Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Eduard matt
Zeitschrift für den Strafvollzug und Straffälligenhilfe 2004
On a difficult clientel
The topic of ADHD (Attention Deficit Hyperactivity Disorder) has increasingly been raised in
the last few years and has now also reached the penal in
showing this syndrom together with, or as a part of the personality disorders named in
psychiatric discourse are increasingly drawn into focus – not only concerning juveniles but
also adults. It is of such significance because the phenomenon and its manifestation contain
hints to problems in the fields of addiction and delinquency (and both combined). In the last
few years, this topic has predominantly been discussed among child and adolescent
psychiatrists (Döpfner 2000). A criminological perspective, discussion and integration is still
This corresponds to increasing complaints about deviant inmates, about adolescents who
repeatedly fail in school or other measures, who “stand out” due to constant truancy,
aggression, willingness to use violence and behavioural disorders. The rejection of the
strategy of incarceration (locking in) in the juvenile area as well as the increasing
overcrowding of the forensic psychiatry lead to severe cases as well as borderline cases
ending up in a regular prison. The staff often finds it difficult to deal with these cases. Results
and experiences from the psychiatric treatment show as one expression of the impairment,
that some of the violent criminals are not impressed by punishments at all. Here, social work
1 In the original: “Zappelphilipp”. Reference to Heinrich Hoffmann’s famous story “Der Zappelphilipp” (fidget philipp) of 1845 on a hyperactive boy (his own son) who rocks his chair until the tablecloth with everything on it falls down [translator’s note].
2 The author had the chance to attend two conferences on the subject: “ADHD in a Prison Population” in Hønefoss, Norway (5th-8th October 2003) within the context of a learning partnership between prisons in Germany (Bremen), Norway, Latvia and Estonia, which makes possible an exchange of practical experience. The program is supported by the European Union in form of the campaign Gruntvig II, which is part of the SOKRATES program. Furthermore, the conference of the New Society of Criminology in Munich (9th-11th October 2003) on “Applied Criminology between Freedom and Security”, in cooperation with the Arbeitsgemeinschaft für Methodik und Dokumentation in der Forensischen Psychiatrie (AGFP) [working group for methodology and documentation in the forensic psychiatry] with the relationship of criminology and psychiatry as a topic, as well as the new requirements facing an increase of ‘dissocial personalities’ among the offenders.
comes to nothing. To find better ways to react and to get away from mere disciplining
strategies, an improved check of the phenomena is necessary.
The connection between psychological disorders and criminal behaviour has recently been
drawn more into focus. Especially among persistent offenders and ‘Intensivtäter’ (repeat
offenders) there are unproportianally many cases of ADHD. Information from criminological
long-term studies shows a career pattern of delinquent behaviour. It is characterised by
persistence and deviant behaviour in early childhood (see e.g. Stelly, Thomas 2001, p.161:
Loeber 1998: Lösel, Bliesener 2003). The term ‘Intensivtäter’ has almost developed into a
psychiatric diagnosis (Rössner). The other important group contains the drug addicts. Here,
the therapy resistant and the substituted became the focus of attention (for adults: Willems
2001): With a ADHD diagnosis and therapy, there are much better achievements (e.g. hardly
any additional consumption). Likewise, ADHD in sex offenders is discussed as a significant
factor of risk, of vulnerability (Blocher 2001).
As an aspect of the folllowing discussion, it has to be clarified, as what ADHD shall be
categorised. Is it a defintie psychiatric diagnosis, a clear set of symptoms of an illness, a factor
of vulnerabilty (Bois 2003) or should one better speak of a psychological or even a technical
disorder, of a disturbed mental state or of a functional impairment (this term is gradually
gaining acceptance). For the discussion, the understanding and the handling of this
phenomenon, the consequences resulting herefrom are significantly different. The rather
narrow term of an illness almost inevitably leads to the assumption of an unchangable
situation as well as the necessity of medication. The term impairment avoids a
psychiatrisation of the group and allows very different forms of dealing with it. Impairments
require the learning of coping strategies. ADHD is not a reason to object to the order of a
(forensic) measure, as it cannot be subsumed under the legal term ‘another severe
psychological deviance’. Generally, a reduced responsibility is not assumed.
While the psychiatric perspective increasingly focusses on the task of a differentiated
diagnosis, a criminological perspective is still in development: The aspects considered here
would rather be prevention, practical consequences and possibilities of reaction to the
impairment. There is as yet no article on work with ADHD clients in jail. Yet, the functional
impairment has a huge impact on the life of the adolescents, on their behaviour, but also on
Diagnosis
ADHD is characterised by three symptom areas: attention disorder, hyperactivity and
impulsivity. The diagnosis can only be obtained on the basis of the description of directly
observable behaviour. According to DSM IV 18 symptoms are listed and categorised into
Symptoms: not being able to concentrate, lack of self-control, mind wandering, lack of
stamina (but also concentrated on interesting activities, then very motivated, attentive and
persistent), forgetful, does not seem to listen, stopping activities early, not getting ready, poor
revision, easily distracted, often refuses cognitive requests, learning difficulties
symptoms: wriggles a lot with hands and feet (thus ‘Zappelphilipp’ as a historical
description), cannot play, learn or work quietly, often gets up, excessive notorious activities,
subjective: feeling of restlessness, excessive motoricity, unorganised and restless activities,
- Impulsivity (lack of impulse control) (3 criteria)
Symptoms: cannot wait, interrupts others, often talks excessively, cannot interrupt activities,
cannot finish them either, rash, sudden action without thinking or waiting beforehand, also:
uncontrolled fits of rage, low acceptance of rules, inappropriate behaviour, changes of mood
For a confirmation of the diagnosis, 2/3 of the criteria should apply. The symptons should at
first have been observed before the 7th birthday. The symptoms should at least have been
observed for a period of six months, and the social maturity should be delayed. The diagnosis
The manifestation is characterised by a spectrum of variants: One main problem is the
disturbed control of behaviour, the so-called executive functions (e.g. for children packing
3 ‘For adults in particular, there is a lack regarding the following fields of symptoms: changes of mood, emotional overstimulatability, fits, desorganization of lifestyle and the inability to consequently finish a task’ (Blocher 2001, p.455). Also see: Neuhaus 2000.
school bags, organising and doing one thing after the other), the ADHD patient does not get it
together, cannot coordinate tasks, they lack self-organisation. They often do not react to
instructions. The motoric restlessness does not always have to be involved. Other symptoms
can be: dreamy, slow, without motivation, unconcentrated. In this case, one would speak of
ADD, a rather daydreaming type (more widespread among women). Other subtypes are
characterised by learning problems (partial performance disorder, spelling or arithmetic
problems going hand in hand with the impairment) and less by behavioural problems.
However, it must be pointed out that the impairments can be differently distinctive in their
intensity. They have dimensional rather than categorical character. They can likewise vary in
The impairment often goes together with other disorders/impairments. We here speak of a
high level of comorbidity. Disturbed social behaviour (in 30-50% of all cases), often
aggressive behaviour, depressive illnesses (10-40%, they suffer themselves), anxiety illnesses
(20-25%), learning disorders, partial performance disorders (10-25%), tics, Tourette
syndrome (up to 30%). Comorbidity increases with age. The disorder of social behaviour, the
symptom of dissociality is expressed in the following way: not fearing punishment, no
perception of reward or punishment, insensitivity, difficulties in recognising expressions of
emotions, low ability to empathize. There is an overproportional amount of cases with
aggressive behaviour. Different phenomena became evident: a disturbed self-image with a
low self-esteem, deviant perceptions and assessments of reality, diverse personality disorders.
Furthermore it always has to be considered that emotional and social competences are
strongly connected to the control and direction of attention.
ADHD is said to be genetically determined (disposition): often, one parent is found to show
the corresponding symptoms. A neurobiological metabolic disorder, a disorder of the so-
called dopaminerg system is in discussion. As yet, no objective connections have been found,
an objective, measurable biological substratum is not indicatable. The connection has to be
regarded as unspecific (even if in the sense of being at special risk). The interpretation of a
genetic cause however does not in its consequence imply a determinist understanding. In the
discussion, appearance, intensity and procedure is seen as the result of the combination of
genetic dispositions (predisposition, seen as a vulnerability factor) and social as well as family
influences. Especially a difficult social environment or psychosocial situation modify the
factor of disposition and can thus lead to different shapes of the impairment. Likewise, a
wrong (in this case inconsequent) upbringing can lead to a pronounced course of ADHD.
Genetics and social influences are no longer seen as factors excluding each other but rather
under the aspect of interaction and reinforcement. The causes for ADHD thus neither are a
miseducation nor a brain damage in early childhood, while both can have a negative influence
on the symptomization. A biologication of social matters (Jantzen 2001) is to be opposed.
The impairments caused by a lack of attention, hyperactivity and lack of control of impulse
can manifest themselves in the most different fields of the biographical development:
increased risk of failure at school, education or professional training, delinquency, criminality,
unemployment, descent down the social ladder, family burdens, behavioural disorders (being
a loner, social isolation) as well as an increased risk of invalidity (e.g. due to accidents). The
willingness to take risks often corresponding to ADHD – depending on the intensity of the
impairment – the search of equals, the ‘wrong friends’, the sensation seeking leads the
persons into risk. Likewise, the relative span of attention is responsible for some phenomena.
To take the behaviour for an impairment also requires not to suppose, the person could
actually discipline himself but does not want to. He does not react to well meant advice, he
would like to but is not able to do it. There is a huge gap yawning between being willing to do
something and being able to do something. Hence, it is important for the understanding of the
action, not to take it as inappropriate behaviour or provocation and not to accuse, reproach or
even discipline him. It is to be undestood as an expression of the impairment and therefore
In the field of crime, we have a special risk, as the increased willingness to take risks but also
the resulting social isolation can increasingly lead to delinquent behaviour. Thus, there is an
overproportional amount of ADHD cases among delinquent youths. For those in jail, the
diagnosis has rarely been given before. Occasionally, there might be a little hint in the file.
Mostly, however, they are undiagnosed and untreated. ADHD as an impairment itself does
not lead to increased delinquency but to a significantly higher risk. This is concerning the
untreated, while the quote of those therapized corresponds to the one of average youths.
Often, the entry into delinquency happens early, with a broad set of offences. In a study, it is
reported that of those having had an early development of the impairment 12% had serious
contact with the police until the age of 11, and 35% until the age of 16. Most of them had
completed less than 7 years of school. In this group we also find more acts of violence.
Spreading
Even the frequency (prevalence) of ADHD is not determined clearly. About 2-6% of the
children and youths aged 6 to 18 years are said to be concerned (BMGS 2002), others assume
a span of 3-10%, a conservative estimation here is 5%. The relation of gender is not
determined definitely, it varies between 3:1 and 9:1 (boys:girls). Opposing common
assumptions, it is believed today, that the impairment does not always‘ grow out’ in adult age.
For about 50-70% of the cases, it persists. It is thus not always a temporary impairment.
The diagnosis is difficult to give, as it refers to behaviour and as it is gained on the basis of
self-assessment or assessment by others. Applying an intensive interview of 2-3 hours for
clarification is hardly affordable generally and also quite difficult to perform. So this method
of gathering information is not very secure. It is mostly self-descriptions that are applied.
Information from other sources, especially from parents or teachers, is most of the time
Within jail, it is estimated that 25-30% of the youths are concerned. In one prison, among
adults, indications of the disorder were found in 43% (Ziegler et al. 2003, p.17). Indications of
the disorder were increasingly found among persistent offenders. Singular central symptoms
ADHD however only is a syndrome in the analyses of deviant behaviour (with a
simultaneously high comorbidity). Especially psychiatrists look for the so-called dissocial
personality disorder among the prisoners (diagnosis scheme ICD 10, F 60.2). Prevalences of
personality disorders among prisoners are presented in a span of 7 to 81% (Frädrich, Pfäfflin
ong young prisoners, a prevalence of 50% of oppositional, dissocial behviour is
estimated. In a Norwegian study with prisoners, 50% were found to have affective disorders,
experiences of abuse in almost all of them and personality disorders in 85% (Rasmussen). An
investigation in Halle (Germany) with people accused in the district court found 43.8% of
personality disorders of the dissocial type 35.7%. The ‘aggressive subtype’ in personality
disorders is listed with a prevalence of 25-28%. For a comparison, the prevalence of such
phenomena in within the control group/average population: 2.5%.
Now, the question of mechanisms of selection is raised. If there are 4% of ADHD cases at
school while there are 30% in jail, how does this development come about?
One question yet always remains: Which problems are due to the impairment, which are due
to the situation in prison? It has to be differentiated between symptoms presenting an
adjustment in jail, a consequence of conditions in jail and – often inappropriate – coping
strategies on the one hand, and symptoms that can be interpreted as enduring characteristics of
the problematic nature of the life of those concerned (Paverdian 1993).
A causal therapy does not exist, a medication does not show curing effects. Facing a diversity
of shapings and causes, a multimodal therapy is generally recommended. However,
medication is still the dominating form of therapy. By giving a low dose of an amphetamine, a
transmitter, which is involved in the transmission of stimulation, the proportion of serotonin
in the brain is influenced, the degrading of dopamine is hindered, and thus, an increase of the
ability to concentrate, to learn and quiet is achieved. In treatment, a better brain performance
However, if medication is always appropriate is controversial. For some, in severe cases, it
can be necessary for the production of concentration. For others however, other methods can
be similarly successful. It has to be considered that medication has the effect of quieting down
(and here, one always has to ask, for what purpose). The risk of ‘normalisation’ of undesirable
behaviour is high. Furthermore, not all react to medication (70% of the youths, even less
adults). The compliance is rather weak, especially hyperactives get tired of the medication
(and therefore refuse it), the therapy requires a high level of motivation. Some, especially
youths, experience the medication as overpowering and disciplining.
The substance methylphenidate (known as the medicament Ritalin®) is an amphetamine,
which has mechanisms in its effect similar to cocaine and other drugs belonging to the
4 It is to be mentioned critically that aspects of delinquency as well as corresponding behaviours (repeated
amphetamines (but not only those). Even if the substance is comparable, the doses are very
different. Ritalin® only contains a very small amount. The mechanism of the effect is also
different (the one euphorizes, the other normalizes). The discussion about drugs and addiction
plays a not insignificant role – Ritalin® falls under the law governing the use and traffic of
drugs (in Germany) and therefore can only be prescribed for children and youths. The fear of
an addiction, the aspect of fighting an addiction with a substance concerned by the law is
often seen as a reason for refusing the intake. A new medicament that would not concern the
law and could also be used for adults promises a higher rate of prescriptions.
Experts assume, that possibly some addicts are undiagnosed ADHD cases, who take drugs
(cocaine, amphetamines, also other drugs) as a sort of self-medication, as an inadequate form
of coping with their perceived impairment. Due to their biographical and social situation, they
are yet often in risk of becoming addicted. Thus, they are over-represented among drug
addicts. Yet, the medication does not involve the risk of a development of an addiction;
therapized ADHD patients have a risk of developing addictions that is comparable to that of
It has to be noted that Ritalin® is not a miracle cure. The administering, if necessary, should
always be embedded in other measures. While it does have the effect of a temporary
improvement of concentration, it should be secured that this concentration can also be used.
By medication alone, deviances in behaviour and social life cannot be cured. An appropriate
communicative and social behaviour has to be learned. Without the appropriate requirements
and caretaking, medication alone does not prove successful on a long-term basis. It can thus
be necessary as a prerequisite for a treatment. It makes it possible for the patient to live up to
his potential. The combination of medication and other therapy methods thus prove to
produce good effects. With the help of medication, something is made available that could not
be used without medication. It should yet be the last choice and only be applied in severe
When reacting to the impairment, the distinctness of the individual case, facing a great variety
of symptoms, has to be considered. An empathy training for instance is only appropriate if
there are significant disorders in this field. Behavioural therapy proved to be useful in cases of
punishment, risky behaviour etc.) are counted as symptoms which are included into the diagnosis.
inattentiveness but also aggressive behaviour (Petermann et al. 2002). Likewise, family
therapy is successful: the establishment of a clear educational standpoint of the parents
reduces hyperactive reactions significantly (Hüther, Bonney 2002). For the aggressive
elements and disorders in social behaviour mostly involved, other methods can be useful
(Cognitive skills programs: ATV (anti-aggression-training), trainig of social competences
ergotherapy). The main focus is on the measures for the improvement of attention and the
control and direction of behaviour. The aim is the mastering of coping strategies, the
management of symptoms and situations. It is important to develop useful techniques in the
dealing with the impairment, to learn to control behaviour.
The prognosis is better the earlier the effective treatment starts. Therefore, an early
involvement of family and schoolis necessary. If however hindering social factors are added,
further social risk factors, the social prognosis is unfavourable. Comorbid factors such as
aggressiveness and dissocial behaviour but also a failed treatment worsen the prognosis. It has
to be considered that ADHD is only one of many risk factors for the social development of
An effective therapy requires an intense cooperation of school, parents, psychologists,
trainers, legal authorities, police, social services and others – a cooperation, in which none of
the institutions is experienced. Problems like data protection and professional duty to maintain
confidentiality might make an effective cooperation difficult.
What can be done in a place of detention to improve the situation of those concerned? Which
treatments can be offered? In the Chen, first experiences in the dealing
with ADHD clients were made in a ergotherapy course. Furthermore, there is a course for the
training of social competences (Fit for Life). The treatment itself is merely symptomatic.
What can be done beside medication is mainly concerning management, the coping with
symptoms and situations. It is important for the youths to learn to deal with the impairment.
The purchase of a punchbag for example proved to be a good investment to ‘let off steam’.
5 For the different programs of violence prevention, especially applied in the field of school, see Schick, Ott 2002.
6 The Chance project is runnig from 01.11.2000-31.12.2004 and is supported by the senator for labour, women, health, youth and social services, the European Community (main emphasis 10: qualification in the penal system), the job centres of Bremen and Bremerhaven as well as the senator of justice. The responsible body is JUDIT Bremen for the place of detention in Bremen. See Matt 2003, http://www.chance.uni-bremen.de.
The participants are instructed to control and work off their impulses this way. It is a long-
term training aspect: They learn to realize, when they should rather get out of a situation.
Other instructive, directive treatments have proven useful (training methods, perceptual
training, sociotherapy). Other forms of producing concentration may also come into effect.
The establishment of computerbased learning for instance was found to be successful.
Appropriate assisting measures still have to be developed and offered. Further appliccable
therapies are being searched for in order to gain experience with the realization and the
adaption. Facing a long period of experiencing the failure of ADHD patients, it is especially
important to give them a sense of achievement for them to strengthen their self-esteem.
ADHD and delinquency
ADHD can influence the biographical career and the social situation of the individual very
strongly and often negatively. For the understanding of this process, Stephan Quensel’s
(1970) considerations on the ‘mutual process of building-up’ to a descending spiral are
especially relevant, as they contain the temporary process. The development from first
deviances resulting from ADHD to a negative career up to a sentence in prison is to be
understood as an interactive process between (socially) deviant behaviour on the one hand and
social reactions on the other. Some develop problematic behaviour in reaction to the self-
perceived impairments as well as to their failures in everyday life or at school. However, these
children very early experience rejection, due to their own inattentive, hyperactive and/or
aggressive behaviour. Most of them cannot cope with disappointment. These early rejections
can lead to social isolation and therefore present a significant risk. To react by being the
clown in class or getting into an outsider position, one does not create social interaction or
acknowledgement from others. The isolation is rather reinforced. Experiences of
stigmatization or selection become pronounced. The problems and the behaviour produced by
the impairment due to restlessness and impulsive behaviour can lead into unfavourable
situations, if not avoided. Such situations are: delayed development, performance problems at
school, insecurity and lack of confidence, burdening relationships to adults. In the proceeding
of the development, further problematic behaviour can develop (addiction, delinquency), if
the development is not cushioned by a protecting factor (or the patient even learns to use his
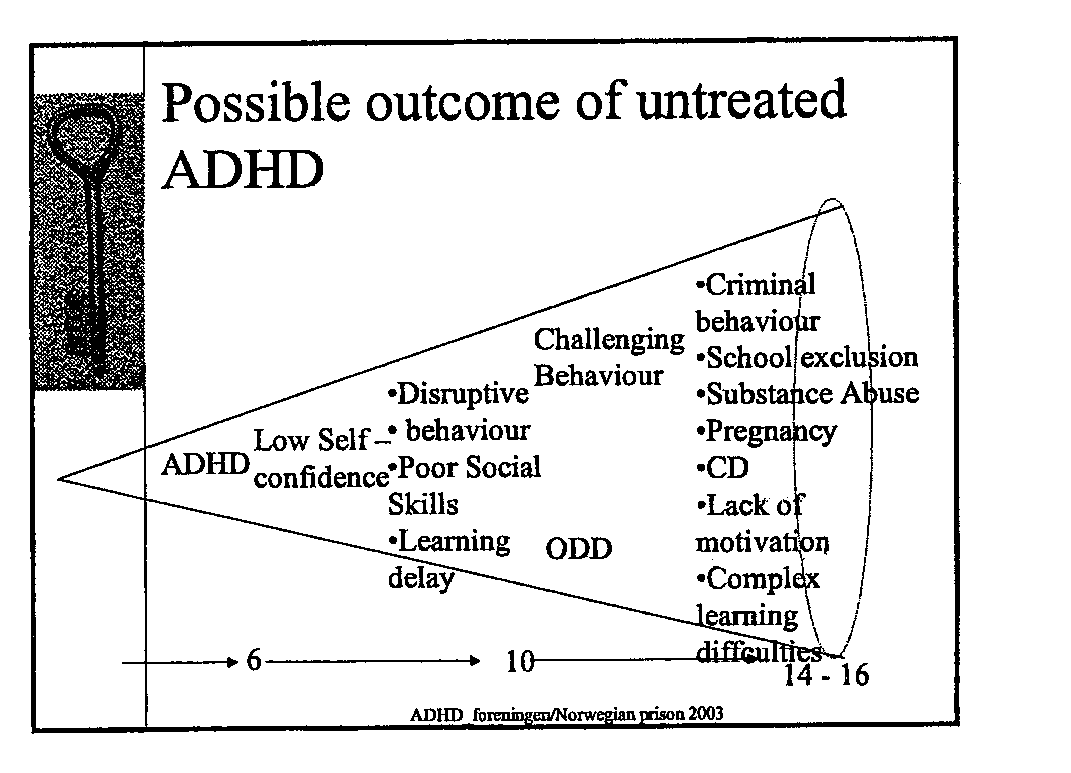
oddities construcively and successfully). Per level of severeness of the problems, there is a
broad set of variations. In the sense of criminological longitudinal studies, we are confronted
with difficult courses of cases, with an accumulation of discrimination with inadequate
compensation mechanisms on the part of those concerned, as well as the negative reactions on
the part of the social environment. The model of development as a diagram:
DIAGRAM (Possible outcoume of untreated ADHD)
Consequently, it is important to develop appropriate offers, which make it possible to master
those deviances in behaviour. Appropriate practices in the dealing with the impairment have
to be communicated. Medication alone would at most make security and order easy in the
ward, but it would not do anything for the patient himself. Appropriate pedagogical and
therapeutical support has to be developed.
Especially for those deviant youths with long careers of delinquency, an increased
cooperation of the penal institution with psychologists and psychiatrists seems to be required.
A distinction of exclusive offers, especially for this group, is needed. The developing risk of
stigmatization has to be opposed. Juvenile prisoners react very intensely on terms like
psychologically disturbed or disabled. Thus, a reconsideration is required. Aspects of the
biographical and social situation as well as the emotional, cognitive and social competence (as
well as the compensation strategies therefore developed) are to be involved into the therapy
process as conditions. Only a qualified, differentiating diagnosis and an improved awareness
of the difficulties can lead to adequate modes of reaction, can make it possible to fulfil the
Literatur: Blocher, Detlev et al.: Symptome aus dem Spektrum des hyperkinetischen Syndroms bei
Sexualdelinquenten. In: Fortschritte Neurologie Psychiatrie 69, 2001, S. 453-459
du Bois, Reinmar: ADHS, Aggressivität und die Verschreibung von Stimulantien. In: Recht und
Bronder, Knut Halvard: Living with ADHD. Presentation. Hønefoss 2003 Döpfner, Manfred; Jan Frölich; Gerd Lehmkuhl: Hyperkinetische Störungen. Göttingen 2000 Eckpunkte der Ergebnisse der vom Bundesministerium für Gesundheit und Soziale Sicherung
durchgeführten interdisziplinären Konsensuskonferenz zur Verbesserung der Versorgung von Kindern, Jugendlichen und Erwachsenen mit Aufmerksamkeitsdefizit-Hyperaktivitätsstörung (ADHS), Bonn 28. und 29. Oktober 2002.
Fädrich, Stefan; Friedemann Pfäfflin: Zur Prävalenz von Persönlichkeitsstörungen bei
Strafgefangenen. In: Recht und Psychiatrie 18, 2000, S. 95-104
Huber, Nicole: Jugendkriminalität und ADHS. Diplomarbeit Villingen-Schwenningen 2001 Hüther, Gerald; Helmut Bonney: Neues vom Zappelphilipp. Düsseldorf 2002 Jantzen, Wolfgang: Über die soziale Konstruktion von Verhaltensstörungen. Das Beispiel
„Aufmerksamkeitsdefizitsyndrom“ (ADS). In: Zeitschrift für Heilpädagogik 6, 2001, S. 222-231
Loeber, Rolf; Farrington, David P. et al.: Antisocial Behavior and Mental Problems. Mahwah 1998 Lösel, Friedrich; Thomas Bliesener: Aggression und Delinquenz unter Jugendlichen. Untersuchungen
von kognitiven und sozialen Bedingungen. Neuwied 2003
Matt, Eduard: Der Projektverbund „Chance“ in Bremen: Konzeption und Praxis. Zeitschrift für
Strafvollzug und Straffälligenhilfe 52, 2003. S. 81-88
Neuhaus, Cordula: Das ist ja wieder typisch! - ADS bei Jugendlichen und jungen Erwachsenen:
Extravaganzen, Stimmungslabilitäten, Somatisierungstendenzen. In: Thilo Fitzner, Werner Stark (Hrsg.): ADS: verstehen - akzeptieren - helfen. Weinheim 2000, S. 94-117
Parverdian, Joseph: „Ver-rücktheit“ als Bewältigungsstrategie im Strafvollzug. In: Recht und
Petermann, Franz; Nicole Gerken; Heike Natzke; Hans-Jörg Walter: Verhaltenstraining für
Schulanfänger. Trainingshandbuch mit CD. Paderborn 2002
Quensel, Stephan: Wie wird man kriminell? In: Kritische Justiz 3, 1970, S. 377-382 Schick, Andreas; Isabel Ott: Gewaltprävention an Schulen - Ansätze und Ergebnisse. In: Praxis der
Kinderpsychologie und Kinderpsychiatrie 51, 2002, S. 766-791
Stelly, Wolfgang; Jürgen Thomas: Einmal Verbrecher - immer Verbrecher? Opladen 2001 Wilems, Timothy E. et al.: A controlled clinical trial of Bupropion for Attention Deficit Hyperactivity
Disorder in adults. In: American Journal of Psychiatry158, 2001, S. 282-288
Ziegler, E.; D. Blocher; J. Groß; M. Rösler: Erfassung von Symptomen aus dem Spektrum des
Hyperkinetischen Syndroms bei Häftlingen einer Justizvollzugsanstalt. In: Recht und Psychiatrie 21, 2003, S. 17-21

 Zeitschrift für den Strafvollzug und Straffälligenhilfe 2004
On a difficult clientel
Zeitschrift für den Strafvollzug und Straffälligenhilfe 2004
On a difficult clientel 
 comes to nothing. To find better ways to react and to get away from mere disciplining
strategies, an improved check of the phenomena is necessary.
The connection between psychological disorders and criminal behaviour has recently been
drawn more into focus. Especially among persistent offenders and ‘Intensivtäter’ (repeat
offenders) there are unproportianally many cases of ADHD. Information from criminological
long-term studies shows a career pattern of delinquent behaviour. It is characterised by
persistence and deviant behaviour in early childhood (see e.g. Stelly, Thomas 2001, p.161:
Loeber 1998: Lösel, Bliesener 2003). The term ‘Intensivtäter’ has almost developed into a
psychiatric diagnosis (Rössner). The other important group contains the drug addicts. Here,
the therapy resistant and the substituted became the focus of attention (for adults: Willems
2001): With a ADHD diagnosis and therapy, there are much better achievements (e.g. hardly
any additional consumption). Likewise, ADHD in sex offenders is discussed as a significant
factor of risk, of vulnerability (Blocher 2001).
As an aspect of the folllowing discussion, it has to be clarified, as what ADHD shall be
categorised. Is it a defintie psychiatric diagnosis, a clear set of symptoms of an illness, a factor
of vulnerabilty (Bois 2003) or should one better speak of a psychological or even a technical
disorder, of a disturbed mental state or of a functional impairment (this term is gradually
comes to nothing. To find better ways to react and to get away from mere disciplining
strategies, an improved check of the phenomena is necessary.
The connection between psychological disorders and criminal behaviour has recently been
drawn more into focus. Especially among persistent offenders and ‘Intensivtäter’ (repeat
offenders) there are unproportianally many cases of ADHD. Information from criminological
long-term studies shows a career pattern of delinquent behaviour. It is characterised by
persistence and deviant behaviour in early childhood (see e.g. Stelly, Thomas 2001, p.161:
Loeber 1998: Lösel, Bliesener 2003). The term ‘Intensivtäter’ has almost developed into a
psychiatric diagnosis (Rössner). The other important group contains the drug addicts. Here,
the therapy resistant and the substituted became the focus of attention (for adults: Willems
2001): With a ADHD diagnosis and therapy, there are much better achievements (e.g. hardly
any additional consumption). Likewise, ADHD in sex offenders is discussed as a significant
factor of risk, of vulnerability (Blocher 2001).
As an aspect of the folllowing discussion, it has to be clarified, as what ADHD shall be
categorised. Is it a defintie psychiatric diagnosis, a clear set of symptoms of an illness, a factor
of vulnerabilty (Bois 2003) or should one better speak of a psychological or even a technical
disorder, of a disturbed mental state or of a functional impairment (this term is gradually 
 impairment has a huge impact on the life of the adolescents, on their behaviour, but also on
Diagnosis
impairment has a huge impact on the life of the adolescents, on their behaviour, but also on
Diagnosis 
 school bags, organising and doing one thing after the other), the ADHD patient does not get it
together, cannot coordinate tasks, they lack self-organisation. They often do not react to
instructions. The motoric restlessness does not always have to be involved. Other symptoms
can be: dreamy, slow, without motivation, unconcentrated. In this case, one would speak of
ADD, a rather daydreaming type (more widespread among women). Other subtypes are
characterised by learning problems (partial performance disorder, spelling or arithmetic
problems going hand in hand with the impairment) and less by behavioural problems.
However, it must be pointed out that the impairments can be differently distinctive in their
intensity. They have dimensional rather than categorical character. They can likewise vary in
The impairment often goes together with other disorders/impairments. We here speak of a
high level of comorbidity. Disturbed social behaviour (in 30-50% of all cases), often
aggressive behaviour, depressive illnesses (10-40%, they suffer themselves), anxiety illnesses
(20-25%), learning disorders, partial performance disorders (10-25%), tics, Tourette
syndrome (up to 30%). Comorbidity increases with age. The disorder of social behaviour, the
symptom of dissociality is expressed in the following way: not fearing punishment, no
perception of reward or punishment, insensitivity, difficulties in recognising expressions of
emotions, low ability to empathize. There is an overproportional amount of cases with
aggressive behaviour. Different phenomena became evident: a disturbed self-image with a
low self-esteem, deviant perceptions and assessments of reality, diverse personality disorders.
Furthermore it always has to be considered that emotional and social competences are
strongly connected to the control and direction of attention.
ADHD is said to be genetically determined (disposition): often, one parent is found to show
the corresponding symptoms. A neurobiological metabolic disorder, a disorder of the so-
called dopaminerg system is in discussion. As yet, no objective connections have been found,
an objective, measurable biological substratum is not indicatable. The connection has to be
regarded as unspecific (even if in the sense of being at special risk). The interpretation of a
genetic cause however does not in its consequence imply a determinist understanding. In the
discussion, appearance, intensity and procedure is seen as the result of the combination of
genetic dispositions (predisposition, seen as a vulnerability factor) and social as well as family
influences. Especially a difficult social environment or psychosocial situation modify the
school bags, organising and doing one thing after the other), the ADHD patient does not get it
together, cannot coordinate tasks, they lack self-organisation. They often do not react to
instructions. The motoric restlessness does not always have to be involved. Other symptoms
can be: dreamy, slow, without motivation, unconcentrated. In this case, one would speak of
ADD, a rather daydreaming type (more widespread among women). Other subtypes are
characterised by learning problems (partial performance disorder, spelling or arithmetic
problems going hand in hand with the impairment) and less by behavioural problems.
However, it must be pointed out that the impairments can be differently distinctive in their
intensity. They have dimensional rather than categorical character. They can likewise vary in
The impairment often goes together with other disorders/impairments. We here speak of a
high level of comorbidity. Disturbed social behaviour (in 30-50% of all cases), often
aggressive behaviour, depressive illnesses (10-40%, they suffer themselves), anxiety illnesses
(20-25%), learning disorders, partial performance disorders (10-25%), tics, Tourette
syndrome (up to 30%). Comorbidity increases with age. The disorder of social behaviour, the
symptom of dissociality is expressed in the following way: not fearing punishment, no
perception of reward or punishment, insensitivity, difficulties in recognising expressions of
emotions, low ability to empathize. There is an overproportional amount of cases with
aggressive behaviour. Different phenomena became evident: a disturbed self-image with a
low self-esteem, deviant perceptions and assessments of reality, diverse personality disorders.
Furthermore it always has to be considered that emotional and social competences are
strongly connected to the control and direction of attention.
ADHD is said to be genetically determined (disposition): often, one parent is found to show
the corresponding symptoms. A neurobiological metabolic disorder, a disorder of the so-
called dopaminerg system is in discussion. As yet, no objective connections have been found,
an objective, measurable biological substratum is not indicatable. The connection has to be
regarded as unspecific (even if in the sense of being at special risk). The interpretation of a
genetic cause however does not in its consequence imply a determinist understanding. In the
discussion, appearance, intensity and procedure is seen as the result of the combination of
genetic dispositions (predisposition, seen as a vulnerability factor) and social as well as family
influences. Especially a difficult social environment or psychosocial situation modify the

 factor of disposition and can thus lead to different shapes of the impairment. Likewise, a
wrong (in this case inconsequent) upbringing can lead to a pronounced course of ADHD.
Genetics and social influences are no longer seen as factors excluding each other but rather
under the aspect of interaction and reinforcement. The causes for ADHD thus neither are a
miseducation nor a brain damage in early childhood, while both can have a negative influence
on the symptomization. A biologication of social matters (Jantzen 2001) is to be opposed.
The impairments caused by a lack of attention, hyperactivity and lack of control of impulse
can manifest themselves in the most different fields of the biographical development:
increased risk of failure at school, education or professional training, delinquency, criminality,
unemployment, descent down the social ladder, family burdens, behavioural disorders (being
a loner, social isolation) as well as an increased risk of invalidity (e.g. due to accidents). The
willingness to take risks often corresponding to ADHD – depending on the intensity of the
impairment – the search of equals, the ‘wrong friends’, the sensation seeking leads the
persons into risk. Likewise, the relative span of attention is responsible for some phenomena.
To take the behaviour for an impairment also requires not to suppose, the person could
actually discipline himself but does not want to. He does not react to well meant advice, he
would like to but is not able to do it. There is a huge gap yawning between being willing to do
something and being able to do something. Hence, it is important for the understanding of the
action, not to take it as inappropriate behaviour or provocation and not to accuse, reproach or
even discipline him. It is to be undestood as an expression of the impairment and therefore
In the field of crime, we have a special risk, as the increased willingness to take risks but also
the resulting social isolation can increasingly lead to delinquent behaviour. Thus, there is an
overproportional amount of ADHD cases among delinquent youths. For those in jail, the
diagnosis has rarely been given before. Occasionally, there might be a little hint in the file.
Mostly, however, they are undiagnosed and untreated. ADHD as an impairment itself does
not lead to increased delinquency but to a significantly higher risk. This is concerning the
untreated, while the quote of those therapized corresponds to the one of average youths.
Often, the entry into delinquency happens early, with a broad set of offences. In a study, it is
reported that of those having had an early development of the impairment 12% had serious
factor of disposition and can thus lead to different shapes of the impairment. Likewise, a
wrong (in this case inconsequent) upbringing can lead to a pronounced course of ADHD.
Genetics and social influences are no longer seen as factors excluding each other but rather
under the aspect of interaction and reinforcement. The causes for ADHD thus neither are a
miseducation nor a brain damage in early childhood, while both can have a negative influence
on the symptomization. A biologication of social matters (Jantzen 2001) is to be opposed.
The impairments caused by a lack of attention, hyperactivity and lack of control of impulse
can manifest themselves in the most different fields of the biographical development:
increased risk of failure at school, education or professional training, delinquency, criminality,
unemployment, descent down the social ladder, family burdens, behavioural disorders (being
a loner, social isolation) as well as an increased risk of invalidity (e.g. due to accidents). The
willingness to take risks often corresponding to ADHD – depending on the intensity of the
impairment – the search of equals, the ‘wrong friends’, the sensation seeking leads the
persons into risk. Likewise, the relative span of attention is responsible for some phenomena.
To take the behaviour for an impairment also requires not to suppose, the person could
actually discipline himself but does not want to. He does not react to well meant advice, he
would like to but is not able to do it. There is a huge gap yawning between being willing to do
something and being able to do something. Hence, it is important for the understanding of the
action, not to take it as inappropriate behaviour or provocation and not to accuse, reproach or
even discipline him. It is to be undestood as an expression of the impairment and therefore
In the field of crime, we have a special risk, as the increased willingness to take risks but also
the resulting social isolation can increasingly lead to delinquent behaviour. Thus, there is an
overproportional amount of ADHD cases among delinquent youths. For those in jail, the
diagnosis has rarely been given before. Occasionally, there might be a little hint in the file.
Mostly, however, they are undiagnosed and untreated. ADHD as an impairment itself does
not lead to increased delinquency but to a significantly higher risk. This is concerning the
untreated, while the quote of those therapized corresponds to the one of average youths.
Often, the entry into delinquency happens early, with a broad set of offences. In a study, it is
reported that of those having had an early development of the impairment 12% had serious

 contact with the police until the age of 11, and 35% until the age of 16. Most of them had
completed less than 7 years of school. In this group we also find more acts of violence.
Spreading
contact with the police until the age of 11, and 35% until the age of 16. Most of them had
completed less than 7 years of school. In this group we also find more acts of violence.
Spreading 
 disorders is listed with a prevalence of 25-28%. For a comparison, the prevalence of such
phenomena in within the control group/average population: 2.5%.
Now, the question of mechanisms of selection is raised. If there are 4% of ADHD cases at
school while there are 30% in jail, how does this development come about?
One question yet always remains: Which problems are due to the impairment, which are due
to the situation in prison? It has to be differentiated between symptoms presenting an
adjustment in jail, a consequence of conditions in jail and – often inappropriate – coping
strategies on the one hand, and symptoms that can be interpreted as enduring characteristics of
the problematic nature of the life of those concerned (Paverdian 1993).
A causal therapy does not exist, a medication does not show curing effects. Facing a diversity
of shapings and causes, a multimodal therapy is generally recommended. However,
medication is still the dominating form of therapy. By giving a low dose of an amphetamine, a
transmitter, which is involved in the transmission of stimulation, the proportion of serotonin
in the brain is influenced, the degrading of dopamine is hindered, and thus, an increase of the
ability to concentrate, to learn and quiet is achieved. In treatment, a better brain performance
However, if medication is always appropriate is controversial. For some, in severe cases, it
can be necessary for the production of concentration. For others however, other methods can
be similarly successful. It has to be considered that medication has the effect of quieting down
(and here, one always has to ask, for what purpose). The risk of ‘normalisation’ of undesirable
behaviour is high. Furthermore, not all react to medication (70% of the youths, even less
adults). The compliance is rather weak, especially hyperactives get tired of the medication
(and therefore refuse it), the therapy requires a high level of motivation. Some, especially
youths, experience the medication as overpowering and disciplining.
The substance methylphenidate (known as the medicament Ritalin®) is an amphetamine,
which has mechanisms in its effect similar to cocaine and other drugs belonging to the
4 It is to be mentioned critically that aspects of delinquency as well as corresponding behaviours (repeated
disorders is listed with a prevalence of 25-28%. For a comparison, the prevalence of such
phenomena in within the control group/average population: 2.5%.
Now, the question of mechanisms of selection is raised. If there are 4% of ADHD cases at
school while there are 30% in jail, how does this development come about?
One question yet always remains: Which problems are due to the impairment, which are due
to the situation in prison? It has to be differentiated between symptoms presenting an
adjustment in jail, a consequence of conditions in jail and – often inappropriate – coping
strategies on the one hand, and symptoms that can be interpreted as enduring characteristics of
the problematic nature of the life of those concerned (Paverdian 1993).
A causal therapy does not exist, a medication does not show curing effects. Facing a diversity
of shapings and causes, a multimodal therapy is generally recommended. However,
medication is still the dominating form of therapy. By giving a low dose of an amphetamine, a
transmitter, which is involved in the transmission of stimulation, the proportion of serotonin
in the brain is influenced, the degrading of dopamine is hindered, and thus, an increase of the
ability to concentrate, to learn and quiet is achieved. In treatment, a better brain performance
However, if medication is always appropriate is controversial. For some, in severe cases, it
can be necessary for the production of concentration. For others however, other methods can
be similarly successful. It has to be considered that medication has the effect of quieting down
(and here, one always has to ask, for what purpose). The risk of ‘normalisation’ of undesirable
behaviour is high. Furthermore, not all react to medication (70% of the youths, even less
adults). The compliance is rather weak, especially hyperactives get tired of the medication
(and therefore refuse it), the therapy requires a high level of motivation. Some, especially
youths, experience the medication as overpowering and disciplining.
The substance methylphenidate (known as the medicament Ritalin®) is an amphetamine,
which has mechanisms in its effect similar to cocaine and other drugs belonging to the
4 It is to be mentioned critically that aspects of delinquency as well as corresponding behaviours (repeated

 amphetamines (but not only those). Even if the substance is comparable, the doses are very
different. Ritalin® only contains a very small amount. The mechanism of the effect is also
different (the one euphorizes, the other normalizes). The discussion about drugs and addiction
plays a not insignificant role – Ritalin® falls under the law governing the use and traffic of
drugs (in Germany) and therefore can only be prescribed for children and youths. The fear of
an addiction, the aspect of fighting an addiction with a substance concerned by the law is
often seen as a reason for refusing the intake. A new medicament that would not concern the
law and could also be used for adults promises a higher rate of prescriptions.
Experts assume, that possibly some addicts are undiagnosed ADHD cases, who take drugs
(cocaine, amphetamines, also other drugs) as a sort of self-medication, as an inadequate form
of coping with their perceived impairment. Due to their biographical and social situation, they
are yet often in risk of becoming addicted. Thus, they are over-represented among drug
addicts. Yet, the medication does not involve the risk of a development of an addiction;
therapized ADHD patients have a risk of developing addictions that is comparable to that of
It has to be noted that Ritalin® is not a miracle cure. The administering, if necessary, should
always be embedded in other measures. While it does have the effect of a temporary
improvement of concentration, it should be secured that this concentration can also be used.
By medication alone, deviances in behaviour and social life cannot be cured. An appropriate
communicative and social behaviour has to be learned. Without the appropriate requirements
and caretaking, medication alone does not prove successful on a long-term basis. It can thus
be necessary as a prerequisite for a treatment. It makes it possible for the patient to live up to
his potential. The combination of medication and other therapy methods thus prove to
produce good effects. With the help of medication, something is made available that could not
be used without medication. It should yet be the last choice and only be applied in severe
When reacting to the impairment, the distinctness of the individual case, facing a great variety
of symptoms, has to be considered. An empathy training for instance is only appropriate if
there are significant disorders in this field. Behavioural therapy proved to be useful in cases of
punishment, risky behaviour etc.) are counted as symptoms which are included into the diagnosis.
amphetamines (but not only those). Even if the substance is comparable, the doses are very
different. Ritalin® only contains a very small amount. The mechanism of the effect is also
different (the one euphorizes, the other normalizes). The discussion about drugs and addiction
plays a not insignificant role – Ritalin® falls under the law governing the use and traffic of
drugs (in Germany) and therefore can only be prescribed for children and youths. The fear of
an addiction, the aspect of fighting an addiction with a substance concerned by the law is
often seen as a reason for refusing the intake. A new medicament that would not concern the
law and could also be used for adults promises a higher rate of prescriptions.
Experts assume, that possibly some addicts are undiagnosed ADHD cases, who take drugs
(cocaine, amphetamines, also other drugs) as a sort of self-medication, as an inadequate form
of coping with their perceived impairment. Due to their biographical and social situation, they
are yet often in risk of becoming addicted. Thus, they are over-represented among drug
addicts. Yet, the medication does not involve the risk of a development of an addiction;
therapized ADHD patients have a risk of developing addictions that is comparable to that of
It has to be noted that Ritalin® is not a miracle cure. The administering, if necessary, should
always be embedded in other measures. While it does have the effect of a temporary
improvement of concentration, it should be secured that this concentration can also be used.
By medication alone, deviances in behaviour and social life cannot be cured. An appropriate
communicative and social behaviour has to be learned. Without the appropriate requirements
and caretaking, medication alone does not prove successful on a long-term basis. It can thus
be necessary as a prerequisite for a treatment. It makes it possible for the patient to live up to
his potential. The combination of medication and other therapy methods thus prove to
produce good effects. With the help of medication, something is made available that could not
be used without medication. It should yet be the last choice and only be applied in severe
When reacting to the impairment, the distinctness of the individual case, facing a great variety
of symptoms, has to be considered. An empathy training for instance is only appropriate if
there are significant disorders in this field. Behavioural therapy proved to be useful in cases of
punishment, risky behaviour etc.) are counted as symptoms which are included into the diagnosis.

 inattentiveness but also aggressive behaviour (Petermann et al. 2002). Likewise, family
therapy is successful: the establishment of a clear educational standpoint of the parents
reduces hyperactive reactions significantly (Hüther, Bonney 2002). For the aggressive
elements and disorders in social behaviour mostly involved, other methods can be useful
(Cognitive skills programs: ATV (anti-aggression-training), trainig of social competences
ergotherapy). The main focus is on the measures for the improvement of attention and the
control and direction of behaviour. The aim is the mastering of coping strategies, the
management of symptoms and situations. It is important to develop useful techniques in the
dealing with the impairment, to learn to control behaviour.
The prognosis is better the earlier the effective treatment starts. Therefore, an early
involvement of family and schoolis necessary. If however hindering social factors are added,
further social risk factors, the social prognosis is unfavourable. Comorbid factors such as
aggressiveness and dissocial behaviour but also a failed treatment worsen the prognosis. It has
to be considered that ADHD is only one of many risk factors for the social development of
An effective therapy requires an intense cooperation of school, parents, psychologists,
trainers, legal authorities, police, social services and others – a cooperation, in which none of
the institutions is experienced. Problems like data protection and professional duty to maintain
confidentiality might make an effective cooperation difficult.
What can be done in a place of detention to improve the situation of those concerned? Which
treatments can be offered? In the Chen, first experiences in the dealing
with ADHD clients were made in a ergotherapy course. Furthermore, there is a course for the
training of social competences (Fit for Life). The treatment itself is merely symptomatic.
What can be done beside medication is mainly concerning management, the coping with
symptoms and situations. It is important for the youths to learn to deal with the impairment.
The purchase of a punchbag for example proved to be a good investment to ‘let off steam’.
5 For the different programs of violence prevention, especially applied in the field of school, see Schick, Ott 2002.
6 The Chance project is runnig from 01.11.2000-31.12.2004 and is supported by the senator for labour, women, health, youth and social services, the European Community (main emphasis 10: qualification in the penal system), the job centres of Bremen and Bremerhaven as well as the senator of justice. The responsible body is JUDIT Bremen for the place of detention in Bremen. See Matt 2003, http://www.chance.uni-bremen.de.
inattentiveness but also aggressive behaviour (Petermann et al. 2002). Likewise, family
therapy is successful: the establishment of a clear educational standpoint of the parents
reduces hyperactive reactions significantly (Hüther, Bonney 2002). For the aggressive
elements and disorders in social behaviour mostly involved, other methods can be useful
(Cognitive skills programs: ATV (anti-aggression-training), trainig of social competences
ergotherapy). The main focus is on the measures for the improvement of attention and the
control and direction of behaviour. The aim is the mastering of coping strategies, the
management of symptoms and situations. It is important to develop useful techniques in the
dealing with the impairment, to learn to control behaviour.
The prognosis is better the earlier the effective treatment starts. Therefore, an early
involvement of family and schoolis necessary. If however hindering social factors are added,
further social risk factors, the social prognosis is unfavourable. Comorbid factors such as
aggressiveness and dissocial behaviour but also a failed treatment worsen the prognosis. It has
to be considered that ADHD is only one of many risk factors for the social development of
An effective therapy requires an intense cooperation of school, parents, psychologists,
trainers, legal authorities, police, social services and others – a cooperation, in which none of
the institutions is experienced. Problems like data protection and professional duty to maintain
confidentiality might make an effective cooperation difficult.
What can be done in a place of detention to improve the situation of those concerned? Which
treatments can be offered? In the Chen, first experiences in the dealing
with ADHD clients were made in a ergotherapy course. Furthermore, there is a course for the
training of social competences (Fit for Life). The treatment itself is merely symptomatic.
What can be done beside medication is mainly concerning management, the coping with
symptoms and situations. It is important for the youths to learn to deal with the impairment.
The purchase of a punchbag for example proved to be a good investment to ‘let off steam’.
5 For the different programs of violence prevention, especially applied in the field of school, see Schick, Ott 2002.
6 The Chance project is runnig from 01.11.2000-31.12.2004 and is supported by the senator for labour, women, health, youth and social services, the European Community (main emphasis 10: qualification in the penal system), the job centres of Bremen and Bremerhaven as well as the senator of justice. The responsible body is JUDIT Bremen for the place of detention in Bremen. See Matt 2003, http://www.chance.uni-bremen.de.

 The participants are instructed to control and work off their impulses this way. It is a long-
term training aspect: They learn to realize, when they should rather get out of a situation.
Other instructive, directive treatments have proven useful (training methods, perceptual
training, sociotherapy). Other forms of producing concentration may also come into effect.
The establishment of computerbased learning for instance was found to be successful.
Appropriate assisting measures still have to be developed and offered. Further appliccable
therapies are being searched for in order to gain experience with the realization and the
adaption. Facing a long period of experiencing the failure of ADHD patients, it is especially
important to give them a sense of achievement for them to strengthen their self-esteem.
ADHD and delinquency
The participants are instructed to control and work off their impulses this way. It is a long-
term training aspect: They learn to realize, when they should rather get out of a situation.
Other instructive, directive treatments have proven useful (training methods, perceptual
training, sociotherapy). Other forms of producing concentration may also come into effect.
The establishment of computerbased learning for instance was found to be successful.
Appropriate assisting measures still have to be developed and offered. Further appliccable
therapies are being searched for in order to gain experience with the realization and the
adaption. Facing a long period of experiencing the failure of ADHD patients, it is especially
important to give them a sense of achievement for them to strengthen their self-esteem.
ADHD and delinquency 

 compensation mechanisms on the part of those concerned, as well as the negative reactions on
the part of the social environment. The model of development as a diagram:
DIAGRAM (Possible outcoume of untreated ADHD)
Consequently, it is important to develop appropriate offers, which make it possible to master
those deviances in behaviour. Appropriate practices in the dealing with the impairment have
to be communicated. Medication alone would at most make security and order easy in the
ward, but it would not do anything for the patient himself. Appropriate pedagogical and
therapeutical support has to be developed.
Especially for those deviant youths with long careers of delinquency, an increased
cooperation of the penal institution with psychologists and psychiatrists seems to be required.
A distinction of exclusive offers, especially for this group, is needed. The developing risk of
stigmatization has to be opposed. Juvenile prisoners react very intensely on terms like
psychologically disturbed or disabled. Thus, a reconsideration is required. Aspects of the
biographical and social situation as well as the emotional, cognitive and social competence (as
well as the compensation strategies therefore developed) are to be involved into the therapy
process as conditions. Only a qualified, differentiating diagnosis and an improved awareness
of the difficulties can lead to adequate modes of reaction, can make it possible to fulfil the
compensation mechanisms on the part of those concerned, as well as the negative reactions on
the part of the social environment. The model of development as a diagram:
DIAGRAM (Possible outcoume of untreated ADHD)
Consequently, it is important to develop appropriate offers, which make it possible to master
those deviances in behaviour. Appropriate practices in the dealing with the impairment have
to be communicated. Medication alone would at most make security and order easy in the
ward, but it would not do anything for the patient himself. Appropriate pedagogical and
therapeutical support has to be developed.
Especially for those deviant youths with long careers of delinquency, an increased
cooperation of the penal institution with psychologists and psychiatrists seems to be required.
A distinction of exclusive offers, especially for this group, is needed. The developing risk of
stigmatization has to be opposed. Juvenile prisoners react very intensely on terms like
psychologically disturbed or disabled. Thus, a reconsideration is required. Aspects of the
biographical and social situation as well as the emotional, cognitive and social competence (as
well as the compensation strategies therefore developed) are to be involved into the therapy
process as conditions. Only a qualified, differentiating diagnosis and an improved awareness
of the difficulties can lead to adequate modes of reaction, can make it possible to fulfil the

 Literatur:
Literatur: