Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
6suth.cc
The new england journal of medicine
c u r r e n t c o n c e p t s
E. Rand Sutherland, M.D., M.P.H., and Reuben M. Cherniack, M.D.
hronic obstructive pulmonary disease (copd) is a syndrome of
From the Department of Medicine, Nation-al Jewish Medical and Research Center; and
progressive airflow limitation caused by chronic inflammation of the air-
ways and lung parenchyma. The primary physiological abnormality in COPD is Critical Care Medicine, Department of Med-
an accelerated decline in the forced expiratory volume in one second (FEV ) from the
icine, University of Colorado Health Sci-ences Center — both in Denver. Address
normal rate in adults over 30 years of age of approximately 30 ml per year to nearly 60 reprint requests to Dr. Cherniack at 1400
ml per year.2 As shown in Figure 1, the disease course begins with an asymptomatic Jackson St., J-208, Denver, CO 80206. phase in which lung function deteriorates without associated symptoms. The onset
of the subsequent symptomatic phase is variable but often does not occur until the Copyright 2004 Massachusetts Medical Society.
FEV has fallen to approximately 50 percent of the predicted normal value.3 Since sub-
stantial deterioration in airflow has already occurred by the time most patients presentwith symptoms, it is reasonable to conclude that the degree of airflow limitation is onlyone of many factors that govern the onset of symptoms.
Hyperinflation, which occurs at rest and worsens with exercise (Fig. 2), is an addi-
tional physiological abnormality that is commonly seen in patients with moderate-to-severe COPD. It is manifested primarily by an increase in the functional residualcapacity, which places the muscles of respiration at a mechanical disadvantage, there-by increasing the work of breathing and reducing exercise tolerance. Additional physi-ological abnormalities include a reduction in the diffusing capacity for carbon mon-oxide, hypoxemia, and alveolar hypoventilation.
d i a g n o s i s , s t a g i n g , a n d p r o g n o s i s
Because the majority of cases occur in patients who have smoked,4 all current or formersmokers should be considered at increased risk for COPD. Other risk factors, whichaccount for far fewer cases, include a -antitrypsin deficiency,5 airway hyperrespon-
siveness,6 and indoor air pollution.7 Since symptoms may not occur until lung func-tion is substantially reduced, early detection is enhanced by spirometric evaluation ofFEV and forced vital capacity (FVC). Guidelines from the Global Initiative for Chronic
Obstructive Lung Disease (GOLD) state that the airflow limitation in COPD is charac-terized by an FEV value that is less than 80 percent of the predicted normal value and
Currently, most guidelines recommend that practitioners use a combination of in-
formation about symptoms and evidence of impairment of physiological function indetermining the severity of the disease,3,8-10 although the guidelines differ somewhatwith regard to setting thresholds for mild, moderate, and severe disease (Table 1). Thestage of the disease suggests the prognosis, and follow-up data from longitudinal stud-ies indicate that moderate and severe stages of the disease are associated with highermortality.11 However, in the largely asymptomatic group of patients that GOLD3 cate-gorizes as “stage 0, at risk,” only 18.5 percent of the patients progress to more severe
Downloaded from www.nejm.org by ALEXANDRE A. HOLANDA MD on January 30, 2007 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
airflow limitation at 15 years,12 which suggests (including both the indolent and progressive na-that more information is required to predict which ture of symptoms), and a knowledge of the distri-patients with incipient disease will progress rapidly bution and potential overlap of physiological dis-to a more advanced stage.
Most guidelines also state that in addition to
airflow limitation, patients with COPD have an in-
m a n a g e m e n t o f s t a b l e c o p d
complete response to albuterol (change in FEV ,
<200 ml and 12 percent)3,13 and typically do not The major goals of therapy include smoking ces- have evidence of airway hyperresponsiveness (i.e., sation, symptom relief, improvement in physio- an abnormal bronchoconstrictor response to a logical function, and limitation of complications, stimulus such as methacholine). Although these such as abnormal gas exchange and exacerbations features are helpful in distinguishing COPD from of the disease. As summarized in Figure 3, an inte- asthma,3 the distinctions are not entirely clear-cut. grated approach to treatment combines health care Indeed, there is responsiveness to a bronchodila- maintenance and use of drug and supplemental tor in 23 to 42 percent of patients with COPD, de- therapies in a stepwise fashion as the disease pro- pending on the criteria used.14 Furthermore, data gresses. from the Lung Health Study indicate that 59 per- cent of men and 85 percent of women with mod- health care maintenance erate disease (mean [±SD] FEV :FVC ratio, 0.63± Regular Assessment of Lung Function
0.055 percent) have airway hyperresponsiveness.15 It is not yet known whether spirometric screeningThus, although guideline-based spirometric criteria for COPD is cost effective, and evidence-based cri-are useful starting points, differentiation of COPD teria for the optimal frequency of such testing infrom asthma requires careful integration of epi- patients with established disease need to be es-demiologic risk factors (including the patient’s age, tablished. Until more data become available, wesmoking status, and family history), clinical status recommend that spirometry be performed in all
(% of predicted) Symptoms Axis of Progression Figure 1. Deterioration in Lung Function in Patients with COPD.
Symptoms generally develop only after a significant decline in forced expiratory volume in one second (FEV ) has oc-
curred; they progress as lung function deteriorates further.
Downloaded from www.nejm.org by ALEXANDRE A. HOLANDA MD on January 30, 2007 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
patients at risk to detect asymptomatic airflow lim- drug therapy itation; in patients with established disease, spi- Inhaled Bronchodilators rometry should be performed at least annually, and Inhaled bronchodilators are the foundation of more frequently if needed, to assess clinical status pharmacotherapy for COPD because of their ca- or the response to therapy.
pacity to alleviate symptoms, decrease exacerba-tions of disease, and improve the quality of life.21-25
These drugs also improve airflow and hyperinfla-
Abstinence from smoking results in a sustained tion (Fig. 2),26,27 thereby decreasing the work of50 percent reduction in the rate of lung-functiondecline in patients with COPD,2 and smoking ces-sation is the only intervention known to be so ef-
Total Lung
fective in modifying the disease. Unfortunately,
Capacity
achieving and maintaining smoking cessation inpatients with COPD is a challenge. Approximately35 percent of the subjects in the Lung Health Studyachieved abstinence at one year, but only 22 percent
reported continued abstinence at five years with a
Ventilation
regimen combining nicotine replacement (avail-able in the form of chewing gum, inhaler, spray,and transcutaneous patch), behavioral counsel-ing, and frequent maintenance visits.16 Sustained-release bupropion is also effective, although thelikelihood of sustained abstinence among patients
Patients
who have COPD is lower with bupropion than with
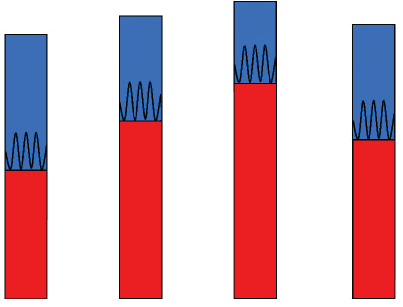
Patients with COPD Patients with COPD during Exercise Figure 2. Pulmonary Hyperinflation in Patients with COPD.
Although there is little evidence of a direct benefit
As compared with healthy patients, patients with COPD have pulmonary hy-
of vaccination in patients with COPD, we recom-
perinflation with an increase in functional residual capacity (red) and a de-
mend that pneumococcal vaccination and annual
crease in inspiratory capacity (blue). This condition increases the volume at
influenza vaccination be offered to all patients in
which tidal ventilation (oscillating line) occurs and places the muscles of res-piration at mechanical disadvantage. Hyperinflation worsens with exercise
an attempt to reduce both disease-specific mortali-
and therefore reduces exercise tolerance (dynamic hyperinflation). Inhaled
ty and mortality from all causes.18,19 Administra-
bronchodilators improve dynamic hyperinflation, as well as hyperinflation at
tion of the influenza vaccine does not appear to in-
rest (not shown), thereby reducing the work of breathing and increasing exer-
crease adverse outcomes in patients with COPD in
Table 1. A Comparison of Four Sets of Staging Criteria for COPD.* American Thoracic Society European Respiratory Society British Thoracic Society (1997)10 GOLD (2003)3
* GOLD denotes Global Initiative for Chronic Obstructive Lung Disease, and FEV forced expiratory volume in one second (shown as a percent-
age of the predicted normal value). In the Symptoms columns, NA denotes not applicable (staging is based on physiology only), – no symptoms, ± variable symptoms, + mild-to-moderate symptoms, ++ symptoms that limit exertion, and +++ symptoms that limit daily activities.
Downloaded from www.nejm.org by ALEXANDRE A. HOLANDA MD on January 30, 2007 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
breathing and improving exercise tolerance. Para-
Inhaled bronchodilators can be grouped ac-
doxically, improvement in function resulting from cording to mechanism or duration of action (Ta-the administration of bronchodilators is not always ble 2). Short-acting b -adrenergic–receptor agonists
reflected by changes in FEV and FVC, and mea- (e.g., albuterol sulfate) and cholinergic-receptor
surement of lung volumes or inspiratory capacity antagonists (e.g., ipratropium bromide) result inmay be necessary to document physiological im- bronchodilation for four to six hours.28 Long-act-provement.27
ing b -adrenergic–receptor agonists such as for-
Supplemental Therapy Stepwise Drug Therapy
Combination of anticholinergic and b-agonist bronchodilator
Health Care Maintenance
Pneumococcal and annual influenza vaccination
Symptoms Figure 3. An Algorithm for the Treatment of COPD.
The components of COPD therapy include health care maintenance, drug therapy, and supplemental therapy. Because patients with reduced lung function may be asymptomatic, spirometry is indicated to diagnose asymptomatic reduction in lung function in at-risk patients. Treatment should be initiated when reduced lung function is demonstrated, with or without the presence of symptoms. Smoking cessation should be aggressively pursued in patients across the severity spectrum, and vaccination is an important addition to health care maintenance. Patients may initially require only as-needed therapy with a single short-acting anticholinergic agent or b-agonist. For patients with moderate-to-severe dis-ease, or for those with persistent or increasing symptoms with as-needed bronchodilators, a single regularly scheduled, long-acting inhaled bronchodilator of either pharmacologic class or the regularly scheduled combination of a short- or long-acting anticholinergic agent and a b-agonist is preferred. For patients treated with a long-acting inhaled bronchodi-lator, a short-acting agent should be prescribed concurrently for rapid treatment of acute symptoms (box with dashed outline). The addition of pulmonary rehabilitation to treatment regimens will reduce symptoms and improve exercise performance, and the addition of theophylline or an inhaled corticosteroid (or both) to optimal inhaled bronchodilator therapy may provide additional benefits. Patients with moderate or severe disease should be tested for hypoxemia, and it should be aggressively treated if present. Lung-volume–reduction surgery and transplantation are options for a sub-group of patients with very severe disease.
Downloaded from www.nejm.org by ALEXANDRE A. HOLANDA MD on January 30, 2007 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
moterol fumarate and salmeterol xinafoate have al improvement in lung function and symptomsan effect for 8 to 12 hours, and the long-acting an- when added to inhaled bronchodilators.35,36 Sinceticholinergic agent tiotropium bromide has a dura- theophylline may be toxic, frequent monitoring fortion of effect of more than 24 hours. In stable dis- supratherapeutic levels, adverse drug reactions, andease, administration by means of a metered-dose drug interactions is critical. or dry-powder inhaler is preferred.
For patients with mild airflow limitation and in- Inhaled Corticosteroids
termittent symptoms, a single short-acting inhaled The appropriate role of inhaled corticosteroids inbronchodilator relieves symptoms and improves COPD is controversial. Many studies have shownairflow. Albuterol and ipratropium are equally ef- that inhaled corticosteroids do not substantiallyfective with regard to bronchodilation, symptom modify airway inflammation in COPD, and fourscores, and the rates of treatment failure and can be large, long-term clinical trials37-40 comparing in-used interchangeably for mild disease as the first haled corticosteroids with placebo found that thesestep in a series of measures for treating patients drugs do not appreciably alter the rate of declinewith COPD (Fig. 3).28-31
in lung function. This absence of physiological
Since most patients have at least moderate air- effects, as well as differences in inflammatory phe-
flow limitation when first evaluated, they are likely notype between COPD and asthma,41 has led manyto require regularly scheduled bronchodilation3 investigators to conclude that these drugs are inef-and to derive benefit from a long-acting broncho- fective in COPD. dilator as initial therapy. Formoterol, salmeterol,
However, some of the same trials have demon-
and tiotropium all have an equivalent peak bron- strated that treatment with inhaled corticosteroidschodilator effect but have a prolonged duration of alleviates patients’ symptoms,40 reduces the fre-effect, which may explain the superiority of these quency of exacerbations,39 and improves health sta-drugs to short-acting bronchodilators in reducing tus.42 These studies relied on FEV as the primary
symptoms and the frequency of exacerbations and outcome variable and did not evaluate such physio-in improving the quality of life.22,23,25 Treatment logical variables as hyperinflation, which may havemay be initiated with either a long-acting anticho- a greater effect on clinical status than the FEV does.
linergic agent or a b-agonist, since there is little Moreover, these studies may not have been pow-evidence to suggest clinically significant differenc- ered adequately to detect small differences in thees between pharmacologic classes. Long-acting in- rate of decline in the FEV .43 In fact, the effect of
haled bronchodilators are not appropriate for the cigarette smoking in blunting the spirometric re-treatment of acute symptoms, so a short-acting sponse to corticosteroids, as was recently observedbronchodilator should also be prescribed for acute in a study involving patients with asthma,44 mayrelief of symptoms (Fig. 3).
have affected the response to inhaled corticoste-
Combination bronchodilator therapy (an anti-
cholinergic agent plus a b-agonist) may be consid-ered for patients in whom a single inhaled bron-
Table 2. Duration and Administration of Inhaled Bronchodilators.
chodilator has failed to provide adequate relief. Duration Usual Dose*
The combination of albuterol and ipratropium
Short-acting
provides greater bronchodilation than either drug
used alone,28 and similar benefits are obtained by
combining long-acting b-agonists with ipratro-
pium.32,33 Although the combination of albuterol
and ipratropium is commonly prescribed for regu-
Long-acting
larly scheduled use, regularly scheduled ipratropi-
um combined with albuterol on an as-needed ba-
sis has been reported to be equally effective.34
If symptoms continue despite combined inhaled-bronchodilator therapy, theophylline may be pre- * MDI denotes metered-dose inhaler, and DPI dry-powder inhaler. scribed because of its capacity to provide addition-
Downloaded from www.nejm.org by ALEXANDRE A. HOLANDA MD on January 30, 2007 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
roids in the studies of COPD, in which smokers received oral prednisolone before fluticasone.39made up 39 to 100 percent of the study population. The overall response to prednisolone was minimalThus, the medical literature suggests that inhaled (a mean increase in FEV of 69 ml) and was unre-
corticosteroids provide clinical benefit to some pa- lated to the patients’ baseline FEV , responsiveness
tients with COPD and that this effect is indepen- to a bronchodilator, subsequent decline in FEV ,
dent of the patients’ FEV response, perhaps op- or response to inhaled fluticasone.48 Thus, although
erating through an improvement in hyperinflation a trial of oral corticosteroids may be useful in de-or a reduction in the frequency of exacerbations.
tecting coexisting asthma, it is a poor predictor
Guidelines recommend that inhaled cortico- of the response to inhaled corticosteroids among
steroids be considered for patients with moder- patients with COPD. Oral corticosteroids should ate-to-severe airflow limitation who have persistent not be used in the routine management of stable symptoms despite optimal bronchodilator thera- disease. py.3 This recommendation is based in large part on the Inhaled Steroids in Obstructive Lung Dis- supplemental therapy ease in Europe (ISOLDE) trial, in which subjects Pulmonary Rehabilitation with a mean FEV of approximately 50 percent of Pulmonary rehabilitation improves patients’ exer-
the predicted normal value had a 25 percent rela- cise capacity, reduces dyspnea, improves the qual-tive reduction in frequency of exacerbations when ity of life,49 and reduces the number and durationtreated with inhaled fluticasone propionate.39 Ex- of hospitalizations related to respiratory disease.50acerbations appear to accelerate the rate of lung- It is appropriate for patients with clinically signif-function decline in COPD,45 and the reduction in icant exertional symptoms and is most effectiveexacerbations seen in the ISOLDE trial supports when delivered as a multifaceted program incor-the use of inhaled corticosteroids to modify the porating individually tailored aerobic physical train-frequency of exacerbations, independently of the ing, comprehensive education about the disease,drugs’ effects on underlying airway inflammation. psychosocial counseling, and nutritional support.51In addition, the observation that the combination Although having a low body-mass index is associat-of inhaled corticosteroids and long-acting b-ago- ed with increased mortality from respiratory diseasenists is superior to placebo or either drug alone among patients with COPD,52 there is no evidencewith regard to lung function, frequency of exacer- that enhanced nutrition improves body weight, lungbations, symptoms, and health status46,47 suggests function, exercise capacity, or survival.53that the use of inhaled corticosteroids should be re-stricted to patients in whom optimal bronchodilator Treatment of Abnormal Gas Exchangetherapy has failed to improve the symptoms, physi- Hypoxemia develops as a result of a worsening ven-ological findings, or frequency of exacerbations.
tilation–perfusion mismatch, and aggressive test-
It is important to recognize that in older pa- ing for hypoxemia is critical, since clinical trials
tients the side effects of inhaled corticosteroids are have shown that mortality is reduced by treatmentnot well understood, and the use of these drugs with supplemental oxygen for 15 or more hours pershould be carefully considered. Since it is difficult to day.54,55 In stable patients, Medicare guidelinespredict accurately which patients will benefit from suggest that oxygen therapy should be initiatedtherapy, clinical and spirometric responses should if the resting partial pressure of arterial oxygen isbe assessed in the months after the initiation of in- 55 mm Hg or lower or if the oxygen saturation ishaled corticosteroids. Treatment should be discon- 88 percent or less. However, these recommenda-tinued if no substantial clinical or physiological tions are based in large part on the inclusion crite-improvement is seen, since there is no evidence ria for the Medical Research Council study54 andthat continuing treatment with inhaled corticoste- the Nocturnal Oxygen Therapy Trial55 and may notroids provides any long-term benefit in such cases. identify all patients who would benefit from sup-
plemental oxygen. For example, supplemental ox-
ygen substantially improves training intensity and
Assessing the spirometric response to a trial of oral exercise tolerance even in patients in whom desat-corticosteroids has been advocated as a means of uration does not occur during exercise.56identifying patients who have a response to inhaled
Supplemental oxygen should be adjusted to
corticosteroids. In the ISOLDE trial, all subjects maintain an oxygen saturation of at least 90 per-
Downloaded from www.nejm.org by ALEXANDRE A. HOLANDA MD on January 30, 2007 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
cent at all times. Since patients may have normal therapy alone. In 2000, a small randomized, con-oxygen saturation at rest but hypoxemia with ex- trolled trial that compared lung-volume–reductionertion or sleep, pulse oximetry and oxygen titra- surgery with medical therapy in patients with se-tion should be performed during all three condi- vere emphysema demonstrated improved lungtions. Worsening hypoxemia during air travel must function, exercise capacity, and quality of life 6 tobe considered, and a general recommendation is 12 months after surgery.61 Subsequently, the Na-that patients requiring oxygen should increase tional Emphysema Treatment Trial found that thetheir oxygen flow rate by 2 liters per minute during addition of lung-volume–reduction surgery to op-flight.57
timal medical therapy and rehabilitation led to
In advanced disease, hypoxemia and hypercap- an overall improvement in exercise tolerance and
nia (alveolar hypoventilation) may occur as a result survival in a subgroup of patients with reduced ex-of an increase in the dead-space fraction, a ventila- ercise tolerance and predominantly upper-lobe em-tion–perfusion mismatch, or an increase in the work physema.62 Overall mortality did not improve,of breathing with enhanced production of carbon however, and mortality was increased in a sub-dioxide. Inhaled bronchodilators can help reduce group of patients with severe physiological impair-the work of breathing and improve gas exchange ment (FEV , ≤20 percent of the predicted normal
in some patients with alveolar hypoventilation. value) and homogeneous emphysema or a carbonTrials of noninvasive positive-pressure ventilation monoxide diffusing capacity no more than 20 per-have been conducted in patients with stable COPD, cent of the predicted normal value.63and although hypercapnia can be improved,58 im-
Single-lung transplantation is an alternative sur-
provement often comes at the cost of increased gical option for patients with end-stage emphyse-hyperinflation.59 A two-year trial of noninvasive ma who have an FEV that is less than 25 percent
positive-pressure ventilation in addition to supple- of the predicted normal value after the administra-mental oxygen in patients with alveolar hypoventi- tion of a bronchodilator and who have such com-lation demonstrated improvements in dyspnea and plications as pulmonary hypertension, marked hy-the quality of life but only small improvements in poxemia, and hypercapnia.64 The surgery does notarterial carbon dioxide levels.60
appear to improve survival significantly in thesepatients, however.65
Supported by a grant (K23 HL04385) from the National Heart,
Lung-volume–reduction surgery can reduce hyper- Lung, and Blood Institute.
Dr. Cherniack reports having served as a consultant for Glaxo-
inflation and should be considered in patients with SmithKline, and Dr. Sutherland having served as a consultant forsevere upper-lobe emphysema and reduced exer- Schering-Plough and having received grant support from Glaxo-cise tolerance who are not faring well with medical SmithKline. r e f e r e n c e s
obstructive pulmonary disease. Am J Respir
National Health and Nutrition Examination
Anthonisen NR, Connett JE, Murray RP.
al. Exposure to biomass smoke and chronic
12. Vestbo J, Lange P. Can GOLD Stage 0
provide information of prognostic value in
Study participants after 11 years. Am J Res-
chronic obstructive pulmonary disease? Am
J Respir Crit Care Med 2002;166:329-32. 13. Lung function testing: selection of ref-
erence values and interpretative strategies. 14. Calverley PM, Burge PS, Spencer S,
Siafakas NM, Vermeire P, Pride NB, et al.
reversibility testing in chronic obstructive
pulmonary disease. Thorax 2003;58:659-64.
(COPD). Eur Respir J 1995;8:1398-420. 15. Tashkin DP, Altose MD, Bleecker ER, et 10. BTS guidelines for the management of
al. The Lung Health Study: airway respon-
chronic obstructive pulmonary disease. Tho-
siveness to inhaled methacholine in smok-
ers with mild to moderate airflow limita-
11. Mannino DM, Buist AS, Petty TL, Enright
tion. Am Rev Respir Dis 1992;145:301-10.
line reactivity predicts changes in lung func-
16. Anthonisen NR, Connett JE, Kiley JP, et
tion over time in smokers with early chronic
in the United States: data from the First
al. Effects of smoking intervention and the
Downloaded from www.nejm.org by ALEXANDRE A. HOLANDA MD on January 30, 2007 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
use of an inhaled anticholinergic broncho-
solution in patients with chronic obstruc-
Venn AJ, Martin RJ. Inhaled corticosteroids
dilator on the rate of decline of FEV : the
tive pulmonary disease: a three-center study.
reduce the progression of airflow limitation
in chronic obstructive pulmonary disease:
30. Ram FS, Sestini P. Regular inhaled short
a meta-analysis. Thorax 2003;58:937-41. 17. Tashkin D, Kanner R, Bailey W, et al. 44. Chaudhuri R, Livingston E, McMahon
Smoking cessation in patients with chronic
of stable chronic obstructive pulmonary dis-
AD, Thomson L, Borland W, Thomson NC.
ease: Cochrane systematic review and meta-
Cigarette smoking impairs the therapeutic
blind, placebo-controlled, randomised trial.
response to oral corticosteroids in chronic
31. Petrie GR, Palmer KN. Comparison of
asthma. Am J Respir Crit Care Med 2003;168:
18. Nichol KL, Margolis KL, Wuorenma J,
Von Sternberg T. The efficacy and cost effec-
45. Donaldson GC, Seemungal TA, Bhow-
tiveness of vaccination against influenza
among elderly persons living in the commu-
32. Wadbo M, Lofdahl CG, Larsson K, et al.
Effects of formoterol and ipratropium bro-
decline in chronic obstructive pulmonary dis-
19. Nichol KL, Nordin J, Mullooly J, Lask R,
Fillbrandt K, Iwane M. Influenza vaccina-
trolled study. Eur Respir J 2002;20:1138-46. 46. Calverley PM, Pauwels RA, Vestbo J, et al.
tion and reduction in hospitalizations for
33. van Noord JA, de Munck DR, Bantje TA,
cardiac disease and stroke among the elderly.
the treatment of chronic obstructive pulmo-
term treatment of chronic obstructive pul-
nary disease: a randomised controlled trial. 20. Tata LJ, West J, Harrison T, Farrington P,
Smith C, Hubbard R. Does influenza vacci-
additive effect of ipratropium. Eur Respir
nation increase consultations, corticosteroid
47. Szafranski W, Cukier A, Ramirez A, et al.
prescriptions, or exacerbations in subjects
34. Cook D, Guyatt G, Wong E, et al. Regu-
Efficacy and safety of budesonide/formot-
with asthma or chronic obstructive pulmo-
lar versus as-needed short-acting inhaled
erol in the management of chronic obstruc-
beta-agonist therapy for chronic obstructive
tive pulmonary disease. Eur Respir J 2003;
21. Higgins BG, Powell RM, Cooper S, Tat-
21:74-81. [Erratum, Eur Respir J 2003;21:
tersfield AE. Effect of salbutamol and ipra-
35. McKay SE, Howie CA, Thomson AH, 48. Burge PS, Calverley PM, Jones PW, Spen-
bronchial reactivity in asthma and chronic
Whiting B, Addis GJ. Value of theophylline
cer S, Anderson JA. Prednisolone response
bronchitis. Eur Respir J 1991;4:415-20.
treatment in patients handicapped by chronic
in patients with chronic obstructive pulmo-
22. Dahl R, Greefhorst LA, Nowak D, et al.
obstructive lung disease. Thorax 1993;48:
nary disease: results from the ISOLDE study.
Inhaled formoterol dry powder versus ipra-
tropium bromide in chronic obstructive pul-
36. ZuWallack RL, Mahler DA, Reilly D, et 49. Lacasse Y, Wong E, Guyatt GH, King D,
monary disease. Am J Respir Crit Care Med
al. Salmeterol plus theophylline combina-
tion therapy in the treatment of COPD. Chest
respiratory rehabilitation in chronic obstruc-
23. Rennard SI, Anderson W, ZuWallack R,
et al. Use of a long-acting inhaled beta2-
37. Pauwels RA, Löfdahl C-G, Laitinen LA,
adrenergic agonist, salmeterol xinafoate, in
50. Griffiths TL, Burr ML, Campbell IA, et al.
patients with chronic obstructive pulmonary
Results at 1 year of outpatient multidisci-
disease. Am J Respir Crit Care Med 2001;163:
obstructive pulmonary disease who continue
plinary pulmonary rehabilitation: a random-
smoking. N Engl J Med 1999;340:1948-53.
ised controlled trial. Lancet 2000;355:362-8. 24. Aalbers R, Ayres J, Backer V, et al. For- 38. Vestbo J, Sorensen T, Lange P, Brix A,
moterol in patients with chronic obstruc-
51. British Thoracic Society Standards of
tive pulmonary disease: a randomized, con-
trolled, 3-month trial. Eur Respir J 2002;19:
bilitation. Pulmonary rehabilitation. Tho-
936-43. [Erratum, Eur Respir J 2002;20:245.]
a randomised controlled trial. Lancet 1999;
25. Casaburi R, Mahler DA, Jones PW, et al. 52. Gray-Donald K, Gibbons L, Shapiro SH,
A long-term evaluation of once-daily inhaled
39. Burge PS, Calverley PM, Jones PW, Spen-
Macklem PT, Martin JG. Nutritional status
and mortality in chronic obstructive pulmo-
nary disease. Eur Respir J 2002;19:217-24.
ised, double blind, placebo controlled study
nary disease. Am J Respir Crit Care Med 1996;
26. Belman MJ, Botnick WC, Shin JW.
of fluticasone propionate in patients with
moderate to severe chronic obstructive pul-
53. Ferreira IM, Brooks D, Lacasse Y, Gold-
hyperinflation during exercise in patients
monary disease: the ISOLDE trial. BMJ 2000;
stein RS, White J. Nutritional supplementa-
with chronic obstructive pulmonary disease.
tion for stable chronic obstructive pulmo-
Am J Respir Crit Care Med 1996;153:967-75. 40. The Lung Health Study Research Group. 27. O’Donnell DE, Lam M, Webb KA. Spiro-
Effect of inhaled triamcinolone on the decline
metric correlates of improvement in exercise
in pulmonary function in chronic obstruc-
54. Long term domiciliary oxygen therapy
performance after anticholinergic therapy
tive pulmonary disease. N Engl J Med 2000;
in chronic obstructive pulmonary disease.
Am J Respir Crit Care Med 1999;160:542-9. 41. Sutherland ER, Martin RJ. Airway inflam- 28. Combivent Inhalation Aerosol Study
disease: comparisons with asthma. J Allergy
55. Nocturnal Oxygen Therapy Trial Group.
disease, a combination of ipratropium and
Continuous or nocturnal oxygen therapy in
albuterol is more effective than either agent
42. Spencer S, Calverley PM, Sherwood
alone: an 85-day multicenter trial. Chest
Burge P, Jones PW. Health status deteriora-
ease: a clinical trial. Ann Intern Med 1980;
tion in patients with chronic obstructive pul-
29. Gross NJ, Petty TL, Friedman M, Sko-
monary disease. Am J Respir Crit Care Med
56. Emtner M, Porszasz J, Burns M, Som-
fay A, Casaburi R. Benefits of supplemental
43. Sutherland ER, Allmers H, Ayas NT,
Downloaded from www.nejm.org by ALEXANDRE A. HOLANDA MD on January 30, 2007 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
emic chronic obstructive pulmonary disease
lung volume in severe stable COPD. Thorax
medical therapy for severe emphysema.
patients. Am J Respir Crit Care Med 2003;
60. Clini E, Sturani C, Rossi A, et al. The Ital- 63. Idem. Patients at high risk of death after 57. Johnson AOC. Chronic obstructive pul-
ian multicentre study on noninvasive venti-
lung-volume–reduction surgery. N Engl J
monary disease · 11: fitness to fly with COPD.
lation in chronic obstructive pulmonary dis-
ease patients. Eur Respir J 2002;20:529-38. 64. Arcasoy SM, Kotloff RM. Lung trans- 58. Meecham Jones DJ, Paul EA, Jones PW,
Wedzicha JA. Nasal pressure support venti-
61. Geddes D, Davies M, Koyama H, et al.
Effect of lung-volume–reduction surgery in
65. Hosenpud JD, Bennett LE, Keck BM,
Edwards EB, Novick RJ. Effect of diagnosis
J Respir Crit Care Med 1995;152:538-44.
on survival benefit of lung transplantation
59. O’Donoghue FJ, Catcheside PG, Jordan 62. National Emphysema Treatment Trial
AS, Bersten AD, McEvoy RD. Effect of CPAP
on intrinsic PEEP, inspiratory effort, and
paring lung-volume-reduction surgery with
Copyright 2004 Massachusetts Medical Society.electronic access to the journal’ s cumulative index
At the Journal’s site on the World Wide Web (www.nejm.org), you can search an index of all articles published since January 1975 (abstracts 1975–1992, full text 1993–present). You can search by author, key word, title, type of article, and date. The results will include the citations for the articles plus links to the full text of articles published since 1993. For nonsubscribers, time-limited access to single articles and 24-hour site access can also be ordered for a fee through the Internet (www.nejm.org).
Downloaded from www.nejm.org by ALEXANDRE A. HOLANDA MD on January 30, 2007 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
GEBRAUCHSINFORMATION: INFORMATION FÜR ANWENDER Imodium 2 mg Kapseln Lesen Sie die gesamte Packungsbeilage sorgfältig durch bevor Sie mit der Einnahme dieses Arzneimittels beginnen, denn sie enthält wichtige Informationen. Nehmen Sie dieses Arzneimittel immer genau wie in dieser Packungsbeilage beschrieben bzw. genau nach Anweisung Ihres Arztes oder Apothekers ein. - Heben Sie
ERSTE HILFE RATGEBER Welche med. Indikationen sind bei welchen Symtomen/Beschwerden/Verletzungen anzuwenden? Beschwerden Medikamente Anwendungsspektrum Dosierung Gegenanzeige/Nebenwirkungen Wundbehandlung nicht bei Überempfindlichkeit gegen Jod, nichtin der SchwangerschaftBetaisodona Wundflies (=LSG) bei infizierten Hautpartien, wenn Wundbehandlungsmittel Bepanthen Salb
 patients at risk to detect asymptomatic airflow lim- drug therapy
patients at risk to detect asymptomatic airflow lim- drug therapy