Human Reproduction Vol.18, No.4 pp. 700±706, 2003
The number of antral follicles in normal women with
proven fertility is the best re¯ection of reproductive age
G.J.Scheffer1,6, F.J.M.Broekmans1, C.W.N.Looman2, M.Blankenstein3, B.C.J.M.Fauser4,
F.H.deJong5 and E.R.teVelde11Department of Reproductive Medicine, Division of Perinatology and Gynecology, University Medical Center Utrecht, 2Department
of Public Health, Faculty of Medicine, Erasmus University, Rotterdam, 3Department of Clinical Chemistry, Free University Medical
Center, Amsterdam, Division of Reproductive Medicine, 4Department of Obstetrics and Gynecology and 5Department of Internal
Medicine III, Erasmus University Medical Center, Rotterdam, The Netherlands6To whom correspondence should be addressed at: Department of Reproductive Medicine, Division of Perinatology and Gynecology,
University Medical Center Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The Netherlands. E-mail: [email protected]
BACKGROUND: The purpose of this study was to compare the predictive capacity of several markers of repro-
ductive age in normal women. METHODS: Healthy female volunteers (n = 162) aged 25±46 years with proven,
normal fertility and regular menstrual cycles were recruited. In this selected group, chronological age was assumed
to approximate reproductive age and, therefore, was taken as the proxy-variable for reproductive age. The number
of antral follicles with 2±10 mm diameter, total ovarian volume, total follicular volume, mean follicular volume, and
volume of either the smallest or largest ovary were estimated by transvaginal sonography of the ovaries. Serum
levels of early follicular FSH, estradiol and inhibin B, as well as the response of estradiol and inhibin B to exogenous
GnRH agonist administration (GAST), were also evaluated. RESULTS: Regression analysis revealed that the antral
follicle number showed the highest correlation with age (r = ±0.68, P = 0.001), and explained 46% of its variance. All
other variables, except inhibin B, were moderately correlated with age. Responses of estradiol and inhibin B to the
GnRH agonist were moderately correlated with age, but highly correlated with the number of antral follicles.
CONCLUSIONS: It is concluded that the number of antral follicles has the closest association with chronological
age in normal women with proven fertility. As stimulated estradiol and inhibin B clearly re¯ect the size of the antral
follicle cohort, the GAST may be considered the second best single test to predict reproductive age.
Key words: antral follicles/GnRH agonist stimulation test/inhibin B/reproductive ageing/transvaginal sonography
Corson et al., 1999; Hall et al., 1999; Creus et al., 2000),
Delaying the period in life to have children considerably
estradiol (E2) (Evers et al., 1998; Mikkelsen et al., 2001) and
contributes to the proportion of couples with involuntary
the E2 and inhibin B response to exogenous GnRH agonist
childlessness (Mosher et al., 1991). Demographic (Wood,
(GAST) (Winslow et al., 1991; Avrech et al., 1996; Galtier-
1989) and clinical (Noord-Zaadstra et al., 1991) studies have
Dereure et al., 1996; Ranieri et al., 1998; Ravhon et al., 2000)
shown that a woman experiences her optimal fertility before
or FSH stimulation (EFORT) (Fanchin et al., 1994; Dzik et al.,
the age of 30±31 years. Thereafter, fertility gradually
2000; Fabregues et al., 2000; Elting et al., 2001) have all been
decreases, with an acceleration towards the age of 40 years.
mentioned in the literature to predict declining fertility related
Already at an age of 40±41 years half of the women will have
to reproductive ageing. Most of these studies were performed
completely lost their capacity for reproduction. It is generally
in infertility populations, using pregnancy rates or response to
accepted that reproductive ageing is in fact ovarian ageing and
ovarian hyperstimulation in IVF as outcome measures.
is related to the decreasing quantity and quality of the pool of
However, the establishment of a pregnancy is in¯uenced by
follicles preserved in the ovary (Seifer et al., 1996; teVelde and
many more, partly unknown, factors. To what extent ovarian
ageing per se contributes to the reproductive failure of an
The number of antral follicles and the total ovarian volume
individual couple remains a matter of speculation.
as measured by transvaginal ultrasound (Lass et al., 1997;
Studies concerning physiological ovarian ageing in women
Tomas et al., 1997; Chang et al., 1998; Ng et al., 2000; Bancsi
without fertility problems have only been performed in a
et al., 2002), basal FSH (Muasher et al., 1988; Scott et al.,
limited number of relatively young women (Schipper et al.,
1990; Bancsi et al., 2000), inhibin B (Seifer et al., 1997;
1998) or have compared small groups of relatively aged
ã European Society of Human Reproduction and Embryology
Antral follicle number re¯ects reproductive age
Table I. Median values and ranges of endocrine and sonographic characteristics in the three age categories
aMedian values of the old age group differed signi®cantly from the young age group.
bMedian values of the middle age group differed signi®cantly from the young age group.
cMedian values of the old age group differed signi®cantly from the middle age group.
Range values are given in parentheses.
women with very young controls (Klein et al., 1996a,b). It
perpendicular measurements depending on the diameter (`6 or >6
therefore seems warranted to evaluate the aforementioned
mm). The volume of each follicle was calculated by applying the
sonographic and hormonal test parameters in a large group of
equation of the volume of an ellipsoid (LQWQDQp/6). By adding all
normal women of different ages with proven natural fertility.
volumes of follicles up to 10 mm in size in both ovaries, the total
Since such women are likely to represent the age-related
follicular volume was obtained (Haning et al., 1982). Mean follicular
decline of the reproductive potential in the normal population,
volume was calculated by dividing the total follicular volume by the
number of follicles counted. The volume of the left and right ovary
the assumption that their chronological age approximates
was assessed by measuring the diameter of the ovarian contour in three
reproductive age seems justi®ed. Chronological age, therefore,
perpendicular directions and applying the equation for the volume of
was used as the outcome variable to identify, ®rst, those factors
an ellipsoid (D1QD2QD3Qp/6) to calculate ovarian volume. Total
that show the best correlation with age, second, to obtain
ovarian volume was then obtained by summing the volume of the left
insight into how the various predictive parameters correlate
and right ovary. Intra- and inter-observer variations of the antral
with one another, and third, whether or not one or more
follicle count and ovarian volume assessment have been published
variables would improve the predictive performance of the best
Endocrine testingBlood sampling was performed on the same day as the sonography
examination. Hormone concentrations were measured in plasma (E2
This study was approved by the local Ethics Committee and written
and FSH) and serum (inhibin B). Specimens were stored at ±20°C until
informed consent was obtained from all participants. Healthy female
processing. A random subgroup of 40 women underwent a GnRH
volunteers (n = 162, age range 25±46 years) were recruited by
agonist stimulation test in the cycle subsequent to the one in which the
advertisement in the local newspapers. Women were enrolled in the
basal endocrine and ultrasound characteristics were measured. A
study protocol if they met all of the following criteria: (i) regular
single s.c. injection of 100 mg of triptorelin (Decapeptyl; Ferring,
menstrual cycles varying from 21 to 35 days, (ii) a biphasic body
Hoofddorp, The Netherlands) was administered at day 3 of the cycle
temperature chart, (iii) proven natural fertility by having had at least
(Ranieri et al., 1998). Blood samples were taken immediately before
one pregnancy carried to term, (iv) each of their pregnancies arisen
and 24 h after GnRH agonist administration. The administered dose is
spontaneously within 1 year after the start of unprotected intercourse,
assumed to provide maximal stimulation of the pituitary with mean
(v) no evidence of endocrinological disease, (vi) no history of ovarian
peak levels of 52 IU/l for LH and 25 IU/l for FSH at 4 h after the
surgery, (vii) no ovarian abnormalities as assessed by transvaginal
injection and LH levels of 12.0 IU/l and FSH levels of 10.3 IU/l after
ultrasound and (viii) hormonal contraception stopped b2 months
24 h (Broekmans et al., 1993). E2 concentrations were assayed with a
before entering the study protocol. For study participation the
microparticle enzyme immunoassay (MEIA) purchased from Abbott
volunteers received monetary compensation.
Laboratories (Abbott Park, IL, USA) and using a semi-automated IMx
analyser. Between-run coef®cients of variation (CV) for E2 were 10.1,
7.0 and 6.9% at 533, 1354 and 4197 pmol/l respectively (n = 49, 49
Transvaginal sonography of the ovaries was carried out on cycle day
and 30). Concentrations of FSH were measured with the use of the
1, 2, 3 or 4. All sonography measurements were performed by the
MEIA technology on a fully automated AxSYM immunoanalyser
same observer (G.S.) using the 7.5 MHz transvaginal probe on a
(Abbott Laboratories) according to the manufacturer's instructions.
Toshiba Capasee SSA-220A (Toshiba Medical Systems Europe BV,
All specimens of each volunteer were analysed in the same run. The
Zoetermeer, The Netherlands). Examination of the ovary was
standard of the FSH assay was referenced against the World Health
established by scanning from the outer to the inner margin (Pache
Organization Second International Reference Preparation for human
et al., 1990; van Santbrink et al., 1995). All follicles 2±10 mm in size
FSH (78/549). The between-run CV of the FSH assay was 6.0, 6.6 and
were measured and counted in each ovary. The sum of both counts was
8% at levels of 5.0, 25 and 75 IU/l (n = 46). Inhibin B levels were
the antral follicle count. Follicle size was calculated from two or three
measured using an immuno-enzymometric assay (Serotec, Oxford,
Table II. Correlation matrix of basal endocrine and ultrasound parameters. (Total group, n = 162)
Smallest ovary volume (small) ±0.24* ±0.10
Total follicular volume (TFV) ±0.36* ±0.17* 0.40* 0.69* 0.47* 0.42* 0.44*
0.25* 0.29* ±0.12 ±0.68* ±0.30* ±0.26* ±0.21* ±0.34* 0.37*
were determined in a stepwise fashion after controlling for the effect
of variables having the strongest correlation with chronological age in
previous steps. The square of the correlation of a variable with
chronological age was calculated as a re¯ection of the fraction of
variation of chronological age explained by this variable and was
considered a direct measure of its predictive performance. The
additional predictive effect of the subsequent variables, after the best
one had been selected, was calculated by multiplying the squares of
the partial correlations with the remaining unexplained fraction.
For all statistical analyses, P < 0.05 was considered as signi®cant.
Figure 1. Dendrogram based on agglomerative cluster analysis. The
Median values and ranges of the various endocrine and
correlation between variables can be estimated from this ®gure by
sonographic parameters for the three age groups are given in
looking for the vertical line that connects the branches. For
Table I. Values of all variables in the old age group differ
example, the correlation between total ovarian volume and volume
of largest ovary is ~0.95. TOV = total ovarian volume; TFV = total
signi®cantly from those of the young group (except inhibin B)
follicular volume; AFC = no. of follicles; InhB = inhibin B;
and from those of the middle group (except E2, inhibin B and
E2 = estradiol; MFV = mean follicular volume.
FSH). The number of follicles is the only variable for which
values in the middle age group also signi®cantly differ from
those of young women. Both the numbers of antral follicles and
UK) (Groome et al., 1996). Intra- and inter-assay CV for the inhibin B
assay were <14.6 and <14.0% respectively.
the total follicular volume decrease with increasing age.
However, the decrease of total follicular volume is less steep
than that of the follicle number, while the mean volume per
Statistical analysis was performed by using SPSS (Statistical Package
follicle increases as a woman grows older and almost doubles
for Social Sciences) for Windows (release 6.1.3) and GLIM
in the old age group as compared with the young age group.
(Generalized Linear Interactive Modelling; NAG, Oxford, UK). For
The correlation matrix (Table II) should be interpreted in
the study group as a whole, three age groups were distinguished: a
conjunction with Figure 1. Volumes of the smallest, the largest
young group of women aged <35 years, an old group of women aged
and both ovaries are highly correlated, indicating that they will
>40 years and a middle group of women with ages in between.
provide almost the same information. Therefore, in subsequent
Responses of inhibin B and E2 in the GAST group were de®ned as the
analyses only one of themÐtotal ovarian volumeÐis taken
serum or plasma level 24 h after GnRH agonist (cycle day 4 value)
into account. The correlation between follicle number and total
minus the baseline level before GnRH agonist was injected (cycle day
follicular volume is also strong (r = 0.69), while the mean
3 value). Comparison between subgroup variables was performed by
volume per antral follicle increases with age (r = 0.37). The
the Mann±Whitney U-test or the Wilcoxon signed rank test, when
sonographic variables, except mean follicular volume, together
appropriate. The correlations between age, the various endocrine and
form one cluster, in which correlation between the ovarian
the sonographic parameters in the total group as well as in the GAST
volume cluster and the follicle cluster is between 0.4 and 0.5
group were presented as a correlation matrix. In addition, in the total
group an agglomerative cluster analysis on the absolute values of the
(Figure 1). The interrelationship between the endocrinological
correlations was performed, in order to visualize the strength of
parameters is less clear-cut. One cluster is formed by inhibin B
correlations between two variables, and to obtain better insight into
and FSH, con®rming their rather strong and inverse correlation
(r = ±0.40). E2 and mean follicular volume also form one,
Using linear regression, univariate correlations of all variables with
positively correlated cluster, which is in line with the positive
chronological ageÐthe outcome variable in this studyÐwere
correlation of both E2 and mean follicular volume with age
calculated for the total group. Subsequently, partial correlations
Antral follicle number re¯ects reproductive age
Table III. Correlations of the endocrine and sonographic variables with
Table IV. Baseline levels, stimulated levels and responses for inhibin B
chronological age. (Total group, n = 162)
and estradiol in the exogenous GnRH agonist administration group (n = 40)
Estradiol (pmol/l) 187 (51±462) 536 (9±1163) 276 (±11±994) 0.001
aWilcoxon signed rank test, baseline versus stimulated levels.
Step 1: univariate correlations; step 2: partial correlations controlling for the
for basal inhibin B. Moreover, E2 and inhibin B responses are
number of follicles; step 3: partial correlations controlling for the number of
clearly better correlated with antral follicle number (r = 0.75
follicles and total follicular volume.
and 0.73 respectively) than with age (r = ±0.42 and ±0.44
respectively). Finally, E2 and inhibin B responses are
The results of the univariate and partial correlations of the
endocrine and sonographic variables with age are shown in
Table III. Number of follicles shows the best correlation with
age (r = ±0.68). In contrast, the correlation of inhibin B with
In this study we showed that the number of antral follicles
age was weak and did not reach statistical signi®cance. The
2±10 mm in diameter, as measured by vaginal sonography
correlations of the remaining variables were all highly
during the early follicular phase, appeared to have the best
signi®cant (P < 0.001). Only E2, total follicular volume and
correlation with chronological age in a carefully selected group
mean follicular volume appeared to have a statistically
of women who had regular cycles and proven normal fertility.
signi®cant correlation with age which was independent from
In such women the age-dependent changes of ovarian function
the number of antral follicles (step 2). After controlling for
are likely to re¯ect the physiological decline of female
both number of follicles and total follicular volume, E2
fecundity. Hence, their chronological age can be assumed to
continued to have a signi®cant, independent correlation with
be a better approximation of reproductive age than that of
age (step 3). Other partial correlations lost statistical signi®-
women who suffer from infertility which may be associated
cance in the next step (results not shown). The variation in
with accelerated reproductive ageing. We realize, however,
chronological age is explained for 46% by the best predictive
that such an approximation is not perfect, because also in
variable, the number of follicles. When adding the two
normal fertile women of the same chronological age, variations
independent predictive variables in a stepwise fashion, the
in reproductive status may be present. However, we are not
explained variation rose ®rst by 3% after the selection of total
aware of a better `gold standard' for the process of reproductive
follicular volume and by another 2% after the selection of E2.
The total explained variation thus increased from 46 to 51%.
It is generally accepted that reproductive ageing is directly
Values of age and the basal endocrine and ultrasound
related to the remains of the stock of primordial follicles, which
variables studied in the GAST group did not differ from those
is established during fetal life. This pool progressively empties
in the remaining group (data not shown). Baseline levels, levels
as a woman grows older and is (almost) completely exhausted
after GnRH agonist stimulation and the corresponding
when menopause is reached (Faddy et al., 1992). In a previous
responses of inhibin B and E2 in the GAST group are shown
study we showed that the pattern of age-dependent loss of
in Table IV. The rise in hormone levels after the GnRH agonist
antral follicle numbers is strikingly similar to that of the
stimulation was statistically signi®cant for both hormones.
primordial follicle pool (Scheffer et al., 1999). It seems
Correlations of age and the investigated hormones and
plausible, therefore, that the number of antral follicles, as
hormonal responses as well as the ultrasound variables are
assessed by sonography, re¯ects what is left of the primordial
shown in the correlation matrix (Table V). Note that the
follicle pool and, thus, the reproductive age of an individual
correlations among age and the endocrine and ultrasound
baseline variables are in the same order as for the total group
The number of antral follicles correlated much better with
(Table II), with the exception that the correlation for inhibin B
the age of the women evaluated in this study, than other
with antral follicle count seems more favourable, presumably
presumed basal markers for reproductive age, including FSH,
due to chance variation. The weak or statistically non-
inhibin B, E2 and ovarian volume. As expected, total follicular
signi®cant correlations for baseline levels of inhibin B and
volume appeared to be a simple derivative from number of
E2 with age are changed into more robust and signi®cant
follicles, evidenced by a strong and positive correlation with
correlations when the response in the GnRH agonist test is
numbers of follicles (r = 0.69) and a negative correlation with
considered (Tables II and IV). Baseline levels of inhibin B
reproductive age (r = ±0.34). We were surprised, however, to
show a statistically signi®cant correlation with antral follicle
®nd that the mean follicular volume considerably increased
numbers. However, the correlations with the number of antral
with age and had almost doubled in the old age group in
follicles of the E2 and inhibin B responses after GnRH agonist
comparison with the young ones. The correlation of mean
stimulation become highly signi®cant and clearly stronger than
follicular volume, a derivative of the total follicular volume
Table V. Correlation matrix of basal endocrinological and ultrasound parameters in the exogenous GnRH
agonist administration (GAST) group (n = 40)
and the number of follicles, with age, therefore, is positive (r =
Although the number of antral follicles in both ovaries
0.37). E2 levels are also positively correlated with age.
appeared to have the best correlation with chronological age,
Apparently, the few antral follicles which are still present in
basal E2 and total follicular volume slightly improved the
the early follicular phase in older aged women, are not only
prediction already obtained with the antral follicle count.
larger but also produce more E2 than the many, but smaller,
Apparently, the predictive information provided by FSH,
antral follicles present at a younger age. Several studies have
inhibin B and total ovarian volume is already covered by the
shown that the follicular phase of the menstrual cycle in older
number of follicles. Nevertheless, 90% of the explained
aged women becomes considerably shorter (Lenton et al.,
variance of age is already obtained with the number of follicles
1984; Klein et al., 1996a; van Zonneveld et al., 2003). This
alone, while the additional contributions of total follicular
phenomenon has been postulated as suggesting accelerated
volume and E2 are 6 and 4% respectively. Such an improve-
growth of antral follicles in older women (Klein et al., 1996a).
ment in predictive performance seems almost negligible.
Since the diameter on the day of ovulation and the mean
Therefore, the use of antral follicle counts as a single test to
follicular growth per day were almost the same in older and
predict the response to controlled ovarian stimulation and the
younger women (van Zonneveld et al., 2003), we suggest that
probability of pregnancy in assisted reproduction seems
follicular development in older women is not accelerated but
rational. Several studies have analysed the usefulness of antral
advanced. Dominant follicle growth in older women is likely to
follicle counts in this respect. In a study of IVF patients (Tomas
have started already in the luteal phase of the previous cycle
et al., 1997) it was shown that the ovarian responsiveness is
before menstruation starts. This earlier start of development is
dependent on the number of small antral follicles (2±5 mm). In
in accordance with data from the literature, indicating that the
another study, patients with an antral follicle (2±8 mm) count
intercycle FSH rise is not only higher, but also starts earlier in
of less than four appeared to have a signi®cantly higher rate of
older women (Klein et al., 1996a; van Zonneveld et al., 2003).
cancellation due to poor response and no pregnancies occurred
Advanced development of follicular growth fully explains why
in this group of patients (Chang et al., 1998). In several studies,
at the onset of the menstrual cycle, antral follicles are larger
logistic regression analysis has shown that the number of antral
and, though lower in number, produce higher E2 levels in older
follicles is a signi®cant predictor for the occurrence of poor
ovarian response in IVF with an adequate balance between test
While numbers of follicles already have clearly decreased in
sensitivity and speci®city (Frattarelli et al., 2000; Pohl et al.,
the middle-aged, hormone levels of FSH, E2 and inhibin B only
2000; Dumesic et al., 2001; Hsieh et al., 2001; Huang et al.,
become notably changed in women aged >40 years.
2001; Bancsi et al., 2002). Most studies, however, also
Apparently, age-dependent hormonal changes are a relatively
revealed that pregnancy prediction from antral follicle counts,
late phenomenon and only occur when follicle numbers are
even in combination with other ovarian reserve factors,
greatly reduced (te Velde and Pearson, 2002). This conclusion
is in line with the results of several studies in normal
It was shown that after the administration of a high dose of
volunteers. Neither maximum FSH and inhibin B concentra-
GnRH agonist, antral follicles greatly increase their production
tions in the follicular phase nor cycle day 3 FSH levels were
and release of E2 and inhibin B from the granulosa cells within
correlated with age in normally cycling, female volunteers
24 h. This ®nding is not new for E2 (Winslow et al., 1991;
aged 20±35 years (Schipper et al., 1998). A study in young
Ranieri et al., 1998) and con®rms results from other studies
controls (aged 20±25 years) and reproductively aged women
(Avrech et al., 1996; Galtier-Dereure et al., 1996; Ravhon et al.,
(aged 40±45 years) showed that inhibin B serum levels were
2000). As E2 and inhibin B are produced from small antral
only signi®cantly lower in the reproductively aged women at
follicles present in the early follicular phase of the cycle, basal
the day of maximal FSH (Klein et al., 1996a). Finally, lower
levels would re¯ect the size of the FSH sensitive cohort of
early follicular inhibin B serum levels were only found in older
follicles. Although this may be true for inhibin B, E2 release is
cycling women compared with young controls (Welt et al.,
much more dependent on other sources such as the remnants of
1999). All this explains why the correlations of basal FSH, E2
the corpus luteum or an advanced growing follicle. Once
and inhibin B with chronological age are only weak to
stimulated by an endogenous FSH (and LH) rise in the GAST,
the relation between inhibin B and the cohort size becomes
Antral follicle number re¯ects reproductive age
magni®ed as evidenced by the improved correlation with the
Dumesic, D.A., Damario, M.A., Session, D.R., Famuyide, A., Lesnick, T.G.,
Thornhill, A.R. and McNeilly, A.S. (2001) Ovarian morphology and serum
hormone markers as predictors of ovarian follicle recruitment by
clear positive correlation with antral follicle number shows that
gonadotropins for in vitro fertilization. J. Clin. Endocrinol. Metab., 86,
the cohort as a whole contributes to the peripheral E
These ®ndings also con®rm studies in which the instant E
Dzik, A., Lambert-Messerlian, G., Izzo, V.M., Soares, J.B., Pinotti, J.A. and
inhibin B response to a single FSH dose administration
Seifer, D.B. (2000) Inhibin B response to EFORT is associated with the
outcome of oocyte retrieval in the subsequent in vitro fertilization cycle.
appeared clearly related to the number of stimulated follicles
in ovarian hyperstimulation for IVF (Fanchin et al., 1994; Dzik
Eldar-Geva, T., Robertson, D.M., Cahir, N., Groome, N., Gabbe, M.P.,
et al., 2000; Eldar-Geva et al., 2000; Elting et al., 2001).
Maclachlan, V. and Healy, D.L. (2000) Relationship between serum inhibin
A and B and ovarian follicle development after a daily ®xed dose
Moreover, the responses of E2 and inhibin B in the GAST are
administration of recombinant follicle-stimulating hormone. J. Clin.
clearly better related to the chronological age of a woman when
compared with baseline levels. This suggests that stimulated E
Elting, M.W., Kwee, J., Schats, R., Rekers-Mombarg, L.T. and Schoemaker, J.
and inhibin B may well re¯ect the quantitative process of
(2001) The rise of estradiol and inhibin B after acute stimulation with
follicle-stimulating hormone predict the follicle cohort size in women with
reproductive ageing. As the antral follicle count is the best
polycystic ovary syndrome, regularly menstruating women with polycystic
re¯ection of reproductive age when basal tests are considered,
ovaries, and regularly menstruating women with normal ovaries. J. Clin.
and at the same time is highly correlated with the E
Evers, J.L., Slaats, P., Land, J.A., Dumoulin, J.C. and Dunselman, G.A. (1998)
inhibin B response in the GAST, the question arises whether
Elevated levels of basal estradiol-17beta predict poor response in patients
the GAST may be a superior test in the prediction of outcome
with normal basal levels of follicle-stimulating hormone undergoing in vitro
in assisted reproduction treatment. Back-to-back comparison
fertilization. Fertil. Steril., 69, 1010±1014.
with antral follicle count has not been published in the
Fabregues, F., Balasch, J., Creus, M., Carmona, F., Puerto, B., Quinto, L.,
Casamitjana, R. and Vanrell, J.A. (2000) Ovarian reserve test with human
literature so far. As yet it cannot be expected that the accuracy
menopausal gonadotropin as a predictor of in vitro fertilization outcome.
of the test in the prediction of outcome in IVF will reach a level
J. Assist. Reprod. Genet., 17, 13±19.
of supremacy that justi®es the increased burden put on the
Faddy, M.J., Gosden, R.G., Gougeon, A., Richardson, S.J. and Nelson, J.F.
(1992) Accelerated disappearance of ovarian follicles in mid-life:
implications for forecasting menopause. Hum. Reprod., 7, 1342±1346.
In summary, in the prediction of chronological age in normal
Fanchin, R., de Ziegler, D., Olivennes, F., Taieb, J., Dzik, A. and Frydman, R.
women, the number of antral follicles appeared to be superior
(1994) Exogenous follicle stimulating hormone ovarian reserve test
to other presumed measures of reproductive ageing.
(EFORT): a simple and reliable screening test for detecting `poor
responders' in in-vitro fertilization. Hum. Reprod., 9, 1607±1611.
Additional, though modest, predictive information may be
Frattarelli, J.L., Lauria-Costab, D.F., Miller, B.T., Bergh, P.A. and Scott, R.T.
obtained from other endocrine or ultrasound variables.
(2000) Basal antral follicle number and mean ovarian diameter predict cycle
cancellation and ovarian responsiveness in assisted reproductive technology
2 and inhibin B correlated strongly with the
number of antral follicles and therefore may provide the same
cycles. Fertil. Steril., 74, 512±517.
Galtier-Dereure, F., De Bouard, V., Picot, M.C., Vergnes, C., Humeau, C.,
body of information on reproductive age. Whether these
Bringer, J., Hedon, B. (1996) Ovarian reserve test with the gonadotrophin-
®ndings will help us to assess the reproductive capacity in
releasing hormone agonist buserelin: correlation with in-vitro fertilization
individual subfertile women remains to be further elucidated.
outcome. Hum. Reprod., 7, 1393±1398.
Groome, N.P., Illingworth, P.J., O'Brien, M., Pai, R., Rodger, F.E., Mather,
J.P. and McNeilly, A.S. (1996) Measurement of dimeric inhibin B
throughout the human menstrual cycle. J. Clin. Endocrinol. Metab., 81,
Avrech, O.M., Royburt, M., Sabah, G., Zukerman, Z., Pinkas, H., Amit, S.,
Hall, J.E., Welt, C.K. and Cramer, D.W. (1999) Inhibin A and inhibin B re¯ect
Ovadia, J. and Fisch, B. (1996) The initial ¯are-up induced by gonadotropin
ovarian function in assisted reproduction but are less useful at predicting
releasing hormone agonist may serve as a predictor of ovarian response in
outcome. Hum. Reprod., 14, 409±415.
the current IVF±ET treatment cycle in normogonadotropic women aged
Haning, R.V., Jr, Austin, C.W., Kuzma, D.L., Shapiro, S.S. and Zweibel, W.J.
40±48 years. J. Assist. Reprod. Genet., 13, 395±400.
(1982) Ultrasound evaluation of estrogen monitoring for induction of
Bancsi, L.F., Huijs, A.M., den Ouden, C.T., Broekmans, F.J., Looman, C.W.,
ovulation with menotropins. Fertil. Steril., 37, 627±632.
Blankenstein, M.A. and te Velde, E.R. (2000) Basal follicle-stimulating
Hsieh, Y.Y., Chang, C.C. and Tsai, H.D. (2001) Antral follicle counting in
hormone levels are of limited value in predicting ongoing pregnancy rates
predicting the retrieved oocyte number after ovarian hyperstimulation.
after in vitro fertilization. Fertil. Steril., 73, 552±557.
J. Assist. Reprod. Genet., 18, 320±324.
Bancsi, L.F., Broekmans, F.J., Eijkemans, M.J., de Jong, F.H., Habbema, J.D.
Huang, F.J., Chang, S.Y., Tsai, M.Y., Kung, F.T., Wu, J.F. and Chang, H.W.
and te Velde, E.R. (2002) Predictors of poor ovarian response in in vitro
(2001) Determination of the ef®ciency of controlled ovarian
fertilization: a prospective study comparing basal markers of ovarian
hyperstimulation in the gonadotropin-releasing hormone agonist-
reserve. Fertil. Steril., 77, 328±336.
suppression cycle using the initial follicle count during gonadotropin
Broekmans, F.J., Bernardus, R.E., Broeders, A., Berkhout, G. and
stimulation. J. Assist. Reprod. Genet., 18, 91±96.
Schoemaker, J. (1993) Pituitary responsiveness after administration of a
Klein, N.A., Battaglia, D.E., Fujimoto, V.Y., Davis, G.S., Bremner, W.J. and
GnRH agonist depot formulation: Decapeptyl CR. Clin. Endocrinol. (Oxf.),
Soules, M.R. (1996a) Reproductive aging: accelerated ovarian follicular
development associated with a monotropic follicle-stimulating hormone rise
Chang, M.Y., Chiang, C.H., Hsieh, T.T., Soong, Y.K. and Hsu, K.H. (1998)
in normal older women. J. Clin. Endocrinol. Metab., 81, 1038±1045.
Use of the antral follicle count to predict the outcome of assisted
Klein, N.A., Battaglia, D.E., Clifton, D.K., Bremner, W.J. and Soules, M.R.
reproductive technologies. Fertil. Steril., 69, 505±510.
(1996b) The gonadotropin secretion pattern in normal women of advanced
Corson, S.L., Gutmann, J., Batzer, F.R., Wallace, H., Klein, N. and Soules,
reproductive age in relation to the monotropic FSH rise. J. Soc. Gynecol.
M.R. (1999) Inhibin-B as a test of ovarian reserve for infertile women. Hum.
Lass, A., Skull, J., McVeigh, E., Margara, R. and Winston, R.M. (1997)
Creus, M., Penarrubia, J., Fabregues, F., Vidal, E., Carmona, F., Casamitjana,
Measurement of ovarian volume by transvaginal sonography before
R., Vanrell, J.A. and Balasch, J. (2000) Day 3 serum inhibin B and FSH and
ovulation induction with human menopausal gonadotrophin for in-vitro
age as predictors of assisted reproduction treatment outcome. Hum. Reprod.,
fertilization can predict poor response. Hum. Reprod., 12, 294±297.
Lenton, E.A., Landgren, B.M., Sexton, L. and Harper, R. (1984) Normal
variation in the length of the follicular phase of the menstrual cycle: effect
Schipper, I., de Jong, F.H. and Fauser, B.C. (1998) Lack of correlation
of chronological age. Br. J. Obstet. Gynaecol., 91, 681±684.
between maximum early follicular phase serum follicle stimulating
Mikkelsen, A.L., Andersson, A.M., Skakkebaek, N.E. and Lindenberg, S.
hormone concentrations and menstrual cycle characteristics in women
(2001) Basal concentrations of oestradiol may predict the outcome of in-
under the age of 35 years. Hum. Reprod., 13, 1442±1448.
vitro maturation in regularly menstruating women. Hum. Reprod., 16,
Scott, R.T., Jr, Hofmann, G.E., Oehninger, S. and Muasher, S.J. (1990)
Intercycle variability of day 3 follicle-stimulating hormone levels and its
Mosher, W.D. and Pratt, W.F. (1991) Fecundity and infertility in the United
effect on stimulation quality in in vitro fertilization. Fertil. Steril., 54,
States: incidence and trends. Fertil. Steril., 56, 192±193.
Muasher, S.J., Oehninger, S., Simonetti, S., Matta, J., Ellis, L.M., Liu, H.C.,
Seifer, D.B., Gardiner, A.C., Ferreira, K.A. and Peluso, J.J. (1996) Apoptosis
Jones, G.S. and Rosenwaks, Z. (1988) The value of basal and/or stimulated
as a function of ovarian reserve in women undergoing in vitro fertilization.
serum gonadotropin levels in prediction of stimulation response and in vitro
fertilization outcome. Fertil. Steril., 50, 298±307.
Seifer, D.B., Lambert-Messerlian, G., Hogan, J.W., Gardiner, A.C., Blazar,
Ng, E.H., Tang, O.S. and Ho, P.C. (2000) The signi®cance of the number of
A.S. and Berk, C.A. (1997) Day 3 serum inhibin-B is predictive of assisted
antral follicles prior to stimulation in predicting ovarian responses in an IVF
reproductive technologies outcome. Fertil. Steril., 67, 110±114.
programme. Hum. Reprod., 15, 1937±1942.
te Velde, E.R. and Pearson, P.L. (2002) The variability of female reproduction
Noord-Zaadstra, B.M., Looman, C.W., Alsbach, H., Habbema, J.D., te Velde,
ageing. Hum. Reprod. Update, 8, 141±154.
E.R. and Karbaat, J. (1991) Delaying childbearing: effect of age on
fecundity and outcome of pregnancy. Br. Med. J., 302, 1361±1365.
Tomas, C., Nuojua-Huttunen, S. and Martikainen, H. (1997) Pretreatment
transvaginal ultrasound examination predicts ovarian responsiveness to
Pache, T.D., Wladimiroff, J.W., de Jong, F.H., Hop, W.C. and Fauser, B.C.
gonadotrophins in in-vitro fertilization. Hum. Reprod., 12, 220±223.
(1990) Growth patterns of nondominant ovarian follicles during the normal
menstrual cycle. Fertil. Steril., 54, 638±642.
van Santbrink, E.J., Hop, W.C., van Dessel, T.J., de Jong, F.H. and Fauser,
Pohl, M., Hohlagschwandtner, M., Obruca, A., Poschalko, G., Weigert, M. and
B.C. (1995) Decremental follicle-stimulating hormone and dominant
Feichtinger, W. (2000) Number and size of antral follicles as predictive
follicle development during the normal menstrual cycle. Fertil. Steril., 64,
factors in vitro fertilization and embryo transfer. J. Assist. Reprod. Genet.,
van Zonneveld, P., Scheffer, G.J., Broekmans, F.J., Blankenstein, M.A., de
Ranieri, D.M., Quinn, F., Makhlouf, A., Khadum, I., Ghutmi, W., McGarrigle,
Jong, F.H., Looman, C.W.N., Habbema, J.D.F. and te Velde, E.R. (2003)
H., Davies, M. and Serhal, P. (1998) Simultaneous evaluation of basal
Do cycle disturbances explain the age related decline of female fertility?
follicle-stimulating hormone and 17 beta-estradiol response to
Cycle characteristics of women aged over 40 years compared with a
gonadotropin-releasing hormone analogue stimulation: an improved
reference population of young women. Hum. Reprod., 18, 495±501.
predictor of ovarian reserve. Fertil. Steril., 70, 227±233.
Welt, C.K., Adams, J.M., Sluss, P.M. and Hall, J.E. (1999) Inhibin A and
Ravhon, A., Lavery, S., Michael, S., Donaldson, M., Margara, R., Trew, G.
inhibin B responses to gonadotropin withdrawal depends on stage of follicle
and Winston, R. (2000) Dynamic assays of inhibin B and oestradiol
development. J. Clin. Endocrinol. Metab., 84, 2163±2169.
following buserelin acetate administration as predictors of ovarian response
Winslow, K.L., Toner, J.P., Brzyski, R.G., Oehninger, S.C., Acosta, A.A. and
in IVF. Hum. Reprod., 15, 2297±2301.
Muasher, S.J. (1991) The gonadotropin-releasing hormone agonist
Scheffer, G.J., Broekmans, F.J., Dorland, M., Habbema, J.D., Looman, C.W.
stimulation testÐa sensitive predictor of performance in the ¯are-up
and te Velde, E.R. (1999) Antral follicle counts by transvaginal
in vitro fertilization cycle. Fertil. Steril., 56, 711±717.
ultrasonography are related to age in women with proven natural fertility.
Wood, J.W. (1989) Fecundity and natural fertility in humans. Oxf. Rev.
Scheffer, G.J., Broekmans, F.J., Bancsi, L.F., Habbema, D.J.F., Looman,
C.W.N. and te Velde, E.R. (2002) Quantitative transvaginal two- and three-
Submitted on April 27, 2001; resubmitted on September 26, 2002; accepted on
dimensional sonography of the ovaries: reproducibility of antral follicle
counts. Ultrasound Obstet. Gynecol., 20, 270±275.
ArtVitum ® Monografie 4 Navitum Sterne: Prävention/Behandlung von degenerativen Gelenkerkrankungen Produktbeschreibung: ArtVitum® ist eine einzigartige Kombination von Chondroitin und Glucoseamin mit klinisch belegter Wirksamkeit der Einzelkomponenten bei Osteoarthritis (Gelenkabnutzung). Navitum® Pharma hat ArtVitum® entsprechend den Ergebnissen richtungsweisender klinischer Stud
Additional Information Juan Bustillo, M.D. Professor of Psychiatry and Neurosciences Director, Schizophrenia Research Program Medical Director Spanish Speaking Clinic Attending Psychiatrist, Clozapine Clinic Research Mentor NIH, Scientific Review Group ITVA (Interventions Committee for Adult Disorders). Member: 6/2011 to 2/2014 Exemplary Psychiatrist Award, National Alliance on Mental Il
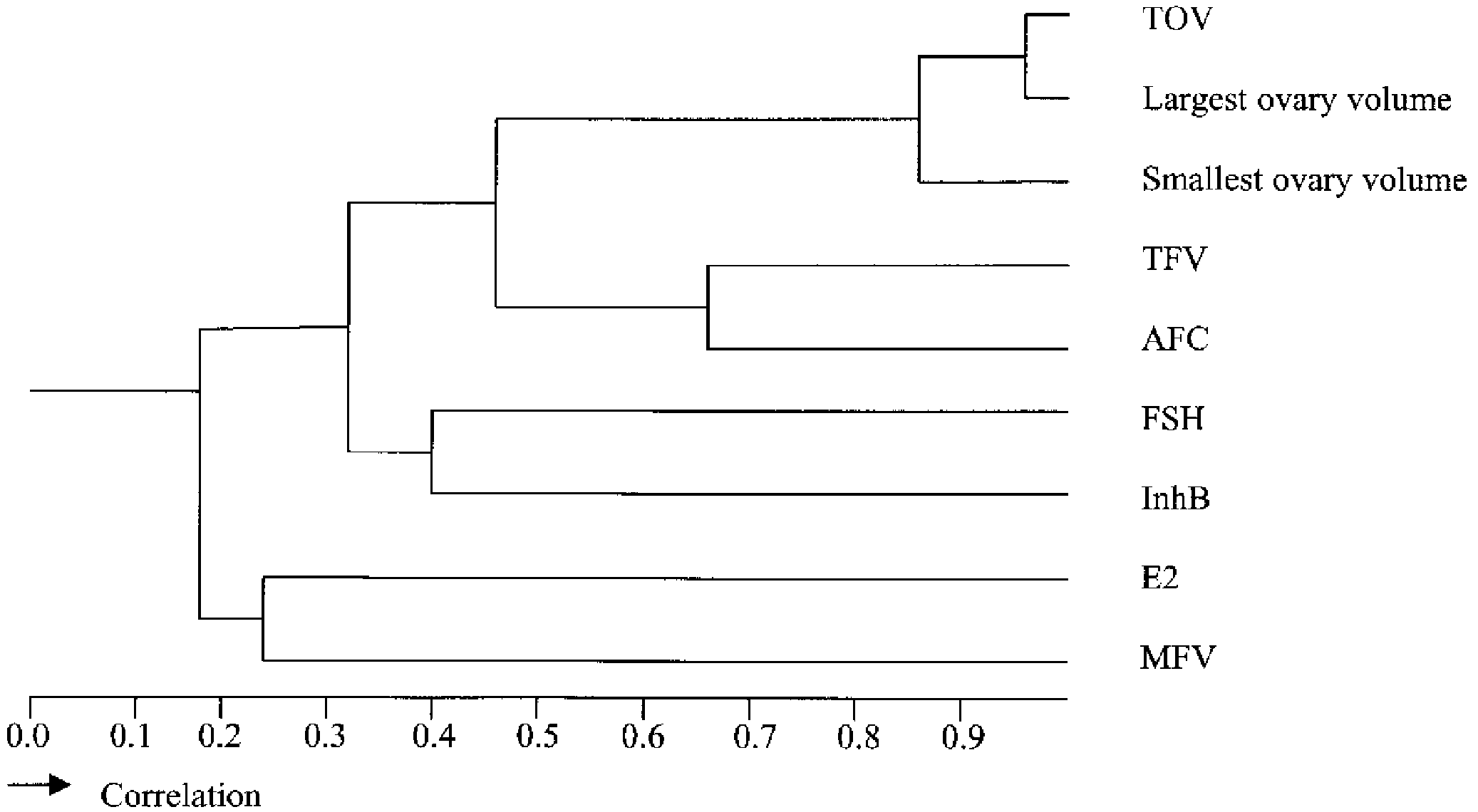 Table II. Correlation matrix of basal endocrine and ultrasound parameters. (Total group, n = 162)
Smallest ovary volume (small) ±0.24* ±0.10
Total follicular volume (TFV) ±0.36* ±0.17* 0.40* 0.69* 0.47* 0.42* 0.44*
0.25* 0.29* ±0.12 ±0.68* ±0.30* ±0.26* ±0.21* ±0.34* 0.37*
were determined in a stepwise fashion after controlling for the effect
of variables having the strongest correlation with chronological age in
previous steps. The square of the correlation of a variable with
chronological age was calculated as a re¯ection of the fraction of
variation of chronological age explained by this variable and was
considered a direct measure of its predictive performance. The
additional predictive effect of the subsequent variables, after the best
one had been selected, was calculated by multiplying the squares of
the partial correlations with the remaining unexplained fraction.
Table II. Correlation matrix of basal endocrine and ultrasound parameters. (Total group, n = 162)
Smallest ovary volume (small) ±0.24* ±0.10
Total follicular volume (TFV) ±0.36* ±0.17* 0.40* 0.69* 0.47* 0.42* 0.44*
0.25* 0.29* ±0.12 ±0.68* ±0.30* ±0.26* ±0.21* ±0.34* 0.37*
were determined in a stepwise fashion after controlling for the effect
of variables having the strongest correlation with chronological age in
previous steps. The square of the correlation of a variable with
chronological age was calculated as a re¯ection of the fraction of
variation of chronological age explained by this variable and was
considered a direct measure of its predictive performance. The
additional predictive effect of the subsequent variables, after the best
one had been selected, was calculated by multiplying the squares of
the partial correlations with the remaining unexplained fraction.