 Harvard St. SE, Minneapolis, MN 55455, USA
b Departments of Pediatrics and Neurology, Hennepin County Medical Center, Minneapolis, MN, USA
Received 18 October 2002; received in revised form 12 March 2003; accepted 18 March 2003
Abstract Objective: To determine the relative bioavailability and tolerability of a topiramate (TPM) suspension after rectal administra-
Design/method: Seven healthy men and five healthy non-pregnant women were enrolled. A 100 or 200 mg tablet of TPM was
given orally and a 200 mg dose was given rectally in a randomized, open-label, crossover study with at least a 2-week washoutperiod between doses. Plasma samples were collected prior to dosing and the following times after each dose: 0.5, 1, 1.5, 2, 3,4, 6, 8, 12, 16, 24, 48, 72, and 96 h. Relative bioavailability was determined by calculating the ratio of the dose-normalized areaunder the curve (AUC/D) for the rectal and oral doses. Results: Ten subjects completed the study. Two of the first seven subjects who received a 200 mg initial oral dose, withdrew
because of side effects. The remaining subjects received a 100 mg oral dose. Three subjects received a 200 mg dose orally andrectally, and seven subjects received 100 mg orally and 200 mg rectally. The average AUC/D was 0.72±0.18 h/l for the rectal doseand 0.76 ± 0.20 h/l for the oral dose. The relative bioavailability (n = 10) for TPM administered rectally was 0.95 ± 0.17 witha range of 0.68–1.2. There were no statistically significant differences between the oral or rectal pharmacokinetic parameters. Conclusions: In healthy adults, rectally administered TPM is absorbed to a similar extent as the oral dosage form. Rectal
administration is an acceptable route of administration for TPM, when the oral route is temporarily unavailable. 2003 Elsevier Science B.V. All rights reserved. Keywords: Topiramate; Rectal administration; Bioavailability
1. Introduction
seizures (Although noncom-pliance is the most common reason for interruptions
A common cause of seizure breakthrough is
of oral therapy, there are a variety of other reasons
interruption in antiepileptic drug (AED) therapy
such as vomiting, gastrointestinal illness, fasting prior
to and after surgery, and impairment of conscious-
catastrophic effects on a patient’s seizure control, in-
ness that may result in a precipitous decrease in AED
cluding increased frequency, intensity, or duration of
Alternatives to oral AED therapy are limited.
Among all the AEDs only three are available as
Corresponding author. Tel.: +1-612-625-2999;
parenteral formulations: phenobarbital, phenytoin,
E-mail address: [email protected] (J.M. Conway).
and sodium valproate. This leaves many patients
0920-1211/03/$ – see front matter 2003 Elsevier Science B.V. All rights reserved. doi:10.1016/S0920-1211(03)00083-4
J.M. Conway et al. / Epilepsy Research 54 (2003) 91–96
and clinicians with the dilemma of using a different
suspension in a volume ≤20 ml. TPM is also lipophilic
AED based on availability of a parenteral solution.
enough (log P = 0.573) to facilitate relatively rapid
Such circumstances expose the patient to both unpre-
dictable side effects and the potential loss of seizure
control. Even when a parenteral formulation is avail-
The objective of this study was to determine the
able, administration requires the presence of skilled
relative bioavailability and tolerability of TPM sus-
medical personnel in a healthcare facility with all
pension after rectal administration using a formulation
the attendant costs and inconveniences. The preferred
that is easily prepared from commercially available
approach would be to maintain the patient on her or
tablets. Information on the absorption and safety of
his current medication by using an alternate route of
rectal administration of TPM can guide the practi-
tioner when oral administration is not possible.
Rectal administration may be used as a bridge when
oral AED therapy is not possible and a parenteralformulation does not exist or is impractical. An ac-
2. Methods
ceptable alternative to the oral route may be rectaladministration if the drug is adequately and consis-
tently absorbed, and the formulation is well tolerated. Many AEDs possess physical–chemical characteris-
The subject population was healthy volunteers from
tics that make them candidates for rectal administra-
18 to 65 years of age. Subjects were excluded from the
study if they had a previous history of nephrolithiasis,
were not in good health, were taking other medica-
were unwilling or unable to receive medications
rectally, were unwilling or unable to tolerate multi-
ple venipunctures, or had a hemoglobin <12 g/dl. The
study was approved by the IRB’s at both the Univer-
These studies demonstrate that it is possible to take
sity of Minnesota (Minneapolis, MN) and Hennepin
commercially available oral formulations and, with a
County Medical Center (Minneapolis, MN). Subjects
few simple steps that can be done in the pharmacy or
were informed of the study and gave written consent.
For each phase of the study, subjects were admitted
Topiramate (TPM) is an AED approved for use
to the DaVita Clinical Research Unit (CRU) located
as adjunctive therapy for partial onset seizures or
at Hennepin County Medical Center, where they re-
primary generalized tonic clonic seizures in children
mained for approximately 24 h. A 100 or 200 mg
(ages 2–16) years and adults. It is also indicated as
tablet of TPM was given orally or a 200 mg dose was
adjunctive therapy for children 2 years of age or older
given rectally in a randomized, open-label, crossover
with seizures due to Lennox–Gastaut syndrome. TPM
study with at least a 2-week washout period between
is available only as oral formulations: 25, 100, and
doses. The original study design was for each subject
200 mg tablets or 15 and 25 mg sprinkle capsules. It
to receive a 200 mg oral dose; however, two of the
has multiple mechanisms of action that work for many
subjects that received a 200 mg oral dose withdrew
from the study due to adverse events. Hence, the
suggests, it is useful for childhood epilepsies including
remaining subjects received a 100 mg oral dose. For
the oral dose, the subject swallowed either the com-
mercially available 100 or 200 mg tablet with 120 ml
of water. The 200 mg dose was selected based on
the predicted concentrations that would be seen in
TPM would appear to be a viable candidate
humans following a single dose and the sensitivity of
for rectal administration. Its chemical–physical prop-
erties indicate that it is sufficiently soluble in water
The rectal dose was prepared by crushing a 200 mg
(9.8 mg/ml) to deliver a clinically relevant dose as a
tablet with a mortar and pestle, and adding 10 ml of
J.M. Conway et al. / Epilepsy Research 54 (2003) 91–96
tap water to suspend the material. The contents of the
gation. The eluate was evaporated to dryness under
mixture were then drawn into a 35 ml syringe and the
nitrogen and the final samples were reconstituted with
mortar was rinsed with 5 ml of water twice and then
100 l of toluene. A 2 l sample was injected on to
drawn into the syringe after each rinse. The syringe
the column and quantified by GC-MS in the SIM
was inverted 10 times to mix the contents. The sub-
mode. The GC-MS system consisted of a HP5890
jects were placed in the right lateral decubitus position
Series II Gas Chromatograph; HP5971 Mass Selec-
and the 35 ml syringe with an attached catheter was in-
tive Detector; HP7673 Autoinjector; using a DB-5MS
serted approximately 2.5 in. into the rectum. The sub-
30 m ×0.25 mm i.d. capillary of 0.5 m film thickness
jects rested in a supine position for at least 60 min and
column (J&W Scientific, Folsom, CA). The program
were monitored to ensure that rectal expulsion did not
for sample analysis was an injection volume of 2 l,
transfer line temperature of 280 ◦C, initial tempera-
Plasma samples were collected just prior to and
ture of 230 ◦C, initial time of 0.5 min, program rate
at the following times after each dose: 0.5, 1, 1.5, 2,
was 10 ◦C/min, final temperature of 290 ◦C, final time
3, 4, 6, 8, 12, 16, 24, 48, 72, and 96 h. Blood sam-
of 1.0 min, and detector temperature of 300 ◦C. Ions
ples were centrifuged and plasma was transferred to
monitored were 193.1 and 324.1 mz. The peak times
a separate container for storage at −80 ◦C. Adverse
were 4.5 min (TPM) and 5.4 min (I.S.).
event data were collected, as a self-report, at each
Each subject’s oral and rectal blood samples were
blood sample collection. The scale was designed to
extracted and analyzed on the same day and compared
measure the level of comfort of the side effects that
on the same standard curve. Triplicate quality con-
were thought to be the most likely to occur: speech
trol samples were run with plasma samples and were
impairment, dizziness, nausea, headache, difficulties
deemed acceptable if the values were within two stan-
in concentrating, sleepiness, unusual sensations, dis-
dard deviations of the mean quality control values for
comfort due to administration of the rectal dose, and
all previous runs. The solubility of the suspension was
abnormal vision. Severity of adverse events was rated
determined by preparing the rectal dose, as described
on a scale from 0 to 5, with 0 indicating no notice-
above, and filtering the suspension. Unextracted trip-
able adverse event and 5, a severe adverse event. Side
licate samples and standard curves were analyzed by
effects and discomfort associated with oral and rec-
tal administration were assessed. Subjects were alsoasked to report adverse events not specifically listed. 4. Pharmacokinetic analyses 3. Sample analysis
All pharmacokinetic analyses were completed with
WinNonlin version 3.1 (Pharsight, Mountain View,
TPM concentrations were determined by a GC-MS
CA) using a noncompartmental approach. The area
method that was modified from one described by
under the TPM plasma concentration time curve
was determined using the trapezoidal rule from time
laboratory. TPM reference standard was provided by
0 to 96 h (AUC0–96). The total AUC was calcu-
Johnson & Johnson Pharmaceutical Research and
lated by adding the AUC96–∞ (C96/kel) to AUC0–96.
Development (Raritan, NJ). For extraction, 50 l of
The elimination rate constant (kel) was determined
the internal standard, cyheptamide (Sigma, St. Louis,
by the log-linear regression analysis of the termi-
MO) and 500 l of saturated ammonium acetate were
nal plasma TPM concentration time points. Relative
added to 500 l of sample or standard. Samples were
bioavailability (Frel) was determined by calculating
vortexed and transferred to an EmporeTM (3M, St.
the ratio of the dose-normalized area under the con-
Paul, MN) C18 solid-phase extraction disk cartridge.
centration time curves (AUC0–∞/D) for the rectal
The disk was primed and the sample was forced
and oral doses using the following equation: Frel =
through the disk by centrifugation. The disk was then
(AUC0–∞,rectal/Drectal)/(AUC0–∞,oral/Doral). We as-
washed with water, hexane, and finally ethyl acetate
sumed linear pharmacokinetics for both the 100 and
was added and forced through the disk by centrifu-
J.M. Conway et al. / Epilepsy Research 54 (2003) 91–965. Statistical analysis
The mean and standard deviation were determined
for all pharmacokinetic parameters. ANOVA was usedto compare the oral to the rectal treatments (MircosoftExcel 2000). A P ≤ 0.05 was considered statisticallydifferent. Bioequivalence was determined using Win-Nonlin version 3.1 and the Westlake method. 6. Results
Fig. 1. Relative bioavailability of each subject. Each diamondrepresents an individual subject.
Ten of 12 subjects, who gave consent, completed
the study (Two of the first seven subjectswithdrew because of side effects following the ini-tial 200 mg oral dose. Because of the unacceptableadverse effects, the oral dose was reduced to 100 mgfor the remaining subjects. Three subjects received200 mg orally and rectally and seven subjects received100 mg orally and 200 mg rectally. Our laboratory de-termined the solubility of the rectal TPM formulationmade from the 200 mg tablet to be 2.78 mg/ml.
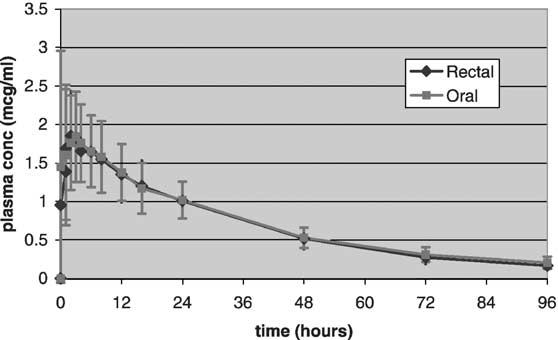
The average AUC0–∞/D for the rectal and oral
doses was 0.72 ± 0.18 h/l and 0.76 ± 0.20 h/l, respec-tively There were no statistical differencesbetween the pharmacokinetic parameters for the oral
Fig. 2. Average plasma concentrations (dose adjusted) vs. time.
and rectal doses. The relative bioavailability (n = 10)
Error bars signify one standard deviation of the mean.
for TPM administered rectally was 0.95 ± 0.17 with a
Subject characteristics for pharmacokinetic analysis (n = 10)
range of 0.68–1.2 The average dose adjusted
AUC0–∞ for 10 subjects is shown in Rectal
TPM bioavailability for 9 of 10 subjects fell within
a range of 80–120%. The 90% confidence interval
bounds for the least-squares mean ratio (rectal/oral)
from log transformed data was 81.9–118.
a Values divided by dose for statistical comparison. J.M. Conway et al. / Epilepsy Research 54 (2003) 91–96
Table 3Side effects vs. route: a comparison of the highest score reported by a subject at any time point the time it occurred
Side effects were rated from 0 (no discomfort) to 5 (severe discomfort).
The subjects that completed the study reported no
neither difference was statistically different. There
impairment of speech or discomfort due to adminis-
were no statistical differences between the routes
tration by either route. Dizziness, nausea, headache,
of administration or other pharmacokinetic param-
difficulties in concentrating, sleepiness, unusual sen-
eters including clearance, half-life, elimination rate
sations, and abnormal vision occurred regardless of
constant, or volume of distribution.
the route of dose delivery. If side effects were re-
The variability in rectal TPM bioavailability could
ported, they generally occurred between 1 and 4 h
be due to several factors. We found that the amount
following the dose, and resolved by 8 h regardless of
of a crushed 200 mg tablet that dissolves in water is
the route of medication. The two subjects (#4 and #7),
2.78 mg/ml. This is much lower than the predicted
who discontinued the study following the oral dose,
solubility of 9.8 mg/ml. Despite the solubility being
reported adverse events. The highest score subject #4
less than expected, it appears that an adequate amount
reported for any given side effect was 1, and the sub-
was absorbed rectally. Drug dissolution can be af-
ject withdrew following difficulty with motor skills
fected by the fineness of the particles, the presence
and cognitive function after the oral dose. Subject #7
of other excipient particulates, and water temperature
reported numerous side effects with a score up to 5
and withdrew from the study after reporting “trouble
of these factors varied when preparing each subject’s
in concentrating” during the entire week after the
rectal dose. Rectal doses with a high percentage of
oral dose. lists the medians and modes of
TPM in suspension, as opposed to solution, may have
the highest value, for the adverse events listed above,
resulted in lower bioavailability. The assumption of
reported by the subjects at any given time point.
linear pharmacokinetics between the 100 and 200 mgdoses was made for the bioavailability calculation. Ifthe pharmacokinetics of TPM is not linear between
7. Discussion
100 and 200 mg doses, the calculations may under-estimate or overestimate bioavailability. Nonetheless,
In healthy adults, rectally administered TPM sus-
rectal TPM displays high and relatively consistent ab-
pension is bioequivalent to the orally administered
sorption relative to other rectally administered AEDS
tablet. This study demonstrated a relative bioavailabil-
ity of 0.95 ± 0.17 for rectally administered TPM with
a 90% confidence interval of 81.9–118. The plasma
Our data suggest that a rectally administered
TPM concentrations attained by rectal administration
10 mg/ml suspension of a crushed TPM tablet may
tended to be lower and peak plasma concentration
be used when oral administration is not possible. Vol-
tended to occur later compared to the oral dose, but
ume considerations may limit the usefulness of this
J.M. Conway et al. / Epilepsy Research 54 (2003) 91–96
formulation if patients require dosages greater than
Cloyd, J.C., Kriel, R.L., 1981. Bioavailability of rectally
200 mg per dose. Alternatively, given the low solubil-
administered valproic acid syrup. Neurology 31 (10), 1348–
ity of the rectal formulation used in this study, it may
Cloyd, J.C., Lalonde, R.L., et al., 1998. A single-blind, crossover
be possible to achieve the same results with a more
comparison of the pharmacokinetics and cognitive effects of a
concentrated suspension. The plasma concentrations
new diazepam rectal gel with intravenous diazepam. Epilepsia
attained following rectal administration should be
sufficient when replacing a dose if a person cannot
Dhillon, S., Oxley, J., et al., 1982. Bioavailability of diazepam after
take their regular dose orally. The T
intravenous, oral and rectal administration in adult epileptic
patients. Br. J. Clin. Pharmacol. 13 (3), 427–432.
tion half-life indicate that rectal TPM can be given at
the same interval as oral TPM (once or twice daily).
pharmacokinetics and effect of food on the bioavailability
This information will help guide the clinician and
of topiramate, a novel antiepileptic drug. J. Clin. Pharmacol.
care givers about an alternate route of administration
Gidal, B.E., Lensmeyer, G.L., 1999. Therapeutic monitoring of
topiramate: evaluation of the saturable distribution between
This study was conducted in healthy adult vol-
erythrocytes and plasma of whole blood using an optimized
unteers. Further research is needed to determine if
high-pressure liquid chromatography method. Ther. Drug
rectal TPM administration can be used for more
extended periods of time in adult and pediatric pa-
Glauser, T.A., Clark, P.O., et al., 1998. A pilot study of topiramate
tients with epilepsy. Rectal administration may also
in the treatment of infantile spasms. Epilepsia 39 (12), 1324–1328.
be useful in situations where patients on TPM go
Graves, N.M., Kriel, R.L., et al., 1985. Relative bioavailability
into status epilepticus due to an abrupt decrease in
of rectally administered carbamazepine suspension in humans.
plasma concentrations (e.g. noncompliance, malab-
sorption, drug interactions, etc.). Until further in-
Graves, N.M., Holmes, G.B., et al., 1989. Relative bioavailability of
formation is available, dose substitution should be
rectally administered phenobarbital sodium parenteral solution. Dicp 23 (7/8), 565–568.
done carefully with close supervision by a healthcare
Johnson & Johnson Pharmaceutical Research Institute Topamax
(topiramate) Data on File. Raritian, NJ.
Kriel, R.L., Birnbaum, A.K., et al., 1997. Failure of absorption
of gabapentin after rectal administration. Epilepsia 38 (11),1242–1244. Acknowledgements
Krumholz, A., Grufferman, S., et al., 1989. Seizures and seizure
care in an emergency department. Epilepsia 30 (2), 175–181.
Grant funding supported by: USP Fellowship,
Matsukura, M., Higashi, A., et al., 1981. Bioavailability of
NINDS P50-NS16308, and Johnson & Johnson Phar-
phenobarbital by rectal administration. Pediatr. Pharmacol.
maceutical Research and Development.
Minagawa, K., Miura, H., et al., 1986. Pharmacokinetics of rectal
diazepam in the prevention of recurrent febrile convulsions. Brain Dev. 8 (1), 53–59. References
Remy, C., Jourdil, N., et al., 1992. Intrarectal diazepam in epileptic
adults. Epilepsia 33 (2), 353–358.
Birnbaum, A.K., Kriel, R.L., et al., 2000. Rectal absorption
Sachdeo, R.C., Glauser, T.A., et al., 1999. A double-blind,
of lamotrigine compressed tablets. Epilepsia 41 (7), 850–
randomized trial of topiramate in Lennox-Gastaut syndrome.
Topiramate YL Study Group. Neurology 52 (9), 1882–1887.
Birnbaum, A.K., Kriel, R.L., et al., 2001. Relative bioavailability of
Shank, R.P., Gardocki, J.F., et al., 1994. Topiramate: preclinical
lamotrigine chewable dispersible tablets administered rectally.
evaluation of structurally novel anticonvulsant. Epilepsia 35 (2),
Biton, V., Montouris, G.D., et al., 1999. A randomized
Shargel, L., Yu, A., 1999. Applied Biopharmaceutics and
placebo-controlled study of topiramate in primary generalized
Pharmacokinetics. Samford, Appleton and Lange.
Stanaway, L., Lambie, D.G., et al., 1985. Non-compliance with
anticonvulsant therapy as a cause of seizures. N. Z. Med. J.
Burstein, A.H., Fisher, K.M., et al., 2000. Absorption of phenytoin
from rectal suppositories formulated with a polyethylene glycol
Wheless, J.W., 2000. Use of topiramate in childhood generalized
base. Pharmacotherapy 20 (5), 562–567.
seizure disorders. J. Child. Neurol. 15 (Suppl. 1), S7–S13.
Décision rendue publique par lecture de son dispositif le 29 janvier 2008 et par affichage dans les locaux de l'Ordre des pharmaciens le 25 février 2008 Le Conseil national de l'Ordre des pharmaciens réuni le 29 janvier 2008 en séance publique ; Vu l'acte d'appel présenté par M. A, titulaire de la Pharmacie A sise …, enregistré au secrétariat du Conseil national de l'Ordre des pharmac
Brand Name (Generic Primary Use Ziagen® (Abacavir) ( Aripiprazole) Trisenox® (Arsenic Trioxide) To treat attention deficit problems CYP2D6 (Atomoxetine) Lipitor® ( Atorvastatin) To manage cholesterol. (Azathioprine) diseases of the immune system, post-organ transplant, Crohn’s disease, and ulcerative colitis. Victrelis® (Boceprevir) To treat hepatitis C i
 Relative bioavailability of topiramate administered rectally
Jeannine M. Conway , Angela K. Birnbaum , Robert L Kriel , James C. Cloyd
a Experimental and Clinical Pharmacology, Epilepsy Research and Education Program, College of Pharmacy,
University of Minnesota, 7-170 WDH 308 Harvard St. SE, Minneapolis, MN 55455, USA
b Departments of Pediatrics and Neurology, Hennepin County Medical Center, Minneapolis, MN, USA
Received 18 October 2002; received in revised form 12 March 2003; accepted 18 March 2003
Abstract
Relative bioavailability of topiramate administered rectally
Jeannine M. Conway , Angela K. Birnbaum , Robert L Kriel , James C. Cloyd
a Experimental and Clinical Pharmacology, Epilepsy Research and Education Program, College of Pharmacy,
University of Minnesota, 7-170 WDH 308 Harvard St. SE, Minneapolis, MN 55455, USA
b Departments of Pediatrics and Neurology, Hennepin County Medical Center, Minneapolis, MN, USA
Received 18 October 2002; received in revised form 12 March 2003; accepted 18 March 2003
Abstract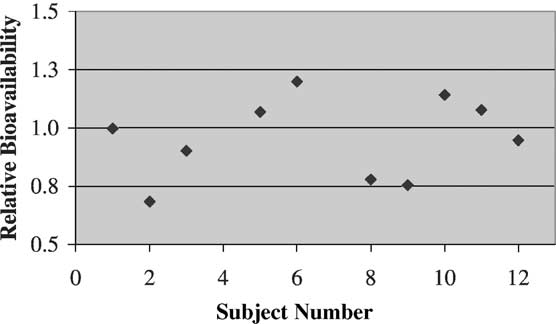
 J.M. Conway et al. / Epilepsy Research 54 (2003) 91–96
5. Statistical analysis
J.M. Conway et al. / Epilepsy Research 54 (2003) 91–96
5. Statistical analysis