Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
«datel»
To enable us to organise an appropriate appointment for you we ask that you complete the enclosed Patient Detail Questionnaire and return to our office as soon as possible. If not previously forwarded, please include the following:
• X-Ray or Scan Reports (Films are not required at this point)
Please bring your films on the day of your appointment
The above forms can be mailed, faxed or emailed to our office. Current address:
The information received will be reviewed by Dr Albietz and we will contact you by mail within 7 working days with an appointment date and time. Thank you for your understanding and co-operation. If you have any further questions please do not hesitate to contact our office on 07 3721 8600.
DATE: ____/____/ ____ Title: Mrs Miss Ms Mr Mast Dr Family Name: Given Name: Address: Date of Birth: ____/____/___ Occupation: Email: Ph: (h)
Medicare Reference Number (Small Number in front of your name):
Dept Of Veteran Affairs No: Exp: / / Gold Card / White Card Health Care Card / Pension No:
Are you a member of a Private Health Fund:
Health Fund: Membership No: Level of Cover (Please tick):
Have you served the 12 month waiting period
ACCOUNT PAYMENT DETAILS
Self Workcover Claim No: REFERRAL DETAILS Referring Doctor Name: Address: Usual GP (If different from referring doctor) Address: NEXT OF KIN DETAILS Next of Kin:
Address: Phone: PATIENT CONSENT I give permission for you to disclose to any doctor, health authority, allied health provider, rehabilitation provider, Workcover Insurer and its agents, or other insurer any information about my medical history relevant to my treatment. Signature: X-RAYS QCOS Orthopaedic does not store x-rays / scans for any period of time exceeding twelve months. It is essential that you keep the scans in your possession at all times. I hereby understand that the QCOS Orthopaedic will destroy any x-rays or scans left in their possession after twelve months, without prior notice. Signature:
Patient Health Questionnaire
1. Do you have a history of: Please specify:
Deep Vein Thrombosis (DVT) Yes No
Do you have a family history of DVT or PE
Arthritis (Osteo, Rheumatoid, Gout etc) Yes No
2. Please list any current or previous medical problems. 3. Have you had any previous operations? Operation When (Year) 4. Are you taking any of the following medications? If yes, please discuss with your doctor
• Plavix, Clopidgrel, Wafarin, Aspirin, Cartia
5. Please list all other medications. Medication: eg Panadol Dose: eg1 gram Frequency: eg 4 per day Route: capsule 6. Please list any allergies Medication / Substance Reaction 7. Have you had any previous back/neck complaints: 1.________________________________________________________________________________________________ 2.________________________________________________________________________________________________ Do you have a current legal claim regarding this condition?
Are you seeing a Solicitor for this condition?
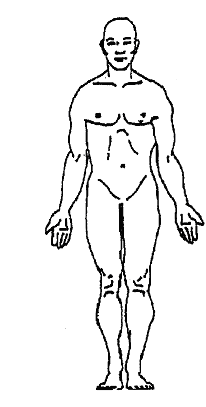
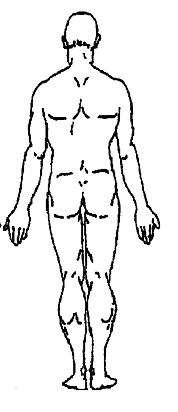
Please indicate on this diagram where your pain is located. Mark areas of pain using shading. Mark areas of tingling or pins and needles with crosses.
Please mark your current level of back pain on the scale below.
0 is no pain and 10 is the worst pain imaginable. |___|___|___|___|___|___|___|___|___|___| 0 1 2 3 4 5 6 7 8 9 10 Please mark your current level of leg pain on the scale below.
0 is no pain and 10 is the worst pain imaginable. |___|___|___|___|___|___|___|___|___|___| 0 1 2 3 4 5 6 7 8 9 10
This questionnaire has been designed to give the doctor information about how your back pain has affected your ability to manage in everyday life. Please answer each section and mark only one box per section that applies best to you. We realise that you may consider that two of the statements may apply to you, but please only mark the box that best describes your problem. Back Pain Questionnaire Pain Intensity Standing
I can tolerate the pain without having to use pain killers
The pain is bad but I manage without taking pain killers
I can stand as long as I want but it gives me extra pain
Pain killers give complete relief of pain
Pain prevents me from standing more than one hour
Pain killers give partial relief of pain
Pain prevents me from standing more than 30 minutes
Pain killers give very little relief of pain
Pain prevents me from standing more than 10 minutes
Pain killers have no effect on pain and I do not use them
Personal Care Sleeping
I can look after myself normally without extra pain
I can look after myself normally but it causes extra pain
It is painful to look after myself and I am slow and careful
Pain interrupts my sleep half of the time
I need some help but manage most of my personal care
I need help every day in most aspects of personal care
I do not get dressed, wash with difficulty and stay in bed
Social Life
I can lift heavy objects without extra pain
My social life is normal and gives me no extra pain
I can lift heavy objects but it gives extra pain
My social life is normal but gives me extra pain
I can only lift heavy objects if they are on a table
Pain restricts more energetic social activities
I can only lift light / medium objects if they are on a table
Pain has restricted my social life and I go out less often
Pain has restricted my social life to home
Travelling
I can travel anywhere without extra pain
I can walk comfortably but running is painful
I can travel anywhere but it causes some pain
Pain prevents me from walking more than one hour
Pain is bad but I manage to travel over two hours
Pain prevents me from walking more than 30 minutes
Pain restricts me to trips of less than one hour
Pain prevents me from walking more than 10 minutes
Pain restricts me to trips of less than 30 minutes
I cannot walk more than a few steps at a time
Pain prevents me from travelling except to the doctor
Employment / Housekeeping
I can sit in any chair as long as I want
My normal homemaking/ job activities don’t cause pain
I can only sit in a special chair as long as I want
I can perform all these activities but do experience pain
Pain prevents me from sitting more than one hour
I can perform most activities but do experience pain
Pain prevents me from sitting more than 30 minutes
Pain prevents me from doing anything but light duties
Pain prevents me from sitting more than 10 minutes
Pain prevents me from doing even light duties
Pain prevents me performing any job/ activities at all
Office Use Only _______/_______ _________%
Height: (cm) Weight (kg) What date did the injury occur? How did the injury occur? Have you had any previous treatment with regards to this injury? Eg: Physiotherapy, Chiropractic, Occupational Therapy, Psychology, Injections, Pain Medication, Acupunctureetc. If you have had any of the above treatment, when did it commence and how often have you been having treatment? Have you seen any other Specialists with regards to this injury?
Have you had any x-rays, CT scans or MRI’s taken with regards to this injury?
Please list the tests that you have had:
Are you currently working?
WorkCover Patients Only WorkCover Claim No:
WorkCover Claim Manager:
Employer Name:
Employer Phone No: Before this accident, did you have any condition or injury that affected this part of your body? Have you had any other previous WorkCover claims?
WorkCover Patients Only Important Information It is very important that your WorkCover Medical Certificates are kept up to date at all times. Please request a new certificate from your doctor at each appointment, if required. Your consultations will only be paid by WorkCover if they hold a current Medical Certificate. It is the patient’s responsibility to give a copy of the Medical Certificate to WorkCover and the Employer. This certificate is also to be given to anyone that is providing treatment eg: Physiotherapist, Chiropractic, Occupational Therapist, Hand Therapist etc A current referral must be held by our office at all times. Medical Certificates will not be issued over the phone. Signature: Date:
What is influenza? Influenza is an infectious illness caused by a virus. It is primarily spread from person to person by the aerosol route, via inhalation of droplets formed during coughing and sneezing, or by direct contact with articles contaminated with respiratory secretions. Influenza usually begins abruptly and can include fever, chills, fatigue, headache, muscle aches, non-productive
Ginseng gibt Kraft - Vor 90 Jahren eröffnete Otto Teetzen in Nowawes die Plantagen- Apotheke Über Arsen, Fragen zum Atomunfall in Japan, die Konkurrenz im Internet und schlaflose Nächte sprach die Chefin Antje Oesberg mit Carola Hein. Antje Oesberg (lacht): Weder Pillen noch Zäpfchen. Von der Romantik des Apothekerberufs ist heute nicht mehr viel übrig. Nach der Wende hat sich Alles wir