Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Obesity
Learning Objectvies: 1. To understand the impact of obesity on general health; 2. To appreciate the causes of obesity in relation to lifestyle; 3. To understand the role of leptin in managing appetite; 4. To appreciate the different treatment options when managing a patient with obesity.
The prevalence of obesity has increased dramatically over the last two decades
throughout the world and is associated with a range of medical and psychological
complications. It is now recognized that obesity is one of the most important public
health problems of our time. Despite this, the trend of increasing obesity continues,
indicating that current public health measures to prevent obesity are failing.
Although there is a high degree of heritability for obesity, the rapid rise in the
prevalence of obesity suggests that environmental factors, such as altered diets and
decreased energy expenditure, are more important in the change in obesity patterns
within countries. Body weight is tightly regulated such that even small mismatches of
less than 100 kcal/ day in energy intake and expenditure may result in massive
obesity. Despite this, the management of the individual with obesity is challenging.
There is much pessimism regarding weight reducing programmes and it has been said
that most obese people do not enter treatment, most who do fail to lose weight and
Normal weight and degrees of either overweight or underweight are defined by the
World Health Organization using the body mass index. The definition of obesity and
overweight, as well as underweight, are based on the observation that mortality is
related to body mass index with mortality being lowest within the BMI range of 20 to
25kg/m2 and increasing at BMIs above and below this range. The effect of BMI on
mortality may have been overestimated because of the effect of smoking and
consequent illness and clinical disorders causing weight loss. These data are based on
white European subjects, and for individuals of South Asian ethnicity, the upper limit
It is estimated that obesity reduces life expectancy by round 9 years and accounts for
30000 deaths in the UK per annum. It costs the UK National Health Service £480
million or 1.5% of total expenditure. In addition, indirect costs are probably £2
billion. Overweight and obesity are also associated with a number of metabolic and
cardiovascular complications, musculoskeletal disease and several cancers,
accounting for 18million days of sickness absence per annum
Body mass index is calculated according to the following formula:
Weight in kilograms /(height in metres)2
• UnderweightBMI<18.5kg/m2 • Normal weight BMI18.5-25kg/m2 • Overweight >25 kg/m2 • Obesity BMI >30 kg/m2 • Morbid obesity BMl>40 kg/m2•
Obesity increases the risk of diabetes, dyslipidaemia and insulin resistance by more
than threefold while increasing coronary heart disease and hypertension two to
threefold. It is estimated that up to 80% of all new cases of diabetes can be attributed
to obesity. The risk of developing type 2 diabetes increases across the normal range,
such that the risk of diabetes in a middle-aged woman whose BMI is greater than
35kg/m2 is 93.2 times greater than woman whose BMI is below 22.5 kg/ m2.
There is compelling evidence that our society discriminates against 'fat people' and
this is damaging to the psychological well-being of obese individuals. Obese women
are likely to leave school earlier, are less likely to be married and have higher rates of
household poverty than women who are not overweight. These findings are
independent of baseline socioeconomic status and are not seen in people with other
chronic conditions such as asthma or musculoskeletal abnormalities.
Limitations of using BMI
As the health risks associated with obesity relate to an excess storage of body fat, and
in particular visceral fat, certain individuals will be misclassified with body mass
index. For any given BMI, women have a higher percentage of body fat than men.
This can lead to the anomalous situation where a lean young male bodybuilder may
have an identical body mass index to a middle-aged obese woman. Nevertheless,
across populations, body mass index correlates well with percentage body fat making
Body fat may be preferentially located in the abdomen (central obesity) or
surrounding the hips and thighs (peripheral obesity). Central obesity is associated with
the metabolic syndrome and is a better predictor of health risk; at the same level of
obesity, the more visceral fat, the greater the risk of developing cardiovascular and
metabolic complications of obesity. Differences in the distribution of body fat explain
why individuals from Asian backgrounds are at higher risk of the complications of
obesity for any given BMI than white Europeans, as Asians tend to have greater
central fat distribution. There are also gender differences in body fat distribution with
most women developing peripheral obesity while men develop central adiposity.
The use of the waist measurement can be used to identify those at high risk of
developing the metabolic complications of obesity, particularly if combined with a
fasting triglyceride concentration. Waist measurements of 100 to 102 cm in men and
88 to 90 cm in women alone provide useful reference values to identify obese patients
who may be at high risk for chronic metabolic diseases. If hypertriglyceridaemia
(>2.0mmol/L) is also present, over 80% of men with waist measurements greater than
90 cm will be at risk of the metabolic syndrome.
Obesity trends
The WHO MONICA project has been following obesity trends in 21 countries among
randomly selected middle-aged participants from the early 1980s to the mid-1990s.
Mean BMI as well as the prevalence of overweight has increased in virtually every
Western European country, Australia, USA and China.
Within the UK, the prevalence of obesity in adults has almost trebled since 1980, such
that in 2002, 23% of men and 25% of women were obese. The prevalence of obesity
among children is lower but the increase in the prevalence of overweight is similar to
the rise in obesity in adults. Obesity rates are higher in low social classes and in some
ethnic minority groups, particularly from South Asia.
The Centers for Disease Control's Behavioral Risk Factor Surveillance System
(BRFSS) provides dramatic evidence to demonstrate the continuing rise in the
prevalence of obesity within the United States. Each year, state health departments
use standard procedures to collect data through a series of monthly telephone
interviews with US adults. In 1991, four states had obesity prevalence rates of 15 to
19% and no states had rates at or above 20%. In 2003, 15 states had obesity
prevalence rates of 15 to 19%; 31 states had rates of 20 to 24%; and four states had
rates greater than 25%. As these data rely on self-reported height and weight, it is
likely that these represent underestimates of the true prevalence of obesity.
Causes of obesity
The causes of obesity are multifactorial, ranging from purely genetic conditions, such
as leptin deficiency, to entirely environmental conditions. It is, however, certain that
obesity can only occur when energy intake remains greater than energy expenditure
for a long period of time. Thus, if either energy intakes increases, or energy ex-
penditure decreases or both, the individual will gain weight. Both energy intake and
expenditure are affected by internal homeostatic mechanisms as well as external
Given the diversity of factors affecting energy balance, it is remarkable how well
body weight can be regulated. Most adults are able to maintain their body weight to
within a few kilograms over 40 or more years in spite of having eaten in excess of 20
tonnes of food. Even in individuals who become obese the mismatch between energy
intake and energy expenditure is extremely small. Daniel Lamberts lived in
Leicestershire, UK during the 18th century and earned a living by exhibiting himself
as a natural curiosity, having reached the weight of 700pounds (320 kg). It is
estimated that when he died at the age of 39, he weighed 52 stone 11 pounds (336 kg),
of which approximately 230 kg would have been fat, containing approximately 2
million kcal. Assuming that there was progressive weight gain throughout his life, the
excess consumption would have been only around 140 kcal/ day, equivalent to an
Appetite is largely regulated by the ventromedial and lateral hypothalamus, with the
ventromedial hypothalamus being a satiety centre and the lateral hypothalamus being
thought of as a hunger centre. Lesions in the lateral hypothalamus cause complete
cessation of feeding while stimulation of this area leads to overeating. The reciprocal
is seen in the ventromedial hypothalamus. The neurobiology of appetite control is
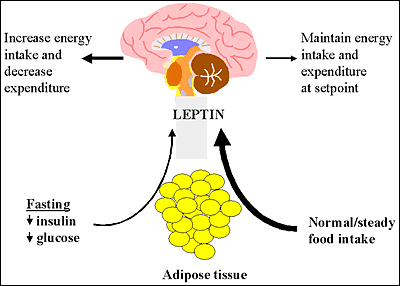
only now being unravelled. The discovery of adipose tissue hormone, leptin, provided
a new paradigm for our understanding of the control of body weight. Under normal
circumstances, circulating leptin concentrations increase as fat mass increases and
Leptin, identified in 1994, is secreted from adipocytes and signals to the brain to
regulate fat mass. Leptin is actively transported across the blood-brain barrier and
reaches the hypothalamus, where it binds to specific leptin receptors located on the
surface of neuropeptide Y (NPY) containing cells. NPY has a powerful stimulating
effect on appetite and leptin suppresses the secretion of NPY, leading to suppression
Thus as fat mass increases, the increased leptin suppresses NPY and appetite
decreases. This provides a classical endocrine negative feedback mechanism by which
appetite and basal metabolic expenditure is regulated in response to changing levels of
demonstrated by studies carried out in mice
that had defective leptin secretion and who
developed severe obesity – the mouse on the
right demonstrates this (in case you weren’t
Abnormalities in the leptin receptor also led to severe obesity. This led to the hope
that abnormalities in leptin action may be responsible for human obesity. While rare
genetic abnormalities in humans in leptin and its receptor have been identified in
cases of severe, early-onset obesity, in most situations leptin levels increase in obesity
and treatment with leptin does not lead to a fall in body weight. This is in contrast to
the rare individuals with leptin deficiency whose body mass index falls dramatically
Ghrelin acts as an appetite-stimulating hormone and is implicated in both short- and
long-term appetite and body weight regulation. It is secreted from the stomach and
circulates in the blood stream where its levels rise and fall before and after meals,
respectively, in response to hunger levels. Ghrelin stimulates food intake by activating
NPY neurons, which express ghrelin receptors, thereby balancing inhibitory signals
received from insulin and leptin. Individuals suffering from Prader-Willi syndrome, a
genetic disorder characterized by a chronic feeling of hunger that leads to obesity,
The contribution of genetic factors has been shown from twin, family and adoption
studies, which suggest that up to 70% of the variance of body mass index is accounted
for by genetic variance. Over the last decade, in addition to genetic mutations in leptin
and its receptor, a number of other human genes have been identified in which major
mis-sense or nonsense mutations have caused severe, early-onset obesity, usually
through the disruption of normal appetite control mechanisms. Although these cases
only represent a minority of all obesity, these studies will begin to identify the critical
molecular components of the human energy balance regulatory systems, which should
allow the targeting of more effective therapies in the future.
Despite the strong contribution of genetics to the development of obesity, the current
obesity epidemic cannot be explained by genetics alone. The change in obesity
patterns has arisen as the result of an adverse environment interacting with a
Dietary intake
The National Food Survey in United Kingdom provides the longest running
continuous survey of household consumption in the world. This has shown that, over
the last 50 years, food consumption within the home has decreased. At first sight these
data appear to be paradoxical until it is remembered that as much as 50% of all food is
consumed outside the home. Since the Second World War, within Europe more food
is produced than is required. This has led to intense competition and incentives to bulk
buy; there can be few people who have never taken advantage of 'two for the price of
one' offers, or the better value 'jumbo' pack.
The National Food Survey has also indicated that there are changes in the types of
food that we are eating. There has been a shift from carbohydrate to fat consumption.
This is important because most individuals regulate their meals size according to
weight or volume rather than caloric intake. Fat contains approximately 9 kcal/ g
while carbohydrate and protein contain 4 kcal/ g. Short-term metabolic studies show
that when the fat content of the diet is increased, individuals continue to eat the same
quantity of food and consequently move into positive energy balance.
There is some evidence from cross-sectional and longitudinal studies that the
proportion of energy consumed as fat is linked with an increase in the prevalence of
obesity. More recently, however, particularly in the UK and US, there has been a
decline in the proportion of energy consumed as fat, while the prevalence of obesity
continues to rise. This may reflect the relatively long lag phase in the development of
obesity and so it may be many years before this dietary change affects the prevalence
We have evolved to undertake vigorous physical activity and therefore it should be
unsurprising that inactivity is associated with ill health. Total energy expenditure is
the sum of our basal metabolic rate, dietary-induced thermogenesis, adaptive
thermogenesis, such as shivering, and physical activity. Of these, physical activity
offers the greatest scope for an individual to increase their energy expenditure.
Physical activity can be defined as any bodily movement produced by skeletal muscle
which results in energy expenditure and can be subdivided into different components,
such as exercise or sport. Activity can be also divided according to its intensity and
duration. Low-intensity activities may include walking or household work while more
intense activities may include running or cycling faster than 10 miles an hour or up
hills. Sedentary behaviour, such as television viewing, is also significant when
considering weight gain as it constrains the opportunity to be active and therefore
Physical inactivity is a major determinant of the current obesity epidemic. Several
studies have shown that physically active people have lower levels of body fat and
weight than inactive people. There are also strong relationships between indicators of
inactivity, such as television viewing and car ownership, and secular trends in obesity.
Unfortunately, epidemiological studies have shown that we are becoming
progressively less active. The Allied Dunbar National Fitness Survey, undertaken in
1995, indicated that 29% of men and 28% of women were classed as sedentary while
only 16% of men and 5% of women participated in regular vigorous activity.
Inactivity increases with age but social class differences are not strong because
occupational activity is often balanced with leisure time activity. In the US, 60% of
adults were not regularly active and 25% reported no significant activity at all.
Similarly, children are also becoming increasingly inactive.
Technological advances have reduced our physical activity in many spheres. The
increasing number of cars has reduced the amount of physical activity we undertake
travelling to and from work. It is estimated that household appliances have reduced
our energy expenditure by around 500kcal/day within the home. These trends have
meant that we have endeavoured to compartmentalize our exercise into 30 to 40 min
in the gym two or three times a week rather than focusing on increasing our energy
As well as eating because we need to eat, many of us also eat for pleasure. Much of
the research into obesity has been concerned with the former homeostatic control of
eating rather than focusing on the latter hedonistic reasons why we eat. Yet these two
aspects of eating are complementary and have two different CNS systems controlling
There is much to be learnt from studying the eating behaviours of people who gain
weight. It is known that overweight individuals select more energy-dense food,
display enhanced hunger traits with less satiety and eat larger and more frequent
meals. Their eating behaviour is also less inhibited. Individuals who tend to gain
weight have a greater readiness to eat and will eat opportunistically. There are differ-
ences in the timing of eating; obese individuals tend to eat more in the afternoon and
less in the morning. In contrast, enjoyment from food is seen as being less important
in those who do not gain weight and health rather than taste becomes a more
Despite the apparent simplicity of the solution for the prevention of obesity, there is
little evidence of the efficacy of health education programmes within the general
population. Education alone is probably insufficient and behaviour modification is
also needed. Healthcare professionals need to take obesity seriously and must
collectively support obesity prevention strategies to prevent the undermining of
A public health and governmental response is also needed to reduce the obesity
epidemic. This could include legislation or a more 'ecological' approach in which
there is a co-ordinated strategy to influence the individual by education and behaviour
change and the toxic environment through economic, physical and sociocultural
Management of the individual with obesity
The major aim of a weight-management programme is to improve health by red ucing
morbidity and mortality associated with obesity rather than simply lowering weight
and adiposity. A 10% weight loss is associated with a major reduction in death and
The scale of the problem means that we are unable to treat all patients with obesity
and therefore it is important to select patients that we are most likely to help.
Characteristics of patients likely to lose weight during a weight-management
• High initial body mass • High central obesity • High energy intake • Initial weight loss
Early weight loss probably reflects the patient's ability to comply with the weight-
management programme. Patients need to be well motivated to undertake the lifestyle
changes. High self-esteem and the acceptance of the need to change also predict
weight loss. This is particularly challenging in the arena of mental illness where
obesity may well complicate the mental state of the patient.
It is important to set appropriate goals to prevent disappointment and frustration
during the programme. A 10% weight loss is an appropriate goal because it is
achievable, results in significant health benefits and can be maintained. However, in
one study when most patients were asked how much weight they would like to lose,
only 1 % reported they would be happy with a weight loss of less than 10% while
63% expected to lose more than 20% of weight. The natural history of body weight
throughout a lifetime is a gradual increase, and therefore the first aim of a weight-
management programme is to prevent further weight gain before moving on to weight
Patient should also be aware of the long-term challenge of weight loss. In the same
way that weight gain occurred over many years, a lifelong change to their lifestyle is
needed to reduce weight. Patient should be encouraged not to think of short-term
fixes. A significant portion of our total energy intake is made up from the basal
metabolic rate. If energy intake falls below basal metabolic rates, strong protective
adaptations occur to try to maintain weight. The patient feels lethargic, tired and
listless and will be unable to maintain this situation for any length of time. Too great a
calorie deficit will therefore lead to failure. On the other hand if a deficit of around
500 kcal is advocated, the patient can lose around 1 kg of weight per week and this is
Dietary strategies
There is a huge popular literature about diets that will aid weight loss. Most of these
diets fail to appreciate that nutrition is a demand led process and therefore any diet
should meet the requirements of the body. There is a need to include both fats and
carbohydrates as energy supplies and any diet that excludes one or other of these
components will create a mismatch between supply and demand. Diets need to be
sustainable over the long-term and most diets that exclude many different food types,
such as the Atkins or Ornish diet, cannot be maintained for more than several months.
The first aim of dietary advice therefore must be to ensure that the individuals eat
sufficient food to meet their metabolic needs. Patient should be advised to avoid
extreme eating restraints and dieting. In order to reduce calorie consumption, two
dietary changes should be considered: the types of food should be changed and
portion sizes reduced. A systematic review of all dietary interventions lasting greater
than 1 year found that there is little evidence to support the use of diets apart from low
fat diets for weight reduction. Low fat diets for up to 36 months resulted in modest
weight losses of around 3.5 kg. The consumption of low-energy-dense foods and
sweeteners may also reduce meal energy intake.
Portion size is also extremely important. There is good evidence that energy intake is
proportional to the amount of food available at mealtimes and by reducing portion
size energy consumption falls. Over the last decade the average size of dinner plate in
the United States restaurant has gone up from 9 inches to 12 inches. The same volume
of food on a larger plate appears smaller and therefore this will lead to over-
consumption while the use of a small plate is a useful means by which patients can
It is important to re-establish 'normal' eating behaviour and attitudes towards food.
Many people eat for reasons that have nothing to do with hunger. For example, people
might eat from boredom, to cope with sadness or to be sociable. Encouraging healthy
eating patterns can lead to a reduction in energy intake. It is important that while food
is consumed, the individual's attention is focused on the food. If the attention is
divided, such as by working at a computer, the reward gained from eating is reduced
and therefore people eat more. It is important that food does not become associated
with other activities, such as watching television, because this will lead to less healthy
eating behaviours. Patients should be advised to eat only at a dining-room or kitchen
table at mealtimes. Cravings for food are often short lived and therefore a useful
strategy can be to distract the patient with an alternative activity such as a 5-min walk
when a craving occurs. The value of commercial weight loss programmes has not
been fully established but they may lead to greater weight loss than an individual's
Exercise
Exercise can play an important part in a weight-management programme. While high
energy expenditure can outstrip energy intake and therefore promotes weight loss in
its own right, exercise also has a role in the prevention of weight regain when
combined with dietary interventions. It is important that patients decrease the amount
of time that they spend sitting or occupied in sedentary activities. Low intensity
activity is also of great importance; for example an 80-year-old patient with agitated
Alzheimer's disease will expand more calories per day than an Olympic athlete
because the patient with Alzheimer's is walking for nearly 24 h every day. The total
time spent active is important and exercise does not need to be undertaken in a single
period. Patients need to think about ways of including physical activity in their
everyday lives. This can be achieved in many areas; for example patients can be
encouraged to use the stairs rather than lifts, to get off the bus one stop early, or to
park at the far end of the car park rather than right next to the door. Physical activity
needs to fit in with daily life and the functional capabilities of individual and ideally
should be pleasurable. The most appropriate type of exercise that patients can
undertake is the one that will still be pursued a decade later.
Pharmacological treatment of obesity has a chequered history and many physicians
still regard these drugs with suspicion and scepticism. Whilst it is true that the
currently available drugs are relatively ineffective when used alone, when used in
combination with lifestyle and behavioural modification programs, they are a useful
adjunct in the management of obesity. The drugs that are currently available can be
divided into two main categories, those acting on the gastrointestinal system, and
centrally acting drugs which affect appetite. The three drugs that are currently
available for the management of obesity are:
• orlistat, which is a pancreatic lipase inhibitor • sibutramine, which is a serotonin and noradrenaline reuptake inhibitor. • rimonabant, which is an endocannabinoid receptor antagonist
Orlistat inhibits pancreatic and gastric lipases, thereby reducing ingested triglyceride
hydrolysis. It produces a dose-dependent reduction in dietary fat absorption that is
near maximal at the currently available dose of 120 mg three times a day. In clinical
trials lasting up to 4 years it leads to modest weight loss of up to 10%. This weight
loss is associated with a reduction in other cardiovascular risk factors including waist
circumference, blood pressure, dyslipidaemia and hyperglycaemia. In patients with
impaired glucose tolerance, it reduces the risk of incident diabetes by 37% over and
above the effect of lifestyle intervention alone. In patients with pre-existing diabetes,
many may be able to reduce or discontinue their oral hypoglycaemic medication.
The main limiting factor for the use of orlistat is the development of gastrointestinal
side-effects secondary to fat malabsorption. These include loose or liquid stools,
faecal urgency and anal leajage, and can be associated with fat soluble vitamins
malabsorption. As the consumption of a high fat diet will inevitably lead to severe
gastrointestinal side-effects, it is important that the prescription of orlistat is ac-
companied by behavioural and dietary advice. Prior to the use of orlistat, it is
important to educate the patient about the drug's mode of action and the dietary
changes needed to reduce the side-effects. As facilities may not always be available
locally, Roche, who manufacture the drug, have established a free telephone and
online patient support programme that has been shown to improve the compliance
with drug therapy as well as achieving greater weight loss.
When orlistat was first introduced into the United Kingdom, its license limited its
usage to 2 years. However, as longer studies have been reported and there is a greater
appreciation of the chronic relapsing nature of obesity, this restriction has now been
removed and patients can continue to use the drug as long as it remains effective. It is
important to note that the drug should not be considered ineffective because weight
loss has stopped, provided the new lowered weight is maintained. Discontinuation of
the drug at this stage may well lead to weight regain. There is no published literature
to suggest that the use of orlistat is associated with dependency on the drug.
Sibutramine is a centrally acting serotonin and noradrenaline reuptake inhibitor
which leads to diminished appetite and decreased food intake. Clinical studies
have shown that patients lose up to around 10% of body weight before reaching a
plateau. If the drug is discontinued, weight is then regained. The weight loss is
associated with a reduction in waist circumference, improved lipid profile and
decreased insulin resistance. The noradrenergic effects of sibutramine can cause
an increase in heart rate and blood pressure. However, this may be offset by the
reduction in blood pressure that occurs with weight loss. Other side-effects
• drymouth • constipation • insomnia • irritability • unusual impatience or excitation • headache • rhinitis and nausea
Within the UK, weight reducing drugs are recommended for use in patients whose
BMI is greater than 30kg/m2 or in patients with comorbidity whose BMI is greater
than 28kg/m2. Initially, the drug should be used for a 3-month trial period and
should only be continued if the patient loses more than 5% of body weight.
Furthermore, it should be reconsidered if the patient has not lost more than 10%
of body weight within the first 6 months.
Rimonabant is an endocannabinoid-1 receptor antagonist, which has been shown
to be effective in reducing body weight and in weight maintenance with up to 2
years of therapy in several phase III studies. It has recently entered clinical
practice. Endocannabinoids increase food intake through endocannabinoid-1
receptor activation and animal experiments show that antagonism of this receptor
reduces sucrose and food intake. Endocannabinoid-1 receptors are also found in
peripheral tissues where activation of this receptor leads to increased insulin
resistance, possibly through alteration in adipocytokine production, such as
decreased adiponectin secretion. Antagonism of this receptor leads to weight loss
and a reduction in features of the metabolic syndrome, with only around half of
the improvements in metabolic profile being explained by changes in weight. The
main side-effects of rimonabant are depressed mood, anxiety and nausea and
therefore caution may be needed if this drug is to be used in patients with
psychiatric illness. There have been small trials of these drugs in the treatment of
schizophrenia and while inconclusive have not shown any worsening of
Several other drugs have been considered for the use in the management of
obesity including pseudophedrine, ephedra, sertraline, yohimbine, amphetamine
or its derivatives, bupropion, benzocaine, threachlorocitric acid, sertraline and
bromocriptine. There is currently a paucity of data about their effectiveness and
these were not recommended in a recent Cochrane systematic database review.
Bariatric surgery
Bariatric surgery is currently the only long-term cure for obesity. There are two
main types of operation to treat obesity. Malabsorption techniques bypass part of
the stomach or small intestine while restrictive surgery lead to reduced dietary
intake by reducing the size of the stomach and therefore improves satiety. The
best evidence for the long-term effects of gastric surgery for obesity comes from
the Swedish Obese Subjects Study where the weight loss after 2 years was
typically between 30 and 40 kg. Quality of life improves dramatically following
surgery and this is associated with major improvements in metabolic side-effects
of obesity. A review of bariatric surgery has also suggested that gastric bypass
surgery is associated with a 99 to 100% prevention of diabetes in patients with
impaired glucose tolerance and an 80 to 90% clinical resolution of diagnosed
At present, obesity surgery is only recommended for those with morbid obesity.
Each patient requires an extensive preoperative assessment which includes a
psychological assessment as surgery will not treat an eating disorder and may lead
to worsening of the mental state if patients are dependent on food.
Conclusions
Obesity has become a major health problem throughout the world. While genetics can
explain much of the variability of body mass index within a given population, it is
environmental changes over the last 50 years that have precipitated the obesity
epidemic. A public health and governmental response is needed to reduce the toxic
environment in which we live. The management of the individual with obesity is
challenging but successful results can be obtained through lifestyle modification when
combined with realistic goals and patient selection. Drug therapy is currently in its
infancy but the use of orlistat or sibutramine is a useful adjunct to weight loss.
Bariatric surgery is the only long-term solution for patients with morbid obesity.
There can no longer be a place for therapeutic nihilism and therefore we need to de-
velop strategies within health settings to promote lifestyles that will both prevent and
Metformin WHAT IS METFORMIN? • Metformin is a medication used to treat type 2 diabetes, which is also known as non-insulin- dependent diabetes mellitus. It works by lowering or regulating the amount of sugar in your blood. WHAT IS THE MOST IMPORTANT INFORMATION I SHOULD KNOW ABOUT METFORMIN? • In rare cases, metformin can cause a serious side effect called lactic acidosis. Lactic
The Golden Pheasant Inn, Plumley Moor Road, Plumley, Restaurant booking recommended, bar reservations not required DISCRETIONARY 10% SERVICE CHARGE MAY BE ADDED TO TABLES OF 8 OR MORE ALL OF THIS IS GIVEN TO OUR HARDWORKING STAFF AND NOT TO THE ‘MANAGEMENT’ THE STARTERS ; TRADITIONAL PRAWN COCKTAIL Succulent North Atlantic Prawns in our homemade seafood sauce CHEF’S HOMEMADE SOUP OF THE
 estimated that when he died at the age of 39, he weighed 52 stone 11 pounds (336 kg),
of which approximately 230 kg would have been fat, containing approximately 2
million kcal. Assuming that there was progressive weight gain throughout his life, the
excess consumption would have been only around 140 kcal/ day, equivalent to an
Appetite is largely regulated by the ventromedial and lateral hypothalamus, with the
ventromedial hypothalamus being a satiety centre and the lateral hypothalamus being
thought of as a hunger centre. Lesions in the lateral hypothalamus cause complete
cessation of feeding while stimulation of this area leads to overeating. The reciprocal
is seen in the ventromedial hypothalamus. The neurobiology of appetite control is
only now being unravelled. The discovery of adipose tissue hormone, leptin, provided
a new paradigm for our understanding of the control of body weight. Under normal
circumstances, circulating leptin concentrations increase as fat mass increases and
Leptin, identified in 1994, is secreted from adipocytes and signals to the brain to
regulate fat mass. Leptin is actively transported across the blood-brain barrier and
reaches the hypothalamus, where it binds to specific leptin receptors located on the
surface of neuropeptide Y (NPY) containing cells. NPY has a powerful stimulating
effect on appetite and leptin suppresses the secretion of NPY, leading to suppression
estimated that when he died at the age of 39, he weighed 52 stone 11 pounds (336 kg),
of which approximately 230 kg would have been fat, containing approximately 2
million kcal. Assuming that there was progressive weight gain throughout his life, the
excess consumption would have been only around 140 kcal/ day, equivalent to an
Appetite is largely regulated by the ventromedial and lateral hypothalamus, with the
ventromedial hypothalamus being a satiety centre and the lateral hypothalamus being
thought of as a hunger centre. Lesions in the lateral hypothalamus cause complete
cessation of feeding while stimulation of this area leads to overeating. The reciprocal
is seen in the ventromedial hypothalamus. The neurobiology of appetite control is
only now being unravelled. The discovery of adipose tissue hormone, leptin, provided
a new paradigm for our understanding of the control of body weight. Under normal
circumstances, circulating leptin concentrations increase as fat mass increases and
Leptin, identified in 1994, is secreted from adipocytes and signals to the brain to
regulate fat mass. Leptin is actively transported across the blood-brain barrier and
reaches the hypothalamus, where it binds to specific leptin receptors located on the
surface of neuropeptide Y (NPY) containing cells. NPY has a powerful stimulating
effect on appetite and leptin suppresses the secretion of NPY, leading to suppression
 Thus as fat mass increases, the increased leptin suppresses NPY and appetite
decreases. This provides a classical endocrine negative feedback mechanism by which
appetite and basal metabolic expenditure is regulated in response to changing levels of
demonstrated by studies carried out in mice
that had defective leptin secretion and who
developed severe obesity – the mouse on the
right demonstrates this (in case you weren’t
Abnormalities in the leptin receptor also led to severe obesity. This led to the hope
that abnormalities in leptin action may be responsible for human obesity. While rare
genetic abnormalities in humans in leptin and its receptor have been identified in
cases of severe, early-onset obesity, in most situations leptin levels increase in obesity
and treatment with leptin does not lead to a fall in body weight. This is in contrast to
the rare individuals with leptin deficiency whose body mass index falls dramatically
Ghrelin acts as an appetite-stimulating hormone and is implicated in both short- and
long-term appetite and body weight regulation. It is secreted from the stomach and
circulates in the blood stream where its levels rise and fall before and after meals,
respectively, in response to hunger levels. Ghrelin stimulates food intake by activating
NPY neurons, which express ghrelin receptors, thereby balancing inhibitory signals
received from insulin and leptin. Individuals suffering from Prader-Willi syndrome, a
genetic disorder characterized by a chronic feeling of hunger that leads to obesity,
The contribution of genetic factors has been shown from twin, family and adoption
studies, which suggest that up to 70% of the variance of body mass index is accounted
for by genetic variance. Over the last decade, in addition to genetic mutations in leptin
and its receptor, a number of other human genes have been identified in which major
mis-sense or nonsense mutations have caused severe, early-onset obesity, usually
through the disruption of normal appetite control mechanisms. Although these cases
only represent a minority of all obesity, these studies will begin to identify the critical
molecular components of the human energy balance regulatory systems, which should
allow the targeting of more effective therapies in the future.
Despite the strong contribution of genetics to the development of obesity, the current
obesity epidemic cannot be explained by genetics alone. The change in obesity
patterns has arisen as the result of an adverse environment interacting with a
Dietary intake
Thus as fat mass increases, the increased leptin suppresses NPY and appetite
decreases. This provides a classical endocrine negative feedback mechanism by which
appetite and basal metabolic expenditure is regulated in response to changing levels of
demonstrated by studies carried out in mice
that had defective leptin secretion and who
developed severe obesity – the mouse on the
right demonstrates this (in case you weren’t
Abnormalities in the leptin receptor also led to severe obesity. This led to the hope
that abnormalities in leptin action may be responsible for human obesity. While rare
genetic abnormalities in humans in leptin and its receptor have been identified in
cases of severe, early-onset obesity, in most situations leptin levels increase in obesity
and treatment with leptin does not lead to a fall in body weight. This is in contrast to
the rare individuals with leptin deficiency whose body mass index falls dramatically
Ghrelin acts as an appetite-stimulating hormone and is implicated in both short- and
long-term appetite and body weight regulation. It is secreted from the stomach and
circulates in the blood stream where its levels rise and fall before and after meals,
respectively, in response to hunger levels. Ghrelin stimulates food intake by activating
NPY neurons, which express ghrelin receptors, thereby balancing inhibitory signals
received from insulin and leptin. Individuals suffering from Prader-Willi syndrome, a
genetic disorder characterized by a chronic feeling of hunger that leads to obesity,
The contribution of genetic factors has been shown from twin, family and adoption
studies, which suggest that up to 70% of the variance of body mass index is accounted
for by genetic variance. Over the last decade, in addition to genetic mutations in leptin
and its receptor, a number of other human genes have been identified in which major
mis-sense or nonsense mutations have caused severe, early-onset obesity, usually
through the disruption of normal appetite control mechanisms. Although these cases
only represent a minority of all obesity, these studies will begin to identify the critical
molecular components of the human energy balance regulatory systems, which should
allow the targeting of more effective therapies in the future.
Despite the strong contribution of genetics to the development of obesity, the current
obesity epidemic cannot be explained by genetics alone. The change in obesity
patterns has arisen as the result of an adverse environment interacting with a
Dietary intake