Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Neurophys.biomedicale.univ-paris5.fr
Synchrony of rest tremor in multiple limbs in Parkinson’s disease: evidence for multiple oscillators H. Ben-Pazi1,3, H. Bergman2,4, J. A. Goldberg2,4, N. Giladi1, D. Hansel4,5, A. Reches3, and E. S. Simon1
1 Department of Neurology, Tel-Aviv Sourasky Medical Center, Tel-Aviv,
3 Department of Neurology, Hebrew University Faculty of Medicine, Jerusalem, and
4 Interdisciplinary Center for Neural Computation, Hebrew University,
5 Laboratorie de Neurophysique et Physiologie du Systeme Moteur,
Summary. Recent evidence points to involvement of central nervous system oscillators in Parkinson’s disease (PD) rest tremor. It remains unknown whether one or multiple oscillators cause tremor in multiple limbs. Based on the prediction that multiple oscillators would cause low coherence even with similar average frequency, we studied 22 PD patients using accelerometers on multiple limbs. Records were digitized and spectral analysis was performed. Peak frequencies in the arms, legs, and chin were similar, indicating that biomechanical factors did not determine the frequency. Coherence between different axes of individual accelerometers and between different segments of the same limb was high. However, coherence between tremor in different limbs was low. There was no consistent pattern across patients of ipsi- vs. contralateral predominance of coherence. These data suggest that tremor in PD is generated by multiple oscillatory circuits, which operate on similar frequencies. Keywords: Tremor, Parkinson’s disease, oscillations, synchrony, basal ganglia, coherence. Introduction
Rest tremor in Parkinson’s disease (PD) is a common and often debilitatingsymptom that may be refractory to medical treatment. Recently, improvedunderstanding of the physiology of the basal ganglia (BG) (Albin et al., 1989;Chesselet and Delfs, 1996; Wichmann and DeLong, 1996) has led to thereemergence of stereotactic neurosurgical procedures as viable and effectivetreatment options for PD tremor. Lesions or deep brain stimulation to either
the ventral intermediate nucleus (VIM) of the thalamus (Benabid et al., 1991;Pollak et al., 1993), globus pallidus (Lozano et al., 1995), or subthalamicnucleus (Benabid et al., 1994; Kumar et al., 1998) can effectively alleviatetremor in contralateral limbs in PD. These developments highlight the needfor better understanding of PD tremor pathophysiology, as a basis for futuretherapeutic innovations.
Mounting evidence implicates involvement of several CNS regions in
generation and propagation of PD rest tremor. Intraoperative recordingshave demonstrated “tremor cells” in the thalamus (Lenz et al., 1988), globuspallidus (Hutchison et al., 1997), and subthalamic nucleus (Hutchison et al.,1998) of PD patients undergoing stereotactic procedures for tremor relief. Additionally, data from multi-cellular recording from globus pallidus inprimates made parkinsonian by administration of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) showed emergence of increased oscillations andsynchrony of neighboring cells (Bergman et al., 1998). In other studies ofPD tremor, voltage oscillations at the tremor frequency in the thalamus(Volkmann et al., 1996) and primary motor and premotor cortices (Tass et al.,1998) were found by magnetoencephalography. These observations begin toaddress why surgical lesions or electrical stimulation of thalamic (Benabidet al., 1991) or BG nuclei (Benabid et al., 1994; Lozano et al., 1995; Kumar etal., 1998) can effectively improve tremor in contralateral limbs in PD.
A central issue in investigation of tremorgenic mechanisms involves
identification and characterization of involved nuclei or networks. It remainscontroversial whether one or multiple interacting tremorgenic circuits arecritical. Studies of neuronal firing-tremor correlation (Hurtado et al., 1999;Levy et al., 1999) and of multi-limb tremor recording (Lauk et al., 1999;Raethjen et al., 2000) indicated that multiple oscillatory mechanisms areinvolved. However, Hunker and Abbs (1990), using multi-limb electromyo-graphic (EMG) recordings showed similar tremor frequency, from which theauthors inferred a single oscillatory generator. The present study involvesfrequency domain analysis of multi-limb accelerometric recordings to exam-ine the relationship of PD rest tremor between different body parts. Our nullhypothesis was that tremor in different body parts would be of high coherenceif generated by a single oscillator. These data were previously presented inabstract form (Ben Pazi et al., 1999).
Twenty two patients at two medical centers participated in the study. Inclusion criteriawas determined by a movement disorders specialist based on the diagnosis of PDaccording to the United Kingdom Brain Bank criteria (Hughes et al., 1992), and theexistence of bilateral limb tremor. Exclusion criteria were significant dementia, con-current neurological illness, pyramidal signs, or significant autonomic failure. All patientsunderwent routine neurological examinations including the United Parkinson’s DiseaseRating Scale (UPDRS). Patients were requested to stop levodopa the night prior totesting. The Helsinki Commission of the Health Ministry of the State of Israel approvedthe study, and all patients provided informed consent.
The tremor of 13 subjects was recorded by triaxial accelerometers (16 grams; Kistler,
USA) and that of nine subjects was recorded by miniature monoaxial accelerometers
(0.5 grams; Depew, USA). Accelerometers were placed variably on the index finger, handdorsum, upper arm, foot dorsum, first toe, or chin, according to the available accelero-meters and the clinical expression of tremor. Subjects were in a comfortable supineposition (lying flat or reclined sitting) with hands at rest and not touching each other. Three successive 2 minutes epochs were recorded. The accelerometer’s signal was ampli-fied, hardware filtered (Butterworth, 4 poles, 1–30 Hz), and digitized at a rate of 100 Hz(National Instruments, USA).
Digital data analysis was implemented in a custom program written in Matlab (The
Mathworks, USA). The power spectra in the bandwidth of 3–18 Hz were estimated usingWelch’s method, a fast Fourier transform algorithm, and the frequency of the maximalpower magnitude was determined (referred to here as “peak frequency”). The synchronybetween the signals was determined by estimating the coherence function, whichmeasures the linear correlation between them as a function of the frequency (Carter,1987). This function results in a frequency dependent curve ranging in magnitude from0–1, where 1 indicates that the frequency of two signals co-vary exactly in the givenfrequency band. In all cases, coherence measures were evaluated for the entire dataepoch to enhance resolution of the coherence function. The resolution of the power andcoherence spectra was 0.2 Hz, and the 95% confidence level for the coherence was 0.13,based on (Carter, 1987). Maximal coherence values in the range of 3–8 Hz (the range ofPD tremor) were considered for this study. When population summaries are given theyare as “average Ϯ standard deviation”.
In order to examine whether there was greater coherence between ipsi- or contra-
lateral limbs in each subject, we used the following formula: (Ipsi Ϫ Contra)/(Ipsi ϩContra), where Ipsi is the coherence of tremor signals from limbs on the same side of thebody, and Contra is the coherence of tremor signals from homologous limbs on oppositesides of the body. We sought correlation of this tremor “ipsi/contra predominance”parameter with clinical subclass as defined by Tremor/Postural Instibility and GaitDifficulty (T/PIGD) score, and with other clinical variables such as disease duration, sex,and age. The T/PIGD score is a measure derived from the UPDRS, as an indication of therelative severity of tremor or postural instability and gait difficulties (Jankovic et al.,1990).
Patient characteristics are shown in Table 1. Of note, there was a wide rangeof severity of PD manifestations, as evidenced by total UPDRS scores. Inaddition, T/PIGD scores were widely distributed. All patients were treatedwith levodopa/carbidopa, together with various combinations of selegeline,and dopamine agonist and anticholinergic drugs. Patients complied to variousdegrees with the request to withhold levodopa, but all patients had tremor atthe time of examination.
Data from one patient is shown in Fig. 1, which illustrates how tremor
signals of similar frequency may have either high or low coherence. Powerspectra computed from long time epochs showed clear peaks indicatingdominant frequency (“peak frequency”) at approximately 5 Hz. However,coherence was low between ipsilateral limbs (Fig. 1C) and high betweencontralateral limbs (Fig. 1F). The finding of low coherence between signalsthat have apparently similar frequencies may be understood in light of thefact that the power spectrum represents the average from the entire dataepoch. If the frequencies of two signals change in different ways over time,then the coherence may be low despite the fact that the average frequencymay be the same. Here, we see that in the same individual, relatively high
Table 1. Clinical characteristics of the patient population. Evident in the T/PIGD is the
bias of our selection for the presence of significant tremor
UPDRS Uniform Parkinson’s Disease Rating Scale; T/PIGD Tremor / postural
instability and gait disorder score (computed from the UPDRS)
coherence is present in the tremor bandwidth only between contralateralhands.
On average, PD rest tremor in different limbs had similar peak frequency.
This is demonstrated in Fig. 2A, where the bars represent the peak frequencyfor all measurements, averaged across all subjects. The surprisingly smallvariability in the peak frequency regardless of the mass of the limb indicatesthat all body parts receive similar rhythmic neuronal drive. However, itcannot be concluded based on average frequency data alone whether thetremor in different limbs was derived from the same oscillatory source. Sincethe peak frequency of each accelerometer signal was computed from theentire recording epoch, the similarity in peak frequency indicates only that theaverage frequency in the two signals was similar for that epoch. In fact, weobserved that there was considerable temporal variation of individual powerspectra (not shown). As such, it is possible that the two signals have differentinstantaneous frequencies that change over time, and therefore the temporalchanges in the signals are not related. In such a case, low coherence of the twosignals provides evidence for different tremorgenic sources driving the tremorin the different joints. Fig. 1. Example of frequency domain data. Data from monoaxial accelerometers placed on one patient, AM, is shown after transformation of sinusoidal tremor signals to the frequency domain (see Methods). Power spectra of signals from left hand (A) and left foot (B) indicate similar peak frequency of close to 5 Hz. However, coherence (C) is low in the bandwidth of the tremor frequency. In contrast, during a different epoch, power spectra of signals from the left hand (D) and right hand (E) and the coherence (F) had a significant peak in the bandwidth of the tremor frequency. Units as shown; power spectra
in multiples of the acceleration of gravity (g)
Several comparisons of coherence were computed to evaluate the extent
of coupling between tremor signals both within and between limbs. Thesedata, as summarized in Fig. 2B, are shown for five representative subjects. For each subject, average coherence values for comparisons between each ofthe axes of individual triaxial accelerometers (leftmost gray bars, “axis”),between accelerometer signals from placements on the same limb (upper arm,hand, and finger; center white bars, “segment”), and from different upper andlower limbs (rightmost black bars, “limb”) were analyzed. A clear patternemerged: while the interaxis and intersegment coherence was relatively high,the interlimb coherence was generally low. For the entire population ofsubjects, the interaxis coherence value was 0.72 Ϯ 0.19, the intersegmentcoherence was 0.56 Ϯ 0.28, and the interlimb coherence was 0.31 Ϯ 0.20.
For six patients who had obvious chin tremor, we computed average
coherence values between signals from an accelerometer placed on the chinand each of the three axes from multiple triaxial accelerometers placed on
Fig. 2. Summary data: tremor frequency and coherence. A Tremor frequency in different body parts. The average and standard deviation of the peak frequency for rest tremor in different body parts is shown. Note the similarity in average frequency, despite the large difference in mass and biomechanical properties. B Intralimb and interlimb coherence. Shown is the comparison of coherence between tremor in different axes of the same accelerometer (gray; axis), between different segments of the same limb (white; segment), and between different limbs (black; limb) for a subset of patients. C Coherence between chin and limbs. Shown is the comparison of average coherence between tremor in the chin and each of the accelerometers on the limbs (white; segment), and between different limbs (black; limb) for a subset of patients. Bars represent average coherence. Coherence
(ordinate) is in arbitrary units, with range [0, 1] (see Methods)
Fig. 3. Comparison of coherence between ipsi- and contralateral limbs. Shown are the average (white) and maximal (black) values of the derived “ipsi/contra predominance” parameter (ordinate) for each patient (see Methods). Evident is the large variability in
this parameter, both between patients and for multiple trials within each patient
the limbs. These data, summarized in Fig. 2C, demonstrate relatively lowcoherence, generally comparable in magnitude to interlimb coherence in thesame subjects. For the entire population, chin-limb coherence was 0.22 Ϯ 0.23.
The ipsi/contra predominance parameter (Ipsi Ϫ Contra)/(Ipsi ϩ Contra),
did not show any consistent pattern among the patient population (Fig. 3). Both the average and maximum values of this parameter are shown,indicating that there were approximately equal numbers of patients withgreater coherence when comparing ipsilateral or contralateral limbs. Further,there was no significant correlation between this parameter and T/PIGDscoring, disease duration or other clinical variables (two-tailed paired t-test,p Ͼ 0.2). Discussion
The present results show that, despite having similar tremor frequency, PDrest tremor in different limbs is generally of low coherence. One interpre-tation of these results is that tremor in different limbs is driven by differentoscillators which are coupled. Since the coherence is low, we must assume thatthe coupling is weak and their synchrony can be easily disrupted. It should benoted that in the present study coherence was computed for long time epochs,and therefore we cannot exclude that tremor in different limbs might be morestrongly synchronized for brief epochs. This issue will be a focus of futurestudy.
An alternative interpretation of our results is that a common oscillator
drives the tremor in different limbs, and that the observed low coherencemight result from noise in the neural control signals downstream to theoscillator. Although we found that tremor in different limbs can displaysignificant coherence, the magnitude was generally small. A further argumentagainst this interpretation is that the coherence between axes of the same
accelerometer and within limbs was systematically higher that between limbs. There should be no reason why desynchronizing noise would preferentiallyaffect motor circuits leading to different limbs, although we cannot excludethis factor. Rather, we favor the hypothesis that different oscillators that areweakly coupled drive tremor in different limbs.
Our findings are consistent with several recent reports suggesting multiple
oscillators in PD tremor (Hurtado et al., 1999; Lauk et al., 1999; Raethjenet al., 2000), physiological tremor (Lauk et al., 1999), and essential tremor(Simon and Giladi, 1999; Lauk et al., 1999). However, Hunker and Abbs(1990) suggested a single oscillator. In fact, our finding of similar averagefrequency in different limbs is consistent with that of Hunker and Abbs(1990). By calculating the coherence between tremor signals, a step not per-formed by Hunker and Abbs, we were able to infer multiple tremorgenicoscillatory circuits.
It is noteworthy that there was marked interpatient variability in the
coherence measurements. Nonetheless, within each patient there was aconsistent finding of low interlimb coherence relative to the interaxis andintersegment coherence. The relatively high interaxis and intersegmentcoherence may be accounted for either by higher mechanical coupling ortighter coupling of CNS oscillators. The likelihood of a significant degree ofmechanical coupling and the high sensitivity of coherence values to suchcoupling (Tass et al., 1998) strengthens our conclusions, as it may be inferredthat the coherence measure would be even lower in the absence of mechanicalcoupling.
As a step towards understanding the somatotopic organization of tremor-
genic oscillators in PD, we sought a measure of the degree of unilaterality ofthe tremor coherence. Since most motor circuits are mainly related to oneside of the body and PD signs are often asymmetric, it may be expectedthat coherence of tremor would be greater between ipsilateral limbs thanin contralateral limbs. However, we found no pattern of the “ipsi/contrapredominance” parameter across our patient population. Regarding clinical-electrophysiological correlation, we postulated that the degree of unilateralitymight correlate with the subclass of PD – either those patients exhibiting atremor-predominant syndrome or patients with a greater tendency towardsbilateral symptoms of postural instability and gait disability. We predicatedthat the tremor-predominant patients would have greater unilaterality, asreflected by the “ipsi/contra predominance” parameter. However, we foundno significant correlation between these two measures. We are aware thatthe small numbers of patients in this study precludes definitive statementsregarding patient subclass characteristics.
In conclusion, the present results demonstrate low interlimb coherence
in PD rest tremor, and thereby provide evidence for multiple oscillators intremorgenesis. This provides orientation for experimental design and datainterpretation for studies aimed at identifying and characterizing CNSnetworks involved in tremor generation, employing extracellular record-ing and neuroimaging techniques. We believe in the importance offurther characterization of the dynamics of putative neural oscillators that
may be involved in voluntary and involuntary movements. Studies such asthis may lead to future innovations in physiologically based treatments forPD. Acknowledgments
The authors are grateful for the support and guidance of Prof. A. Korczyn. This work wassupported in part by Israeli Academy of Science, AFIRST, and the US-Israel Bi-nationalScience Foundation (HB). References
Albin RL, Young AB, Penney JB (1989) The functional anatomy of basal ganglia
Ben Pazi H, Giladi N, Korczyn AD, Reches A, Hansel D, Goldberg J, Bergman H, Simon
ES (1999) Low interlimb coherence in Parkinson’s disease rest tremor [abstract]. SocNeurosci Abstr 25: 375
Benabid A, Pollak P, Gervason C, Hoffmann D, Gao D, Hommel M, Perret J, De
Rougemont J (1991) Long-term suppression of tremor by chronic stimulation of theventral intermediate thalamic nucleus. Lancet 337: 403–406
Benabid AL, Pollak P, Gross C, Hoffmann D, Benazzouz A, Gao DM, Laurent A, Gentil
M, Perret J (1994) Acute and long-term effects of subthalamic nucleus stimulation inParkinson’s disease. Stereotact Funct Neurosurg 62: 76–84
Bergman H, Feingold A, Nini A, Raz A, Slovin H, Abeles M, Vaadia E (1998)
Physiological aspects of information processing in the basal ganglia of normal andparkinsonian primates. Trends Neurosci 21: 32–38
Carter GC (1987) Coherence and time delay estimation. Proc IEEE 75: 236–255Chesselet MF, Delfs JM (1996) Basal ganglia and movement disorders: an update. Trends
Hughes A, Daniel S, Kilford L, Lees A (1992) Accuracy of clinical diagnosis of idiopathic
Parkinson’s disease: a clinico-pathological study of 100 cases. J Neurol NeurosurgPsychiatry 55: 181–184
Hunker C, Abbs J (1990) Uniform frequency of parkinsonian resting tremor in the lips,
jaw, tongue, and index finger. Mov Disord 5: 71–77
Hurtado JM, Gray CM, Tamas LB, Sigvardt KA (1999) Dynamics of tremor-related
oscillations in the human globus pallidus: a single case study. Proc Natl Acad Sci USA96: 1674–1679
Hutchison WD, Lozano AM, Tasker RR, Lang AE, Dostrovsky JO (1997) Identification
and characterization of neurons with tremor-frequency activity in human globuspallidus. Exp Brain Res 113: 557–563
Hutchison WD, Allan RJ, Opitz H, Levy R, Dostrovsky JO, Lang AE, Lozano AM
(1998) Neurophysiological identification of the subthalamic nucleus in surgery forParkinson’s disease. Ann Neurol 44: 622–628
Jankovic J, McDermott M, Carter J, Gauthier S, Goetz C, Golbe L, Huber S, Koller W,
Olanow C, Shoulson I, et al. (1990) Variable expression of Parkinson’s disease: abase-line analysis of the DATATOP cohort. The Parkinson Study Group. Neurology40: 1529–1534
Kumar R, Lozano AM, Kim YJ, Hutchison WD, Sime E, Halket E, Lang AE (1998)
Double-blind evaluation of subthalamic nucleus deep brain stimulation in advancedParkinson’s disease. Neurology 51: 850–855
Lauk M, Koster B, Timmer J, Gusclauber B, Deuschl G, Lucking CH (1999) Side-to-side
correlation of muscle activity in physiological and pathological human tremors. ClinNeurophysiol 110: 1774–1783
Lenz FA, Tasker RR, Kwan H, Schneider S, Kwong R, Murayama Y, Dostrovsky JO,
Murphy J (1988) Single unit analysis of the human ventral thalamic nuclear group:
H. Ben-Pazi et al.: Synchrony of tremor in PD
correlation of thalamic “tremor cells” with the 3–6 Hz component of parkinsoniantremor. J Neurosci 8: 754–764
Levy R, Davis KD, Hutchison WD, Pahapill PA, Lozano AM, Tasker RR, Dostrovsky JO
(1999) Simultaneously recorded neuron pairs in the motor thalamus of patients withParkinson’s disease and essential tremor [Abstract]. Soc Neurosci Abstr 25: 1408–1408
Lozano AM, Lang AE, Galvez Jimenez N, Miyasaki J, Duff J, Hutchinson WD,
Dostrovsky JO (1995) Effect of GPi pallidotomy on motor function in Parkinson’sdisease. Lancet 346: 1383–1387
Pollak P, Benabid AL, Gervason CL, Hoffmann D, Seigneuret E, Perret J (1993) Long-
term effects of chronic stimulation of the ventral intermediate thalamic nucleus indifferent types of tremor. Adv Neurol 60: 408–413
Raethjen J, Lindemann M, Schmaljohann H, Wenzelburger R, Pfister G, Deuschl G
(2000) Multiple oscillators are causing parkinsonian and essential tremor. MovDisord 15: 84–94
Simon ES, Giladi N (1999) Essential tremor is essentially different from physiological
tremor: a study of position-specific intra-limb frequency and phase relationships[Abstract]. Neurology 52: A518
Tass P, Volkmann J, Weule J, Schnitzler A, Witte OW, Freund H-J (1998)
Corticomuscular and corticostriatal synchronization in parkinsonian rest tremor asrevealed by magnetoencephalography [Abstract]. Mov Disord 13 [Suppl 12]: 268–268
Volkmann J, Joliot M, Mogilner A, Ioannides A, Lado F, Fazzini E, Ribary U, Llinas R
(1996) Central motor loop oscillations in parkinsonian resting tremor revealed bymagnetoencephelography. Neurology 46: 1359–1370
Wichmann T, Delong MR (1996) Functional and pathophysiological models of the basal
ganglia. Curr Opin Neurobiol 6: 751–758
Authors’ address: E. S. Simon, M.D., Laboratory of Motor Physiology, Department
of Neurology, Tel-Aviv Sourasky Medical Center, 6 Weizmann Street, Tel-Aviv, 64239Israel, e-mail: [email protected]
Acceptability and Feasibility of Mifepristone-Misoprostol For Menstrual Regulation in Bangladesh CONTEXT: Annually, more than 700,000 women turn to menstrual regulation, or uterine evacuation with vacuum aspiration; many more resort to unsafe abortion. Using pills for the evacuation of the uterus could increase women’s access to safe menstrual regulation services and reduce the hig
Articles Neoadjuvant bevacizumab, trastuzumab, and chemotherapy for primary infl ammatory HER2-positive breast cancer (BEVERLY-2): an open-label, single-arm phase 2 study Jean-Yves Pierga, Thierry Petit, Thierry Delozier, Jean-Marc Ferrero, Mario Campone, Joseph Gligorov, Florence Lerebours, Henri Roché, Thomas Bachelot, Emmanuelle Charafe-Jauff ret, Maria Pavlyuk, Sandrine Kraemer, Fr
 Synchrony of rest tremor in multiple limbs in Parkinson’s disease:
Synchrony of rest tremor in multiple limbs in Parkinson’s disease: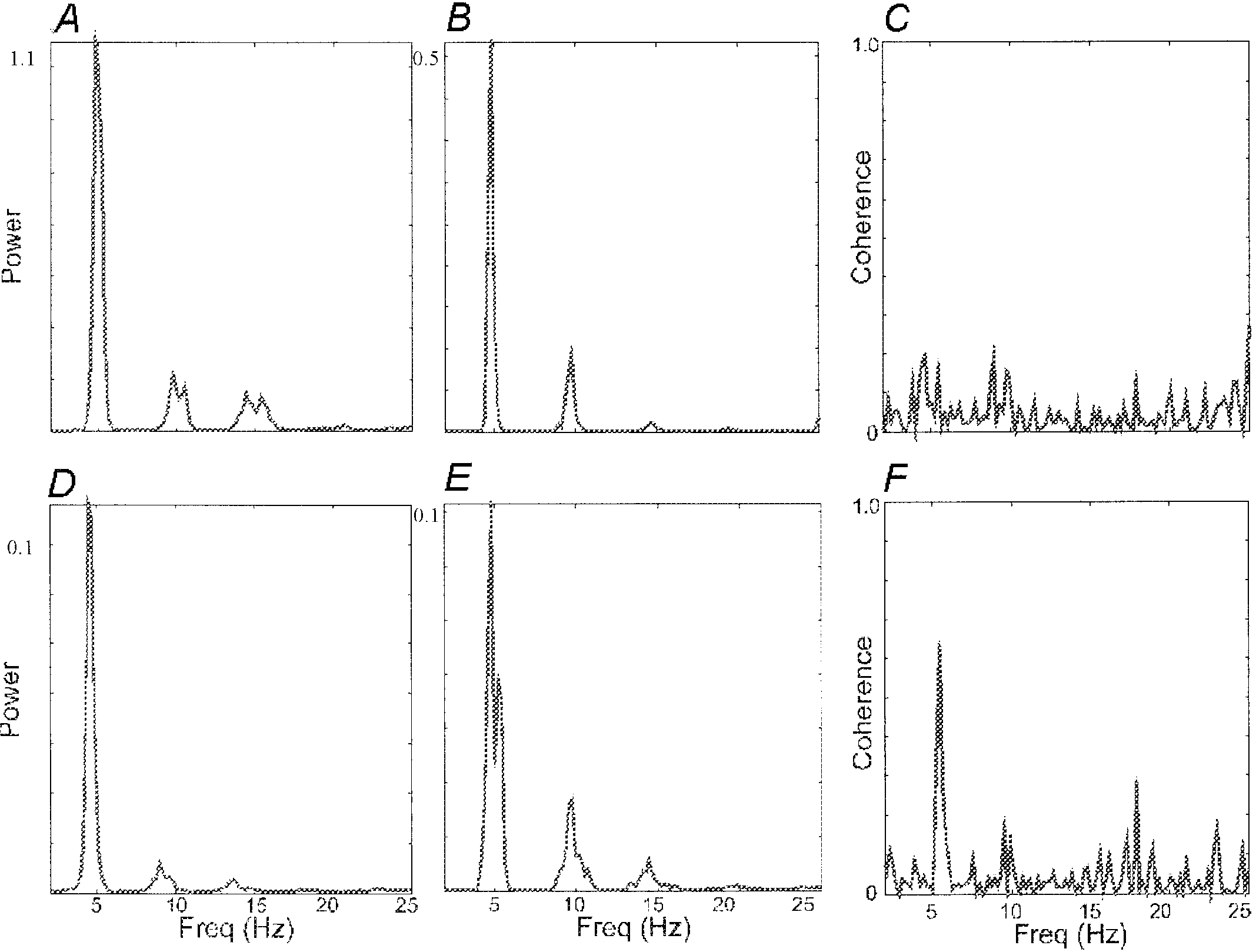 Fig. 1. Example of frequency domain data. Data from monoaxial accelerometers placed
Fig. 1. Example of frequency domain data. Data from monoaxial accelerometers placed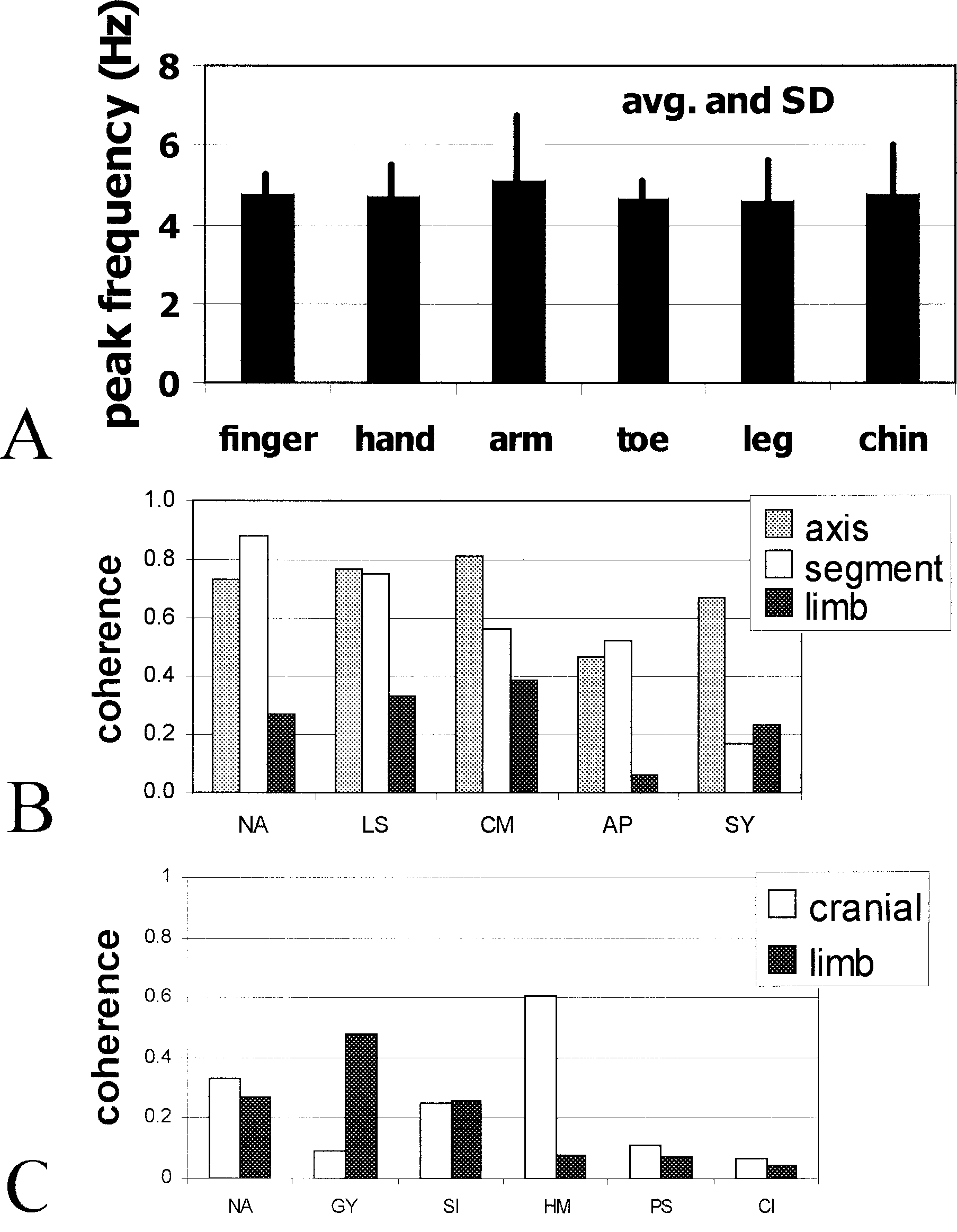 Fig. 2. Summary data: tremor frequency and coherence. A Tremor frequency in different
Fig. 2. Summary data: tremor frequency and coherence. A Tremor frequency in different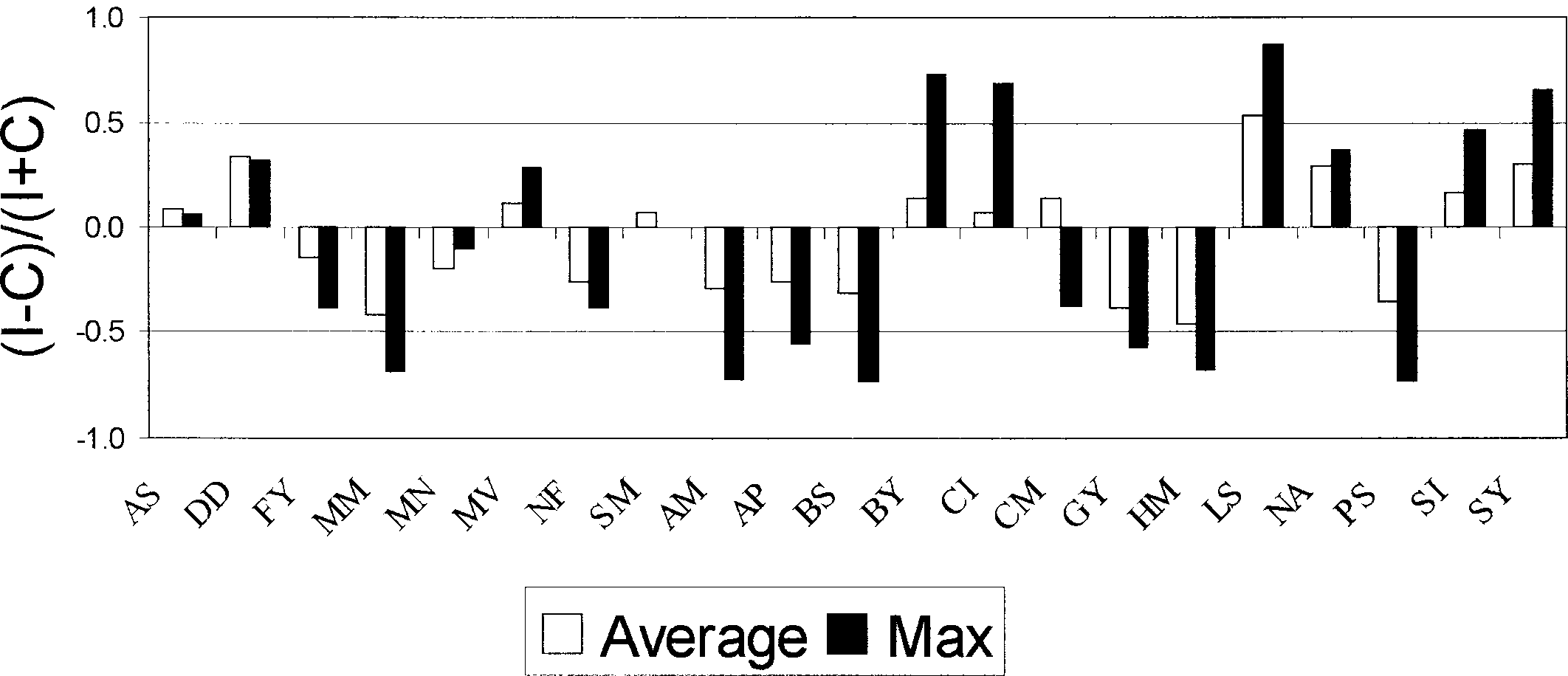 Fig. 3. Comparison of coherence between ipsi- and contralateral limbs. Shown are the
Fig. 3. Comparison of coherence between ipsi- and contralateral limbs. Shown are the