Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
043513u537
Azithromycin Reverses Airflow Obstruction in Established Bronchiolitis Obliterans Syndrome Bryan Yates, Desmond M. Murphy, Ian A. Forrest, Chris Ward, Robert M. Rutherford, Andrew J. Fisher, James L. Lordan, John H. Dark, and Paul A. Corris
William Leech Centre for Lung Research, The Freeman Hospital, High Heaton, Newcastle upon Tyne, United Kingdom
Introduction: A recent pilot study noted clinical benefit of macrolide
airflow limitation, progressive dyspnea, and ultimately, prema-
therapy in the management of six lung transplant recipients with
ture death (1, 10, 11). International Registry data shows a 50%
bronchiolitis obliterans syndrome (BOS), a condition previously
prevalence of BOS at 5 years after transplant. This is associated
regarded as irreversible. Objective: To examine the effect of low-
with a reduction in quality of life and increased morbidity and
dose macrolides on lung function in lung allograft recipients with
mortality, limiting 7-year mean survival to only 31% (12). established BOS and to assess whether this benefit is sustained.
The current classification of BOS is based on changes in
Methods: We retrospectively evaluated the effect of azithromycin (250 mg alternate days) on clinical status and lung function in 20
FEV1, with the maximum post-transplant FEV1 being assigned
allograft recipients with established BOS, confirmed by decline in
a 100% predicted value (the mean of the two best postoperative
1 or FEF25–75; consistent high-resolution computed tomography
1 values with at least 3 weeks between the measurements). findings; and exclusion of acute rejection, infection, or anastomatic
Patients experiencing a persistent decline in FEV1 (i.e., two con-
complications. Azithromycin was introduced at mean 82 months
secutive measurements within 3–6 weeks) in the absence of acute
after transplantation. BOS staging at initiation of treatment was
rejection, infection, or bronchial anastomosis complications are
BOS 3 (10), BOS 2 (2), BOS 1 (6), and BOS0-p (2). All patients were
grouped into stages. Additionally, a reduction in FEF25–75 is used
on maintenance immunosuppression comprising cell-cycle inhibi- tor, oral corticosteroids, and calcineurin inhibitor. Results: There
Current strategies in the management of BOS have ranged
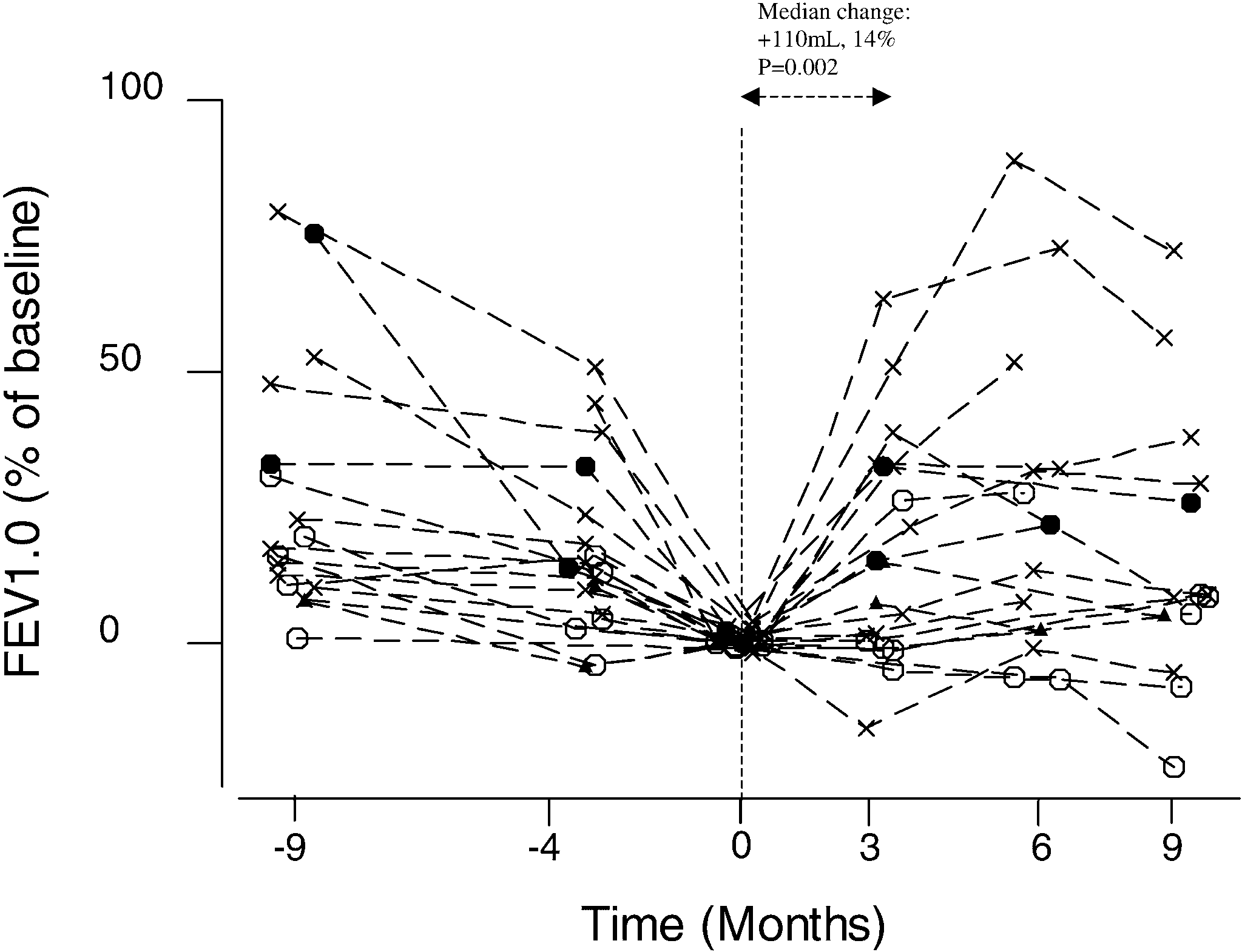
was a significant increase in FEV1 of median 110 ml (range, Ϫ70 to
from switching immunosuppressive regimens, augmenting with
730 ml) between baseline and 3 months of azithromycin therapy (p ϭ 0.002). This improvement was sustained beyond 3 months in
corticosteroids, and initiating cytolytic therapy. These have had
the majority of patients, who had initially benefited from azithro-
little or no impact on the progression of the condition. Although
mycin (up to 11 months follow up). Conclusions: This case series
we have recently demonstrated that total lymphoid irradiation
confirms the benefit of azithromycin in not only halting, but re-
(TLI) significantly reduces the rate of decline in graft function
versing the declining lung function seen in patients with BOS. This
associated with BOS, it fails to halt its progression and may
benefit appears to be maintained over time. Low-dose macrolides
have significant morbidity (14). Significantly, data from ex vivooffer a new and exciting therapeutic strategy for the treatment of
experiments indicate that many of the traditional agents used
progressive BOS, and further clinical and translational mechanistic
may upregulate proinflammatory cytokines and growth factors,
studies are required.
with a potentially detrimental effect on allografts (15–19). Keywords: lung; macrolide; transplantation
There has been recent interest in the potential role of macro-
lide antibiotics in the management of BOS. Macrolides have
Lung transplantation has evolved to become an accepted strat-
demonstrated antiinflammatory properties in other respiratory
egy in the management of advanced disease in selected patients
conditions such as asthma, cystic fibrosis, and diffuse panbronchi-
(1). Unfortunately, although there has been considerable improve-
olitis (15–26). Notably, in a recent pilot study, Gerhardt and co-
ment in early outcomes after lung transplantation as a result
workers described a significant, short-term improvement (mean
of advances in surgical techniques and better perioperative man-
follow-up of 14 weeks) in lung function in six lung transplant
agement, long-term survival remains limited by the development
recipients with BOS who were treated with azithromycin (27).
of bronchiolitis obliterans syndrome (BOS).
These promising data have been confirmed by Verleden and
The histologic lesion of BOS is obliterative bronchiolitis
colleagues in eight further subjects with short-term follow-up
(OB). This is characterized by epithelial cell activation as a
(28). In this article we examine the effect of low-dose mainte-
result of alloimmune and nonalloimmune mechanisms. An early
nance azithromycin therapy in 20 patients with BOS, followed
feature is peribronchiolar leukocyte infiltration leading to an
for up to 48 weeks. This study has previously been partially pre-
abnormal, exaggerated repair response, fibroproliferation, andeventual obliteration of the small airways (2–9). This leads to
sented at The International Society for Heart and Lung Trans-
deteriorating graft function that is characterized by the develop-
plantation and The American Thoracic Society annual meetings,
ment of progressive, irreversible small airway narrowing, fixed
with publication in abstract form (29, 30). Study Subjects
(Received in original form November 18, 2004; accepted in final form June 15, 2005)
Twenty lung transplant recipients with a diagnosis of BOS (n ϭ 18) or
This research was funded by the Newcastle upon Tyne Hospitals Special Trustees,
BOS0-p (n ϭ 2) were placed on maintenance azithromycin. A diagnosis
European Respiratory Society Fellowships (D.M.M., C.W.), Medical ResearchCouncil Fellowship (I.A.F.), and the McPhail Trust (J.L.L.).
of BOS was assigned on the basis of the International Society for Heartand Lung Transplantation criteria (13). Patients displayed no clinical
Correspondence and requests for reprints should be addressed to Paul A. Corris,
evidence of infection, acute rejection, or other cause for their deteriora-
The William Leech Centre for Lung Research, The Freeman Hospital, High Heaton,Newcastle upon Tyne, NE7 7DN, UK. E-mail: [email protected]
tion in lung function. All patients meeting these criteria for BOS wereconsecutively treated with azithromycin. The data presented in this
Am J Respir Crit Care Med Vol 172. pp 772–775, 2005 Originally Published in Press as DOI: 10.1164/rccm.200411-1537OC on June 23, 2005
paper were retrospectively collected and are presented in a case series
Internet address: www.atsjournals.org
Yates, Murphy, Forrest, et al.: Macrolide Therapy in BOS
Treatment Regimen
transplants, and three heart-lung transplants. The mean age at
All patients were treated with oral azithromycin at a dose of 250 mg
transplantation was 38 (range, 17–59 years), with an average
alternate days from the time of BOS diagnosis to preparation of this
manuscript. Patients were regularly evaluated at clinic with pulmonary
number of acute rejection episodes (Grade A2 or greater) was
function testing to assess response. Liver function was monitored at
regular intervals without any adverse effect of therapy. All patients
BOS stages at initiation of treatment were BOS 3 (n ϭ 10),
remained on immunosuppressive therapy comprising a calcineurin in-
BOS 2 (n ϭ 2), BOS 1 (n ϭ 6), and BOS0-p (n ϭ 2). Mean
hibitor (cyclosporin or tacrolimus), oral corticosteroids, and a purine
follow-up at time of manuscript preparation has been 6.25 months
antagonist (azathioprine or mycophenolate mofetil). The standard im-
(range, 3–11 months). There was a significant but variable im-
munosuppression regimen used at our facility is a triple therapy ap-
proach of cyclosporin, prednisolone, and azathioprine. In this study
two patients were on tacrolimus and one on mycophenolate. Azithro-
between baseline and after 3 months of azithromycin therapy
mycin was commenced at varying time points. Immunosuppressant lev-
(Figure 1, p ϭ 0.002). This improvement was sustained beyond
els were not affected by azithromycin therapy in our patient cohort.
3 months in 12 of 17 patients (up to 11 months follow-up). Figure
During the treatment phase, one patient required antibiotic treatment
1 shows percentage change in FEV1 from baseline.
for infection (Patient 15, Table 1) and one patient was switched tomycophenolate (Patient 17, Table 1). Mean follow-up is 6.25 months
DISCUSSION
We have confirmed the recent studies of Gerhardt and coworkers
Statistical Analysis
(27) and Verleden and colleagues (28), and have shown that
Patients had variable times of follow-up, and spirometry was performed
azithromycin therapy can successfully treat BOS, a condition
at various time points. Analysis was performed using nonparametric
refractory to previous clinical management. We have extended
methods (Minitab, release 14 for Windows; State College, PA) and
the current literature by performing our study in a bigger patient
post-treatment data grouped into 3-month blocks and compared with
baseline values. Baseline refers to spirometry measurements performed
These findings are remarkable in that they offer hope in
at the initiation of treatment. Spirometry measurements were per-
arresting the progression of BOS. There was median gain in lung
formed at 3 (2–4 months), 6 (5–7 months), and 9 (8–10) months.
function of 110 ml for the group, and in one patient a 730-mlincrease was observed. There were no side effects of therapy
reported by our patients, and no patient has discontinued therapy
Patient characteristics and responses are shown in Table 1 and
to date. This benefit profile is unprecedented in our program.
Figure 1. Our study population consisted of 10 males and 10
The mechanism of action of macrolides in BOS is not known,
females. The underlying diagnoses were cystic fibrosis (n ϭ 6),
but is not likely to be due to a direct microbicidal action, because
of the low doses used. Similar dosing regimens demonstrate
chiectesis (n ϭ 2), sarcoidosis (n ϭ 2), pulmonary hypertension
clinical improvement, efficacy, improved lung function, and anti-
(n ϭ 2), and retransplantation for obliterative bronchiolitis (n ϭ
inflammatory properties in patients with asthma, cystic fibrosis,
2). There were nine bilateral lung transplants, eight single lung
and panbronchiolitis (20–26). Several mechanisms have been
TABLE 1. CHARACTERISTICS OF STUDY PATIENTS Definition of abbreviations: BLT ϭ bilateral lung transplant; HLT ϭ heart-lung transplant; LSLT ϭ left single lung transplant;
RSLT ϭ right single lung transplant.
Age at transplant refers to the patient’s age in years, diagnosis refers to the patients diagnosis/indication for transplantation,
maximum FEV1 refers to the maximum measured post-transplant FEV1, acute rejection episodes refers to the number of acuterejection episodes of grade A2 or greater before the diagnosis of bronchiolitis obliterans syndrome (BOS), baseline FEV1 refers tothe FEV1 at the commencement of azithromycin, and BOS score refers to the BOS score assigned according to the InternationalSociety of Heart and Lung Transplantation guidelines (37).
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
References
1. Arcasoy SM, Kotloff RM. Lung transplantation. N Engl J Med 1999;
2. Sharples LD, McNeil K, Stewart S, Wallwork J. Risk factors for bronchio-
litis obliterans: a systematic review of recent publications. J HeartLung Transplant 2002;21:271–281.
3. Ross DJ, Marchevsky A, Kramer M, Kass RM. “Refractoriness” of air-
flow obstruction associated with isolated lymphocytic bronchiolitis/bronchitis in pulmonary allografts. J Heart Lung Transplant 1997;16:832–838.
4. Ward C, Snell GI, Zheng L, Orsida B, Whitford H, Williams TJ, Walters
EH. Endobronchial biopsy and bronchoalveolar lavage in stable lungtransplant recipients and chronic rejection. Am J Respir Crit Care Med1998;158:84–91.
5. Ward C, Snell GI, Orsida B, Zheng L, Williams TJ, Walters EH. Airway
versus transbronchial biopsy and BAL in lung transplant recipients:different but complementary. Eur Respir J 1997;10:2876–2880.
6. Ward C, Whitford H, Snell G, Bao H, Zheng L, Reid D, Williams TJ,
Walters EH. Bronchoalveolar lavage macrophage and lymphocytephenotypes in lung transplant recipients. J Heart Lung Transplant 2001;20:1064–1074.
7. Ward C, De Soyza A, Fisher AJ, Pritchard G, Forrest IA, Corris PA. Figure 1. Change in FEV1 over time. Each symbol represents an individ-
Reticular basement membrane thickening in airways of lung transplant
ual patient, and the broken line indicates the pattern of change in their
recipients is not affected by inhaled corticosteroids. Clin Exp Allergy
1 over time in months. The change in FEV1 is represented as a
8. DiGiovine B, Lynch JP III, Martinez FJ, Flint A, Whyte RI, Iannettoni
1 at the time azithromycin was commenced.
For comparison lung function before treatment is also included. Data
MD, Arenberg DA, Burdick MD, Glass MC, Wilke CA, Morris SB,Kunkel SI, Strieter RM. Bronchoalveolar lavage neutrophilia is associ-
at Ϫ9 months was measured 9 months before azithromycin therapy.
ated with obliterative bronchiolitis after lung transplantation: role of
Data at Ϫ4 months refers to values measured at Ϫ3 to Ϫ5 months. Open
IL-8. J Immunol 1996;157:4194–4202. circles ϭ BOS 1; filled circles ϭ BOS 2; cross ϭ BOS 3; filled triangles ϭ
9. Boehler A, Estenne M. Obliterative bronchiolitis after lung transplanta-
tion. Curr Opin Pulm Med 2000;6:133–139.
10. Corris PA. Bronchiolitis obliterans syndrome. Chest Surg Clin N Am
11. Ouwens JP, van der Mark TW, Koeter GH, de Boer WJ, Grevink RG,
proposed to explain these effects, including suppression of in-
van der Bij W. Bronchiolar airflow impairment after lung transplanta-
flammatory mediators and neutrophilic infiltration (31, 32), inhi-
tion: an early and common manifestation. J Heart Lung Transplant2002;21:1056–1061.
bition of airway remodeling through suppression of matrix met-
12. Hertz MI, Mohacsi PJ, Boucek MM, Taylor DO, Trulock EP, Deng MC,
alloproteinases (33), and modulation of the effects of low-grade
Rowe AW. The Registry of the International Society for Heart and
Pseudomonas infection (34, 35).
Lung Transplantation: past, present and future. J Heart Lung Trans-
Long-term low-dose azithromycin therapy offers a novel,
safe, and exciting therapy for the treatment of progressive BOS,
13. Estenne M, Maurer JR, Boehler A, Egan JJ, Frost A, Hertz M, Mallory
and our data confirm the beneficial effects in not only preventing
GB, Snell GI, Yousem S. Bronchiolitis obliterans syndrome 2001: an
a further decline in lung function, but leading to a variable level
update of the diagnostic criteria. J Heart Lung Transplant 2002;21:297–310.
of improvement in lung function in a majority of patients with
14. Fisher AJRR, Bozzino J, Parry G, Dark JH, Corris PA. The safety and
established BOS. The fact that airflow limitation regarded as
efficacy of total lymphoid irradiation in progressive bronchioli-
“fixed” has been reversed implies that structural changes have
tis obliterans syndrome after lung transplantation. Am J Transplant
occurred. In preliminary findings from the heterotopic tracheal
allograft animal model of lung transplantation, macrolide pre-
15. Borger P, Kauffman HF, Timmerman JA, Scholma J, van den Berg
medication has been shown to inhibit pathologic airway fibrosis
JW, Koeter GH. Cyclosporine, FK506, mycophenolate mofetil, andprednisolone differentially modulate cytokine gene expression in hu-
man airway-derived epithelial cells. Transplantation 2000;69:1408–
Our study is limited by the small patient cohort and is a
descriptive case series rather than a randomized, placebo-
16. Briffa N, Morris RE. New immunosuppressive regimens in lung trans-
controlled study. Hence, our findings, although extremely prom-
plantation. Eur Respir J 1997;10:2630–2637.
ising, need to be interpreted with caution. The magnitude of the
17. Hojo M, Morimoto T, Maluccio M, Asano T, Morimoto K, Lagman M,
treatment effect we observed suggests that a formal randomized
Shimbo T, Suthanthiran M. Cyclosporine induces cancer progression
placebo-controlled trial may be feasible. Further clinical and
by a cell-autonomous mechanism. Nature 1999;397:530–534.
18. Muraoka K, Fujimoto K, Sun X, Yoshioka K, Shimizu K, Yagi M, Bose
translational mechanistic studies of the effects of macrolide ther-
H Jr, Miyazaki I, Yamamoto K. Immunosuppressant FK506 induces
interleukin-6 production through the activation of transcription factornuclear factor (NF)-kappa(B): implications for FK506 nephropathy. Conflict of Interest Statement : B.Y. does not have a financial relationship with a J Clin Invest 1996;97:2433–2439.
commercial entity that has an interest in the subject of this manuscript; D.M.M. does not have a financial relationship with a commercial entity that has an interest
19. Zhang JG, Walmsley MW, Moy JV, Cunningham AC, Talbot D, Dark
in the subject of this manuscript; I.A.F. does not have a financial relationship with
JH, Kirby JA. Differential effects of cyclosporin A and tacrolimus
a commercial entity that has an interest in the subject of this manuscript; C.W.
on the production of TGF-beta: implications for the development of
does not have a financial relationship with a commercial entity that has an interest
obliterative bronchiolitis after lung transplantation. Transpl Int 1998;11:
in the subject of this manuscript; R.M.R. does not have a financial relationship
with a commercial entity that has an interest in the subject of this manuscript;
20. Equi A, Balfour-Lynn IM, Bush A, Rosenthal M. Long term azithromycin
A.J.F. does not have a financial relationship with a commercial entity that has an
in children with cystic fibrosis: a randomised, placebo-controlled cross-
interest in the subject of this manuscript; J.L.L. does not have a financial relation-ship with a commercial entity that has an interest in the subject of this manuscript;
over trial. Lancet 2002;360:978–984.
J.H.D. does not have a financial relationship with a commercial entity that has an
21. Everard ML, Sly P, Brenan S, Ryan G. Macrolide antibiotics in diffuse
interest in the subject of this manuscript; P.A.C. has received grant funding of
panbronchiolitis and in cystic fibrosis. Eur Respir J 1997;10:2926.
22. Gorrini M, Lupi A, Viglio S, Pamparana F, Cetta G, Iadarola P, Powers
Yates, Murphy, Forrest, et al.: Macrolide Therapy in BOS
JC, Luisetti M. Inhibition of human neutrophil elastase by erythromy-
30. Yates B, Ward C, Murphy D, Forrest I, Fisher AJ, Lordan J, Dark JH,
cin and flurythromycin, two macrolide antibiotics. Am J Respir Cell
Corris PA. Azithromycin reverses airflow obstruction in established
Bronchiolitis Obliterans Syndrome (BOS) following lung transplanta-
23. Ordonez CL, Stulbarg M, Grundland H, Liu JT, Boushey HA. Effect of
tion. Proc Am Thorac Soc 2005;2:A893.
clarithromycin on airway obstruction and inflammatory markers in
31. Takizawa H, Desaki M, Ohtoshi T, Kawasaki S, Kohyama T, Sato M,
induced sputum in cystic fibrosis: a pilot study. Pediatr Pulmonol
Tanaka M, Kasama T, Kobayashi K, Nakajima J, Ito K. Erythromycin
modulates IL-8 expression in normal and inflamed human bronchial
24. Shimane T, Asano K, Suzuki M, Hisamitsu T, Suzaki H. Influence of a
epithelial cells. Am J Respir Crit Care Med 1997;156:266–271.
macrolide antibiotic, roxithromycin, on mast cell growth and activation
32. Yamasawa H, Oshikawa K, Ohno S, Sugiyama Y. Macrolides inhibit
in vitro. Mediators Inflamm 2001;10:323–332.
epithelial cell-mediated neutrophil survival by modulating GM-CSF
25. Spencer D. Macrolide antibiotics in diffuse panbronchiolitis and in cystic
release. Am J Respir Cell Mol Biol 2004;30:569–575.
fibrosis. Eur Respir J 1998;11:1428.
33. Kanai K, Asano K, Hisamitsu T, Suzaki H. Suppression of matrix metallo-
26. Gotfried MH. Macrolides for the treatment of chronic sinusitis, asthma,
proteinase production from nasal fibroblasts by macrolide antibiotics
and COPD. Chest 2004;125:52S–60S.
in vitro. Eur Respir J 2004;23:671–678.
27. Gerhardt SG, McDyer JF, Girgis RE, Conte JV, Yang SC, Orens JB.
34. Schultz MJ. Macrolide activities beyond their antimicrobial effects:
Maintenance azithromycin therapy for bronchiolitis obliterans syn-
macrolides in diffuse panbronchiolitis and cystic fibrosis. J Antimicrob
drome: results of a pilot study. Am J Respir Crit Care Med 2003;
35. Tateda K, Comte R, Pechere JC, Kohler T, Yamaguchi K, Van Delden
28. Verleden GM, Dupont LJ. Azithromycin therapy for patients with bron-
C. Azithromycin inhibits quorum sensing in Pseudomonas aeruginosa.
chiolitis obliterans syndrome after lung transplantation. Transplanta-Antimicrob Agents Chemother 2001;45:1930–1933.
36. Redmund KF GZ, Hofer M, Reichsteiner T, Vogt P, Russi EW, Boehler
29. Yates B, Ward C, Murphy D, Forrest I, Fisher AJ, Lordan J, Dark JH,
A. Clarithromycin has a preventative effect on chronic graft rejection
Corris PA. Azithromycin reverses airflow obstruction in established
[abstract]. Eur Respir J 2004;24:465s.
Bronchiolitis Obliterans Syndrome (BOS) following lung transplanta-
37. Estenne M, Hertz MI. Bronchiolitis obliterans after human lung trans-
tion. J Heart Lung Transplant 2005;24:S102.
plantation. Am J Respir Crit Care Med 2002;166:440–444.
Decreased gyrification in major depressive disorderYuanchao Zhanga,b, Chunshui Yuc, Yuan Zhoub,d, Kuncheng Lic, Chong Lia,band Tianzi JiangbStructural and functional abnormalities have been extensivelyreported in major depressive disorder, but possible changes inKeywords: complexity, connectivity, cortical folding, local gyrification index,cortical folding have not yet been explored in this
DOSSIER N'16: Reflux gastroœsophagien chez une asthmatique Madame V. B., 40 ans obèse, souffre d'un asthme sévère depuis l'adolescence et qui est actuellementcortico-dépendant. Elle prend 15 mg de prednisone chaque jour depuis six mois, en raison de l'échec detoutes les autres thérapeutiques. L'enquête allergologique a retrouvé des IgE spécifiques dirigées contredes acariens et de
 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
References
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
References