Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Healthegoods.com
role of vitamin d in cardiovascular disease G. Verhave1*, C.E.H. Siegert2
1VU Medical Centre, Amsterdam, the Netherlands, 2St. Lucas Andreas Hospital, Amsterdam,
the Netherlands, *corresponding author: e-mail:[email protected]a b s t r a C t there is increasing evidence for health benefits accomplished
benefits accomplished by activated vitamin D through
by activated vitamin d through interaction with the vitamin d
interaction with the vitamin D receptor (VDR) that go
receptor (vdr) that go beyond calcium and bone homeostasis
beyond these classical functions. The VDR is expressed
and regulation of parathyroid hormone (Pth) secretion.
by many tissues and is present in, for instance, arteries,
treatment with vitamin d receptor agonists (vdras) is
heart, the immune system and endocrine organs (table 1).1
associated with reduced mortality in (pre)dialysis patients.
As kidney function deteriorates, activated vitamin D levels
interestingly, these relations are independent of Pth
decline.2 Therefore patients with renal dysfunction are
levels and calcium x phosphorus product. this suggests
a suitable population to study the effects of vitamin D
the presence of biological functions of vitamin d that
treatment. Low serum 1,25(OH) D levels cause an increase
are independent of its interaction with the parathyroid
in PTH secretion and the development of secondary
glands. because chronic kidney disease leads to increased
hyperparathyroidism (SHPT). High serum PTH and
cardiovascular mortality, mechanisms in which vdras
hyperphosphataemia are known risk factors for increased
can influence cardiovascular disease are discussed. these
mortality among patients on dialysis. Therefore, recent
mechanisms comprise the potential ameliorating effects
guidelines have formulated new, stricter, target ranges for
of vdras on atherosclerosis, arterial media calcification,
serum calcium, phosphorus and PTH levels.3,4
cardiac hypertrophy, the renin-angiotensin system and
In recent years, it has become clear that there is increased
thrombosis. Moreover, treatment strategies with vdras are
mortality among vitamin D deficient patients on dialysis.5
discussed together with several recent observational studies.
Moreover, treatment with vitamin D receptor activators
treatment advice consists of correction of 25(oh) vitamin
(VDRAs) is associated with reduced mortality in (pre)
d deficiency, low-dose calcitriol in patients with secondary
dialysis patients.6-8 Interestingly, these relations are
hyperparathyroidism, and activated vitamin d analogues may be indicated when higher doses are needed to suppress Pth secretion. new insights into biological and clinical effects of table 1. Tissue distribution of the vitamin D receptor vdras may broaden the patient group that may benefit from vdra treatment to patients with creatinine clearances in the 30 to 60 ml/min range. K e y w o r d s
Vitamin D receptor activation, cardiovascular disease,
i n t r o d u C t i o n
Vitamin D is known for its primary role in calcium and
bone homeostasis and regulation of parathyroid hormone
(PTH) secretion. There is increasing evidence for health
Van Zuiden Communications B.V. All rights reserved.
independent of PTH levels and calcium x phosphorus
with a clinical history of atherosclerosis. Arterial media
product. This suggests the presence of biological functions
calcification was observed mainly in the younger group
of vitamin D that are independent of its interaction
without conventional atherosclerotic risk factors.11 Vitamin
with the parathyroid glands. What these theoretical
D can inhibit various aspects of inflammation leading
mechanisms comprise and what the effects are of VDRA
to intimal and medial calcification. Further on we will
C a r d i o v a s C u l a r d i s e a s e v d r a d i r e C t e d C y t o K i n e s : e f f e C t s o n a t h e r o s C l e r o s i s
Below an estimated glomerular filtration rate (eGFR) of 60 ml/min, chronic kidney disease (CKD) leads to increased
T lymphocytes and macrophages are known stimulators
cardiovascular mortality in nondialysed patients.9 In
of intimal thickening and plaque formation in arteries
patients on dialysis this risk further increases: half of the
susceptible of atherosclerosis. Th1 lymphocytes
mortality rate is caused by cardiovascular events.10
secrete interferon-gamma (IFN-γ), which is a potent
The two most important arterial complications leading
macrophage activator and a Th2 lymphocyte suppressor.
to cardiovascular events are intimal and medial
Th2 lymphocytes, in their turn, are antiatherogenic
calcification. Arterial intima calcification is associated
through production of Il-10, which inhibits macrophage
with atherosclerosis and leads to plaque formation and
activation.17 The development of CD4+ T cells into
rupture with subsequent blood vessel occlusion. Arterial
either Th1 or Th2 cells determines the outcome of
media calcification is associated with proliferation of
an immune response, and is primarily directed by
vascular smooth muscle cells and leads to calcification
cytokines; Th1 cells develop in response to IL-12 and
and stiffening of the vessel wall.11 The magnitude of
IFN-γ, whereas IL-4 induces the development of Th2
coronary artery calcification, assessed by electron beam
cells. VDRA have potential ameliorating effects on the
computed tomography and ultrasound, is correlated with
development of atherosclerosis by several mechanisms.
clinical cardiac events.12 Studies evaluating patients with
Firstly, they have a direct effect on naive CD4+ T cells
stage 3 to 5 CKD (table 2) have demonstrated excessive
by enhancing the development of Th 2 lymphocytes
coronary artery calcification,13 even in young adults,14 and
(through Il-4 production).18 Furthermore treatment
suggest that coronary artery calcification is an independent
with VDRA inhibits the transcription of IFN-γ that is
predictor of death in patients on dialysis.15 Whether this
either required for Th1 development or is a product
excessive calcification is primarily due to intimal or medial
of Th1 cells.18,19 Moreover, human and mouse naive
calcification is subject of debate. There is evidence that in
CD4+ cells differentiated into IL-10 producing T cells,
patients with CKD increased arterial media calcification,
after treatment with VDRAs and dexamethasone.20
more than arterial intima calcification, is responsible
Through these mechanisms VDRAs may change the
for the high cardiovascular mortality rate. This was
Th1/Th2 balance and influence the production of (anti)
demonstrated histologically through staining of inferior
epigastric arteries from patients on dialysis that showed ‘pure’ medial calcification.16 In another study among patients on dialysis ultrasonography of carotid arteries
v a s C u l a r C a l C i f i C a t i o n
showed arterial intima calcification in older patients
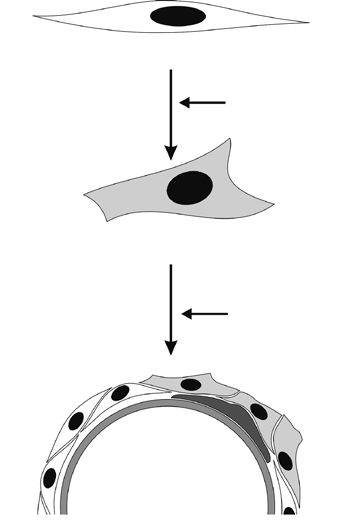
Vascular smooth muscle cells (VSMCs) and osteoblasts derive from a similar mesenchymal precursor cell. Core
table 2. Stages of kidney disease
binding alpha-1 (Cbfa1) is thought to be the switch that
description
turns this mesenchymal cell into an osteoblast. Moe
Normal kidney function but urine findings
and Chen observed expression of Cbfa1 in inferior
or structural abnormalities or genetic trait
epigastric arteries of renal transplant patients while
only minimal expression was found in noncalcified
Mildly reduced kidney function, and other
findings (as for stage 1) point to kidney
arteries.21 Uraemic toxins present in serum from dialysis
patients and the expression of osteogenic markers, such
as bone morphogenetic protein-2 (BMP-2), also lead to
accelerated transformation of VSMCs into osteoblast-like
cells.16 These cells are capable of producing bone matrix
proteins (type1 collagen, osteopontin, bone sialoprotein),
gfr = glomerular filtration rate.
which may subsequently regulate mineralisation.22
Verhave, et al. Vitamin D and cardiovascular disease.
Once mineralisation is initiated, an increased calcium x
r o l e o f v d r a s i n v a s C u l a r
phosphorus product, as occurs in patients with renal
C a l C i f i C a t i o n
insufficiency, may accelerate the process of calcification which leads to stiffening of the vessel.23 In the past
The survival benefit of the use of VDRAs seems
accelerated calcification in patients on dialysis has been
contradictory to the perception that VDRAs, due to their
interpreted to be caused by the presence of potentiators
potential impact of increasing serum phosphorus and
of calcification. An alternative interpretation is that
calcium, may cause vascular calcification.28 Yet there
uraemic serum lacks calcification inhibitors.
is evidence for an inhibitory role of VDRAs in vascular
Recently several inhibitors of vascular calcification
calcification. For a start, VDRs are present in VSMCs and
have been identified. Matrix gla protein (MGP) inhibits
treatment with VDRAs inhibits the synthesis of type 1
vascular calcification in several possible ways. Muscle
collagen.22 More importantly, VDRA treatment reduces
phenotype transition was tested in vivo using MGP
cbfa-1 synthesis,29 stimulates the synthesis of MGP and
-/- mice that spontaneously develop calcification in
inhibits BMP-2 production in cultured osteoblastic cells.30,31
all major arteries. The calcified arteries showed an upregulation of osteopontin and induction of Cbfa1 protein expression.24 Furthermore MGP is an inhibitor
o t h e r M e C h a n i s M s
of BMP-2.25 A number of circulating proteins may inhibit the vascular calcification process, including fetuin-A,26
Decreased vitamin D activity increases renin expression,
PTH-related-peptide and C-natriuretic protein.27
renin levels, atrial natriuretic peptide and angiotensin
These mechanisms demonstrate that vascular calcification
II levels and causes hypertension and cardiac myocyte
is a highly regulated process resulting from an imbalance
hypertrophy in mouse models.32-34 Recently it was found
between the loss of inhibitory factors and the increase
that VDR activation has ameliorating effects on cardiac
of inducing factors present both in vessels and in the
hypertrophy and inhibits several renin-angiotensin system
circulation ( figure 1). Knowledge of the role of VDRAs in
(RAS) components. Intravenous treatment with calcitriol
in patients on haemodialysis has been demonstrated to be strongly associated with regression of myocardial hypertrophy.35 Treatment of nephrectomised rats with paricalcitol was associated with suppression of renin, renin receptor, angiotensinogen and angiotensin II type 1 receptor. Hypertension and the deterioration of
figure 1. Development of vascular calcification
renal function were significantly improved with VDRA treatment.34 Furthermore VDR activation probably has impact on the cardiovascular system by preventing
thrombosis. In vitamin D knockout mice platelet aggregation was enhanced, tissue factor expression was
upregulated and thrombomodulin/antithrombin were downregulated,36 which are all prothrombotic conditions ( figure 2). t r e a t M e n t s t r a t e g i e s Loss of inhibitors:
Recently it has become clear that very low levels of
25(OH) vitamin D (<17.8 ng/ml or 44.5 nmol/l) are associated with increased all-cause mortality in patients with and without kidney disease.37,38 Studies examining replacement of 25(OH) vitamin D in patients without kidney disease support a small but beneficial effect on survival.39 Moreover, treatment with 25(OH) vitamin D results in significant reduction in PTH levels in patients
with 25(OH) vitamin D levels <75 nmol/l, irrespective of their kidney function.40,41Therefore patients with
Cbfa-1 = core binding alpha-1; bMP-2 = bone morphogenetic protein-2;
25(OH) vitamin D levels below 75 nmol/l should receive
MgP = Matrix gla protein.
replacement therapy with native vitamin D/ergocalciferol.
Verhave, et al. Vitamin D and cardiovascular disease. figure 2. Inhibitors of cardiac hypertrophy and vascular damage through vitamin D receptor activation
Usually this treatment is not sufficient to achieve
slower progression of kidney disease and lower mortality
suppression of SHPT in advanced chronic kidney disease
risk.8 For reasons of convenience, in haemodialysis patients
and VDRAs are needed. VDRA therapy in patients
active vitamin D is often administered parenterally after
with CKD has been associated with improved survival.
dialysis. Oral treatment with calcitriol is presumably
Intravenous calcitriol or paracalcitriol treatment of patients
equally effective in reducing SHPT and mortality risk and
on haemodialysis offered a significant survival advantage
of 20 to 25% over patients who did not receive parental
Clinical guidelines suggest stringent control of PTH,
vitamin D.6 This has prompted some other observational
calcium and phosphate in an attempt to lower the risk
studies examining outcomes associated with the use of
of vascular calcification and bone disease.3 Very recently
VDRAs by patients on dialysis and predialysis patients.7,8
KDIGO (Kidney Disease: Improving Global Outcome)
These studies consistently showed that patients treated
guidelines stated that in patients with CKD stage 3 to 5
with any kind of VDRA experienced significantly lower
not on dialysis, in whom serum PTH is rising above the
all-cause and cardiovascular mortality rates compared with
upper limit of normal, despite modifiable factors, VDRAs
patients not receiving any treatment. Subgroup analyses
are warranted.4 Implicit in these recommendations is
indicated that virtually all patients benefited from VDRA
the avoidance of the native VDR activator calcitriol if
therapy, including patients with lower PTH or higher
the calcium and phosphate levels exceed their upper
calcium or phosphorus levels. These findings emphasise
limits. This has advocated the use of several VDRAs that
a physiological effect of VDRAs that is PTH independent.
can suppress PTH production with less induction of
Despite these convincing data we have to be cautious in
concomitant hypercalcaemic and hyperphosphataemic
using observational data as a final proof of a beneficial
effects.45 One could question the importance of this
effect and randomised trials are warranted.
favourable side-effect profile since the benefit of calcitriol extends to patient groups with high calcium and phosphorus levels. On the other hand long-term positive
w h i C h v d r a , d o e s i t M a t t e r ?
calcium balance may contribute to vascular calcification. Moreover, observational data suggest a decreased rate
Several studies using oral calcitriol in predialysis and
of progression of established vascular calcification with
dialysis patients have shown a reduced overall mortality
non-calcium containing phosphate binders.46
risk ranging from -26 to -45%.8,42,43 The advantage
Examples of activated vitamin D analogues with
included patients with the highest levels of serum
this favourable side-effect profile are doxercalciferol,
calcium, phosphorus and PTH. In predialysis patients
paricalcitol, and alfacalcidol. Animal models show
high pharmacological doses of calcitriol may hasten loss
a potential advantage for paricalcitol; it induces less
of kidney function,44 but this effect is not seen with lower
vascular calcification compared with calcitriol.47 Earlier we
doses of calcitriol. On the contrary: low-dose calcitriol
mentioned the historical cohort study by Teng et al., where
(<0.25 µg/day) has been associated with a trend towards
67,339 patients on haemodialysis were examined. In this
Verhave, et al. Vitamin D and cardiovascular disease.
study paricalcitol was associated with a 16% lower all-cause
9. Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney
disease as cause of death, cardiovascular events and hospitalization.
mortality compared with treatment with calcitriol.6 In
another study these findings were not confirmed. Tentori
10. Sarnak MJ, Coronado BE, Greene T, et al. Cardiovascular disease risk
et al. compared outcomes in patients receiving calcitriol,
factors in chronic renal insufficiency. Clin Nephrol. 2002;57:327-35.
paricalcitol and doxercalciferol and found lower mortality
11. London GM, Guerin AP, Marchais SJ, Métivier F, Pannier B, Adda H.
in patients on paricalcitol and doxercalciferol in unadjusted
Arterial media calcification in end-stage renal disease: impact on all cause and cardiovascular mortality. Nephrol Dial Transplant. 2003;18:1731-40.
models. But in adjusted models this difference was
12. Wong ND, Hsu JC, Detrano RC, Diamond G, Eisenberg H, Gardin
not statistically significant.7 Obviously, more studies
JM. Coronary artery calcium evaluation by electron beam computed
are needed to prove the benefit of activated vitamin D
tomography and its relation to new cardiovascular events. Am J Cardiol. 2000;86:495-8.
13. Kramer H, Toto R, Peshock R, Cooper R, Victor R. Association between
chronic kidney disease and coronary artery calcification: the Dallas Heart Study. J Am Soc Nephrol. 2005;16:507-13. t r e a t M e n t a d v i C e
14. Goodman WG, Goldin J, Kuizon BD, et al. Coronary artery calcification in
young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med. 2000;342:1478-83.
Treatment of SHPT is the generally accepted and approved
15. Matsuoka M, Iseki K, Tamashiro M, et al. Impact of high coronary artery
indication for treatment with vitamin D. It seems
calcification score (CACS) on survival in patients on chronic hemodialysis.
reasonable to correct 25(OH) vitamin D deficiency as a first
step in the treatment of SHPT. New insights into biological
16. Moe SM, Duan D, Doehle BP, O’Neill KD, Chen NX. Uremia induces the
and clinical effects of VDR activation may broaden the
osteoblast differentiation factor Cbfa1 in human blood vessels. Kidney Int. 2003;63:1003-11.
patient group that may benefit from VDRA treatment to
17. Li AC, Glass CK. The macrophage foam cell as a target for therapeutic
patients with creatinine clearances in the 30 to 60 ml/min
intervention. Nat Med. 2002;8:1235-42.
range. Low-dose calcitriol is indicated for patients with
18. Boonstra A, Barrat FJ, Crain C, et al. 1,25-dihydroxyvitamin D3 has a direct
early SHPT. A switch to activated vitamin D analogues
effect on naïve CD4+ T cells to enhance the development of Th2 cells. J Immunol. 2001;167:4974-80.
is indicated when higher doses are needed to suppress PTH secretion and treatment goals concerning calcium x
19. Staeva-Vieira TP, Freedman LP. 1,25-dihydroxyvitamin D inhibits
IFN-gamma and IL-4 levels during in vitro polarization of primary murine
CD4+ T cells. J Immunol. 2002;168:1181-9.
20. Barrat FJ, Cua DJ, Boonstra A, et al. In vitro generation of interleukin
10-producing regulatory CD4+ T cells to enhance the development of TH2-inducing cytokines. J Exp Med. 2002;195:603-16. a C K n o w l e d g e M e n t s
21. Moe SM, Chen NX. Pathophysiology of vascular calcification in chronic
kidney disease. Circ Res. 2004;95:560-7.
We would like to thank Dr. Lukas C. Kapitein for the
22. Bellows CG, Reimers SM, Heersche JNM. Expression of mRNAs for type-1
collagen, bone sialoprotein, osteocalcin, and osteopontin at different stages of osteoblastic differentiation and their regulation by 1,25 dihydroxy vitamin D3. Cell Tissue Res. 1999;297:249-59.
23. Reynolds JL, Joannides AJ, Skepper JN, et al. Human vascular smooth
r e f e r e n C e s
muscle cells undergo vesicle mediated calcification in response to changes in extracellular calcium and phosphate concentrations: a potential mechanism for accelerated vascular calcification in ESRD. J Am
1. Holick MF. Vitamin D: importance in prevention of cancers, type 1
diabetes, heart disease and osteoporosis. Am J Clin Nutr. 2004;79:362-71.
24. Steitz SA, Speer MY, Curinga G, et al. Smooth muscle cell phenotype
2. Levin A, Bakris GL, Molitch M, et al. Prevalence of abnormal serum
transition associated with calcification: upregulation of Cbfa1
vitamin D, PRH, calcium, and phosphorus in patients with chronic kidney
and downregulation of smooth muscle lineage markers. Circ Res.
disease: Results of the study to evaluate early kidney disease. Kidney Int.
25. Speer MY, McKee MD, Guldberg RE, et al. Inactivation of the osteopontin
3. K/DOQI clinical practice guidelines for bone metabolism and disease in
gene enhances vascular calcification of matrix gla protein-deficient mice:
chronic kidney disease. Am J Kidney Dis. 2003;42:S1-202.
evidence for osteopontin as an inducible inhibitor of vascular calcification in vivo. J Exp Med. 2002;196:1047-55.
4. KDIGO Clinical practice Guideline for the Diagnosis, Evaluation,
Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone
26. Ketteler M, Bongartz P, Westenfeld R, et al. Association of low fetuin-A
Disorder (CKD-MBD) Kidney Int. 2009;76:suppl 113.
(AHSG) concentrations in serum with cardiovascular mortality in patients on dialysis: a cross-sectional study. Lancet. 2003;361:827-33.
5. Wolf M, Shah A, Gutierrez O, et al. Vitamin D levels and early mortality
among incident hemodialysis patients. Kidney Int. 2007;72:1004-13.
27. Huang Z, Li J, Jiang Z, Qi Y, Tang C, Du J. Effects of adrenomodulin,
C-type natriuretic peptide, and parathyroid hormone-related peptide on
6. Teng M, Wolf M, Lowrie E, Ofsthun N, Lazarus JM, Thadhani R. Survival
calcification in cultured rat vascular smooth muscle cells. J Cardiovasc
of patients undergoing hemodialysis with paricalcitol or calcitriol therapy.
28. Jono S, Nishizawa Y, Shioi A, Morii H. 1,25 dihyroxyvitamin D3 in vitro
7. Tentori F Hunt WC, Stidley CA, et al. Mortality risk among
vascular calcification by modulating secretion of endogenous parathyroid
hemodialysis patients receiving different vitamin D analogs. Kidney Int.
hormone-related peptide. Circulation. 1998;98:1302-6.
29. Drissi H, Pouliot A, Koolloos C, et al. 1,25-(OH)2-vitamin D3
8. Kovesdy CP, Ahmadzadeh S, Anderson JE, Kalantar-Zadeh K. Association
suppresses the bone-related Runx2/Cbfa1 gene promoter. Exp Cell Res.
of activated vitamin D treatment and mortality in chronic kidney disease.
Verhave, et al. Vitamin D and cardiovascular disease.
30. Fraser JD, Otawara Y, Price PA. 1,25-dihhydroxy D3 stimulates the
39. Autier P, Gandini S. Vitamin D supplementation and total mortality:
synthesis of gamma-carboxyglutamic acid protein by osteosarcoma cells.
a meta-analysis of randomized controlled trials. Arch Intern Med.
Mutually exclusive expression of vitamin K-dependent bone proteins in
clonal osteoblastic cell lines. J Biol Chem. 1988;263:911-6.
40. Kooienga L, Fried L, Scragg R, Kendrick J, Smits G, Chonchol M.
31. Virdi AS, Cook LJ, Oreffo RO, Triffit JT. Modulation of bone
The effect of combined calcium and vitamin D3 supplementation on
morphogenetic protein-2 and bone morphogenetic protein-4 gene
serum intact parathyroid hormone in moderate CKD. Am J Kidney Dis.
expression in osteoblastic cell lines. Cell Mol Biol. 1998;44:1237-46.
32. Li YC, Kong J, Wei M, Chen ZF, Liu SQ, Cao LP. 1,25 dihydroxyvitamin
41. Zisman AL, Hristova M, Ho LT, Spraque SM. Impact of ergocalciferol
D(3) is a negative endocrine regulator of the renin-angiotensin system.
treatment of vitamin D deficiency on serum parathyroid hormone
concentrations in chronic kidney disease. Am J Nephrol. 2007;27:36-43
33. Xiang W, Kong J, Chen S, et al. Cardiac hypertrophy in vitamin D receptor
42. Shoben AB, Rudser KD, de Boer IH, Young B, Kestenbaum B. Association
knockout mice: role of the systemic and cardiac renin-angiotensin
of oral calcitriol with improved survival in nondialyzed CKD. J Am Soc
systems. Am J Physiol Endocrinol Metab. 2005;288:125-32.
34. FreundlichM, Quiroz Y, Zhang Z, et al. Suppression of renin-angiotensin
43. Naves-Diaz M, Alvarez-Hernandez D, Passlick-Deetjen K, et al. Oral active
gene expression in the kidney by paricalcitol. Kidney Int. 2008;74:1394-1402.
vitamin D is associated with improved survival in hemodialysis patients. Kidney Int. 2008;74:1070-8.
35. Kim HW, Park CW, Shin YS, et al. Calcitriol regresses cardiac hypertrophy
and QT dispersion in secondary hyperparathyroidism on hemodialysis.
44. Schwarz S, Trivedi BK, Kalantar-Zadeh K, Kovesdy CP. Association of
disorders in mineral metabolism with progression of chronic kidney disease. Clin J Am Soc Nephrol. 2006;1:825-31.
36. Aihara K, Azuma H, Akaike M, et al. Disruption of nuclear vitamin D
receptor gene causes enhanced thrombogenicity in mice. J Biol Chem.
45. Coyne DW, Grieff M, Ahya SN, Giles K, Norwood K, Slatopolsky E.
Differential effects of acute administration of 19-nor-1,25-dihydroxy-vitamin D2 and 1,25-dihydroxy-vitamin D3 on serum calcium and
37. Melamed ML, Michos ED, Post W, Astor B. 25-hydroxyvitamin D levels
phosphorus in hemodialysis patients. Am J Kidney Dis. 2002;40:1283-8.
and the risk of mortality in the general population. Arch Int Med. 2008;168:1629-37.
46. Moe SM, Chertow GM. The case against calcium-based phosphate
binders. Clin J Am Soc Nephrol. 2006;1:697-703.
38. Ravani P, Malberti F, Tripepi G, et al. Vitamin D levels and patient
outcome in chronic kidney disease. Kidney Int. 2009;75:88-95.
47. Mizobuchi M, Finch JL, Martin DR, Slatopolsky E. Differential effects
of vitamin D receptor activators on vascular calcification in uremic rats. Kidney Int. 2007;72:709-15.
Verhave, et al. Vitamin D and cardiovascular disease.
QUE DOIS-JE SURVEILLER PENDANT MON TRAITEMENT ? FICHE D’INFORMATION* LE POIDS : Certains neuroleptiques peuvent entraîner une prise de poids. Certains patients grossissent, d’autres pas. HALDOL ® (Halopéridol) Pour éviter une surcharge pondérale, il convient dès le début du traitement, desurveiller régulièrement son poids, d’éviter les sucreries, de pratiquer une ou
It has been estimated that 100,000 tonnes of extraterrestrial material Every year the Earth is showered by reach the Earth’s surface every year. It extraterrestrial material falling from can be anything from fine dust to space. The Museum’s mineralogy and metallic masses weighing many tonnes. petrology collections include a small Extraterrestrial material t
 Once mineralisation is initiated, an increased calcium x
r o l e o f v d r a s i n v a s C u l a r
Once mineralisation is initiated, an increased calcium x
r o l e o f v d r a s i n v a s C u l a r