Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Zolpidem and driving impairment
Barry K. Logan,1,2 Ph.D. and Fiona J. Couper,2 Ph.D.REFERENCE: Logan BK, Couper FJ. Zolpidem and driving im-
(10 ng/mL), propoxyphene (100 ng/mL), barbiturates (100 ng/mL),
pairment. J Forensic Sci 2001;46(1):105–110.
benzodiazepines (50 ng/mL), and tricyclic antidepressants (100ng/mL). The GC/MS methods are described elsewhere (2,3). ABSTRACT: Zolpidem, a non-benzodiazepine hypnotic, was
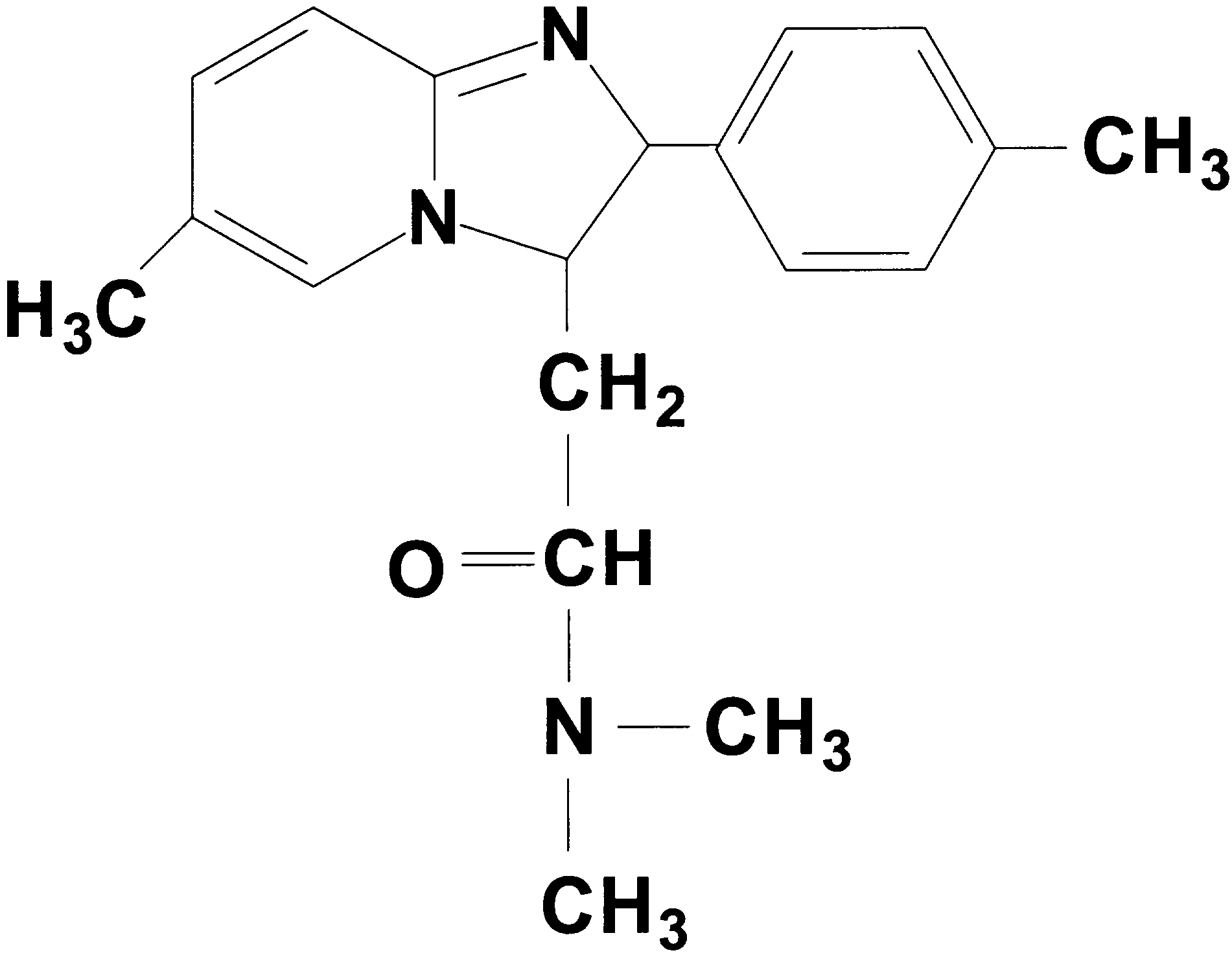
Zolpidem (Fig. 1) is isolated in the basic fraction of the drug screen,
identified in the blood of 29 subjects arrested for impaired driving.
and appears in the chromatogram in the same region as quinine and
Zolpidem concentrations ranged from 0.05 to 1.4 mg/L (mean 0.29mg/L, median 0.19 mg/L). In the subjects whose cases we reviewed
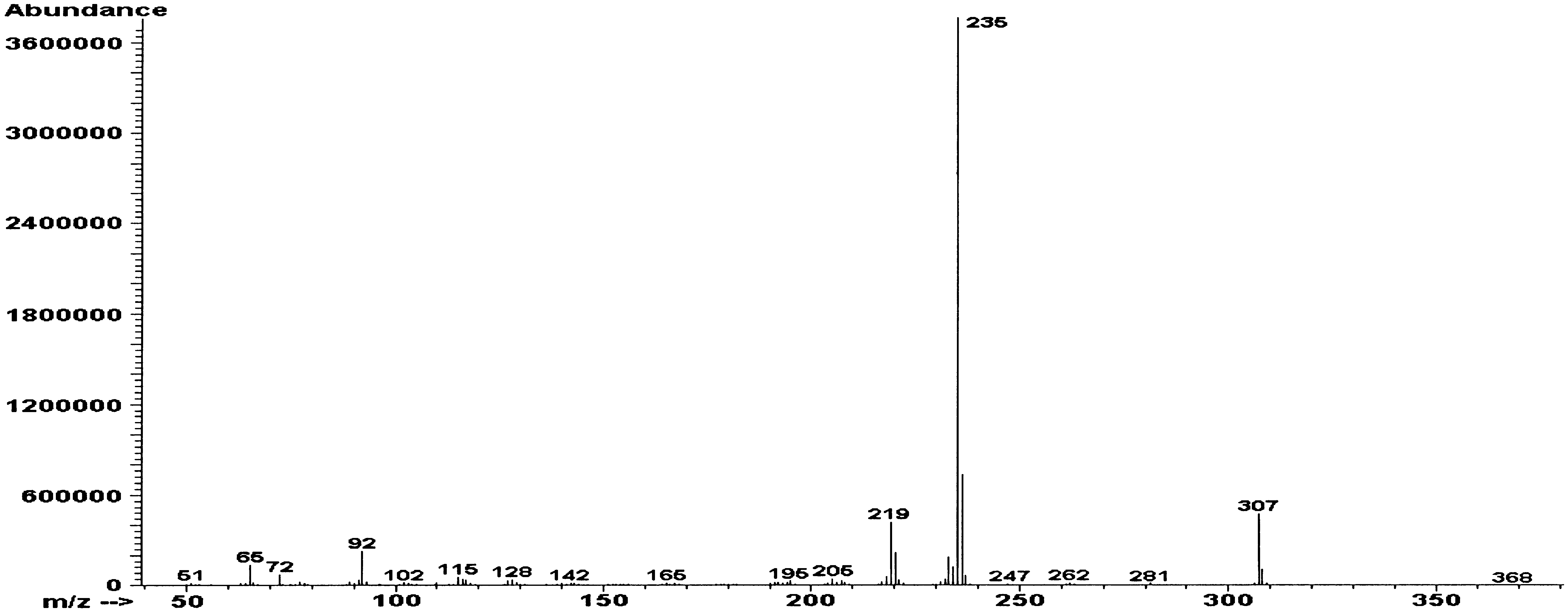
alprazolam. It has the mass spectrum shown in Fig. 2. When iden-
where zolpidem was present with other drugs and/or alcohol, symp-
tified in a subject’s blood, zolpidem was quantitated using a five-
toms reported were generally those of CNS depression. Symptoms
point calibration curve (0.00, 0.10, 0.25, 0.50, 1.00 mg/L). Cali-
included slow movements and reactions, slow and slurred speech,
bration was determined to be linear over the range 0.05 to 2.00
poor coordination, lack of balance, flaccid muscle tone, and hori-zontal and vertical gaze nystagmus. In five separate cases, where
mg/L, and the correlation coefficient was typically better than
zolpidem was the only drug detected (0.08–1.40 mg/L, mean 0.65
0.990. The limit of quantitation (LOQ) was defined as 0.05 mg/L,
mg/L, median 0.47 mg/L), signs of impairment included slow and
the lowest concentration at which the assay was determined to be
slurred speech, slow reflexes, disorientation, lack of balance and co-
linear. Any peaks with the correct retention time, quantitating at
ordination, and “blacking out.” Although no quantitative relation-
less than 0.05 mg/L, but for which a mass spectrum of zolpidem
ship between blood concentrations and degree of driving impair-ment is currently possible, it is reasonable to conclude that because
was obtained, were reported as Ͻ0.05 mg/L.
of its specific activity as a sleep inducer, blood concentrations con-
In cases where the drug was identified, the circumstances of the
sistent with therapeutic doses of zolpidem have the potential to af-
incident, including alcohol or other drugs detected, driving behav-
fect driving in a negative way, and that concentrations above the
ior, subjects’ appearance, statements, performance in field sobriety
normal therapeutic range would further impair a person’s level ofconsciousness and driving ability.
tests, etc., were tabulated from the arrest report and are included inTable 1. KEYWORDS: forensic science, zolpidem, driving, impairment Results and Discussion
Other workers have previously reported that subjects taking the
In total, 29 cases of suspected impaired driving in which zolpi-
popular sleep inducer zolpidem (Ambien®) have been arrested for
dem was identified were encountered between January 1997 and
impaired driving (1), and in our own jurisdiction, we have encoun-
December 1999. Concentrations ranged from Ͻ0.05 (LOQ) to 1.4
tered a number of cases with similar fact patterns. This prompted
mg/L (mean 0–29 mg/L, median 0–19 mg/L). Zolpidem was usu-
us to review the literature on the pharmacology and performance
ally present with other drugs including alcohol (9 cases), antide-
effects of this drug, and to document the circumstances, indicia of
pressants (10 cases), narcotic analgesics (7 cases), muscle relaxants
impairment, patterns of combined drug use, and driving behavior
(5 cases), benzodiazepines (3 cases), and valproic acid (2 cases). In
in these cases in order to assist with the evaluation of future cases.
five cases, however, zolpidem was the only drug detected. In thesecases the concentration range was 0.08 to 1.40 mg/L (mean 0.65
Structurally, zolpidem is an imidazopyridine (Fig. 1), and unre-
Cases of suspected drug-impaired driving are referred to the
lated to the benzodiazepines. It acts as a non-benzodiazepine ago-
Washington State Toxicology Laboratory by law enforcement
agencies for drug and alcohol testing. Cases where the alcohol con-
A1 function, resulting in sedative/hypnotic effects,
without significant anxiolysis, anticonvulsant, or muscle relaxation
centration cannot reasonably account for the degree of impairment
properties. It is prescribed for the short-term treatment of insomnia
observed in the subject are tested by EMIT and gas chromatogra-
and other sleep disorders. The drug is normally prescribed in 5 to
phy/mass spectrometry (GC/MS) for drugs with weakly acidic and
20 mg doses, to be taken before going to bed. Its rapid absorption
basic character. The enzyme multiplied immunoassay technique
after oral ingestion (peak concentrations are achieved in 1 to 2 h),
(EMIT) procedure screened for cocaine metabolites (cutoff limit
and short half-life (~1 to 2 h) make it very effective as a sleep in-
100 ng/mL), opiates (10 ng/mL), amphetamines (100 ng/mL),
ducer, promoting a short-lasting sleep with rapid onset, and limited
cannabinoids (10 ng/mL), methadone (100 ng/mL), phencyclidine
Following administration of a single 15 mg oral dose of zolpi-
1 State toxicologist, Bureau of Forensic Laboratory Services, Washington
dem, Mattila et al. (4) reported blood zolpidem concentrations of
State Patrol, 2203 Airport Way S., Seattle, WA.
Ϯ 0.045 mg/L at 1.5 h, declining to 0.065 Ϯ 0.013mg/L by
Washington State Toxicology Laboratory, University of Washington, 2203
5.5 h. Following 10 and 20 mg doses, peak plasma concentrations
Received 5 Jan. 2000; and in revised from 7 March 2000; accepted 7 March
(Cmax) of 0.125 Ϯ 0.015 mg/L and 0.232 Ϯ 0.017 mg/L, respec-
tively, have been reported by Greenblatt et al. (5). Time-to-peak
and half-lives for both the 10 and 20 mg doses were 1.7 and 2 to 2.2
drugs subject to first-pass metabolism by P450 3A4 (11), and this
h, respectively, and both doses effectively induced sleep. The phar-
may increase bioavailability of zolpidem.
macokinetics appeared unchanged following 15 consecutive nights
Although less than 1% of a dose of zolpidem is reportedly ex-
of administration of 20 mg (6). A review of other studies shows that
creted unchanged in the urine, Levine et al. (12) reported measur-
Cmax normally achieved in subjects following a 20 mg oral dose
able zolpidem concentrations in urine of deceased subjects both in
have been reported as between 0.192 and 0.324 mg/L at 0.75 to 2.6
overdose and during therapeutic use. In the cases we reviewed,
h post-dose, and dose proportionality with respect to AUC and
urine was tested in only one case and found to be qualitatively pos-
Cmax have been reported over the dosage range of 2.5 to 40 mg (7).
Concentrations of 0.05 mg/L or greater (the LOQ for this study)
In the subjects whose cases we reviewed where zolpidem was
would likely represent levels present in the blood no more than 6 to
present with other drugs, symptoms reported were generally those
8 h after ingestion of a normal therapeutic dose, and would be on
of CNS depression. Nine of these subjects were evaluated by drug
the low end of concentrations associated with a therapeutic effect.
recognition (DRE) officers, who expressed the opinion that the
No differences in pharmacokinetics have been noted between eth-
subject was under the influence of a CNS depressant. Of these nine
nic groups or gender (7,8). Bianchetti et al. (9) have reported that
cases, five involved erratic driving causing near collisions while
time-to-peak blood concentrations appear unaffected by the pres-
the other four involved vehicle collisions. Signs of impairment in-
cluded horizontal gaze nystagmus (HGN) (7 cases), vertical gaze
Zolpidem is metabolized oxidatively to a series of inactive hy-
nystagmus (5 cases), lack of balance and unsteady gait (8 cases),
droxylated metabolites (10). Metabolism appears to be directed
poor or slow coordination (7 cases), poor performance of standard-
through CYP450 3A4, 1A2, and 2D6. This raises the possibility of
ized field sobriety tests (8 cases), slow and/or slurred speech (5
longer half-lives and greater AUC for zolpidem in patients taking
cases), muscle flaccidity (4 cases), and impaired or double vision
medications with significant inhibitory effects on these P450
(3 cases). One driver refused to perform the standardized field so-
isozymes. These include the SSRI drugs fluoxetine, paroxetine,
briety tests. The drivers usually had the general appearance of
venlafaxine, and sertraline, which are substrates for, and inhibitors
drowsiness, tiredness, confusion, and disorientation. However,
of, P450 2D6. Of potential significance is the observation that
symptoms associated with individual drugs cannot readily be re-
grapefruit juice ingestion appears to increase bioavailability of
solved in poly-drug cases. Harvengt et al. (13) have reported someincrease of impairment in alertness when zolpidem is given withother drugs with CNS depressant properties, including chlorpro-mazine, imipramine, and haloperidol.
In five cases zolpidem was the only drug detected. Concentra-
tions ranged from 0.08 to 1.40 mg/L, with a mean of 0.65 mg/L,and a median of 0.47 mg/L. (Note, however, that because of theshort half-life, any delay between the driving and the collection ofthe blood will result in a drop in the concentration.) Signs of im-pairment included slow and slurred speech, slow reflexes, disori-entation and confusion, lack of balance and coordination, loss ofshort-term memory, and “blacking out.” Horizontal gaze nystag-mus was present in every case in which it was evaluated. The fol-lowing histories are from these five DUI cases. All subjects under-went blood alcohol analysis, an EMIT screen for drugs of abuse
and several prescription drug classes, and a GC/MS screen for acid,
FIG. 2—Electron impact mass spectrum of zolpidem.
LOGAN AND COUPER • ZOLPIDEM AND DRIVING IMPAIRMENT
unsteady gait, HGN, VGN, impaired vision, slurred speech,
of alcohol and drugs, slurred speech, slow movements,
slow speech, muscle flaccidity, poor SFSTs, appeared tired
lack of convergence, slow and slurred speech, muscle flaccidity,
lack of balance, unsteady gait, HGN, VGN, slow speech,
unsteady gait, HGN, VGN, lack of convergence, double
VGN, lack of convergence, repetitive speech, muscle flaccidity,
Collision-causing driver—poor coordination, lack of balance,
Erratic driving, lack of balance, appeared under the influence
Near collision—slow and unsteady coordination, lack of balance,
Drove over curb, struck parked vehicle, appeared
Erratic driving—poor coordination, HGN, double vision,
Single-vehicle accident—lack of balance, slurred speech
Collision-causing driver—erratic driving, poor coordination,
Erratic driving—violent and combative, appeared
Collision-causing driver—poor coordination, lack of balance,
Collision-causing driver—unsteady gait, hand tremors, HGN,
Involved in accident–appeared disorientated and confused
Circumstances and driving behavior in 29 drivers testing positive for zolpidem.
admitted taking a sleeping pill about an hour before
required assistance to walk, HGN, VGN, muscle flaccidity,
poor SFSTs, appeared disorientated and confused
Minor multi-car collision—causing driver was staggering around,
Erratic driving—collision-causing driver, lack of balance, HGN,
Erratic driving, near collision–poor coordination, lack of balance,
Single-vehicle accident—officer observed signs of impairment
Collision-causing driver—HGN, poor SFSTs
Erratic driving—lack of balance, slow reflexes, slow and slurred
Collision-causing driver—unable to stand or walk, appeared dazed
Erratic driving—hit parked car and red stop light, slurred speech,
Erratic driving—HGN, VGN, poor SFSTs, slurred speech, lack
Single-vehicle accident—drove through red light, blacked out,
Cases which underwent drug recognition evaluation expert (DRE)/Standard field sobriety tests (SFSTs) (19). *
HGN–Horizontal gaze nystagmus; VGN–Vertical gaze nystagmus.
LOGAN AND COUPER • ZOLPIDEM AND DRIVING IMPAIRMENT
neutral and basic compounds as indicated above. In each case, all
In each case, in the absence of any other reasonable explanation
tests were negative for alcohol or for drugs other than zolpidem.
for the impairment, it was attributed to the ingestion of zolpidem. There was no apparent correlation between the stated time of zolpi-
Case 1—A 17-year-old male was stopped by police for erratic
dem ingestion and the corresponding blood concentration. Two
lane travel. The subject’s speech was slow and slurred, his pupils
separate subjects stated they had taken a single Ambien® tablet ap-
were dilated, and he was experiencing double vision, lack of bal-
proximately 12 h prior to being arrested. The corresponding zolpi-
ance, and lack of coordination. The subject also performed several
dem concentrations were 0.33 mg/L and Ͻ0.05 mg/L. In another
field sobriety tests poorly (such as “finger dexterity” and “walk and
subject, zolpidem was taken within 1 to 2 h prior to the arrest, and
turn” tests). The subject admitted to taking two white pills half an
the zolpidem blood concentration was 0.31 mg/L. In a similar case,
hour prior to the DUI stop, but did not know what pills they were.
a subject ingested two Ambien® tablets 30 min prior to the arrest,
Several hours after the arrest, the subject was suffering from am-
with the corresponding zolpidem blood concentration being 0.43
nesia. Blood was drawn an hour and a half after driving, and the
mg/L. Four or five 10 mg Ambien® tablets were allegedly ingested
zolpidem concentration was 0.08 mg/L.
by another subject whose blood zolpidem concentration after fivehours was Ͻ0.05 mg/L. Roger et al. (14) have reported a poor cor-
Case 2—A 59-year-old male was the causing driver in a two-car
relation (r2 ϭ 0.21) between dose and blood concentration of zolpi-
collision, having hit another vehicle at an intersection. The subject
dem at ten hours post administration.
was unable to walk or stand without assistance and appeared dazed,
During the same period a single case of a fatally injured driver
lethargic, and disorientated. He had poor attention and was unable
testing positive for zolpidem was identified. This was a 49-year-
to perform any standardized field sobriety tests since he was unable
old male who had multiple sclerosis and a seizure disorder. He
to stand without support. He could not follow a stimulus for a test
was the causing driver in a three-car accident, going through a red
of nystagmus; however, his eyes showed a lack of smooth pursuit.
light, and striking two other vehicles. He had been observed driv-
The subject had taken two Ambien® tablets 30 min before the col-
ing in an erratic manner prior to the accident. This individual had
lision. Blood was drawn about an hour after driving, and the zolpi-
a blood drug concentration identified as follows: zolpidem 0.38
mg/L, carbamazepine 4.13 mg/L, hydroxyzine 0.36 mg/L, andpentazocine 0.18 mg/L. The other drug concentrations are in the
Case 3—A 37-year-old female was stopped by police for erratic
normal therapeutic range, while the zolpidem concentration is
driving. The subject had hit a parked car, garbage cans, and a stop
sufficient to result in sedation and sleepiness, and consistent with
sign, and then continued driving. The subject’s speech was slow
concentrations in drivers showing significant impairment (see
and slurred, her actions were very slow and she was unaware of
what had just happened. The subject was extremely disorientated
Other instances of drivers apparently impaired by zolpidem have
and had a marked upper body sway and lack of balance. She ap-
been reported. Meeker (1) reported six cases of subjects driving un-
peared very tired and fell asleep during the evaluation, and was suf-
der the influence of zolpidem, four of whom were involved in au-
fering from amnesia. The interval between blood draw and driving
tomobile accidents, three of which were single-vehicle crashes.
was not known, but the blood zolpidem concentration was 0.47
Blood zolpidem concentrations in these cases ranged from 0.10 to
0.73 mg/L (mean 0.31 mg/L, median 0.17 mg/L), and symptomsincluded slow slurred speech, unsteady gait, confusion, and disori-
Case 4—A 52-year-old female was stopped by police on the
entation. This is consistent with observations in our subjects, in-
freeway after drifting into the northbound lanes while driving
cluding the overlap of the blood concentrations with the therapeu-
south, where she then continued to drive. The subject was slow to
respond to police, and was disoriented, confused, and dazed once
For many drugs, there is justifiably some reluctance in equating
stopped. Her speech was slurred and shaky. She was dressed only
blood concentrations with a specific degree of impairment. We be-
in her underwear and a shirt, and told the officer she was returning
lieve in the case of zolpidem, however, that this issue is clearer than
from the store. Several standardized field sobriety tests were per-
for many other drugs, since the specific function of zolpidem is to
formed and the subject showed all six clues of horizontal nystag-
induce sleep. For many other drugs the sedative effects are merely
mus, and displayed vertical nystagmus also. She had extremely
an inconvenient and often infrequent side effect. Therefore, for the
poor balance on the “one leg stand” and “walk and turn” tests, and
purposes of determining whether the drug would affect a person,
could not touch the tip of her nose. When asked to estimate 30 sec-
we advocate collection and analysis of a blood sample, as opposed
onds she stopped at 14. The subject could not remember her ad-
to a urine sample. Because of its short half-life (~2 h), a morning
dress and other details about herself, or her current circumstances.
urinary void would almost certainly test positive for zolpidem,
Blood was drawn an hour and forty-five minutes after driving, and
even though the blood concentrations have fallen below effective
the zolpidem concentration was 0.88 mg/L.
levels. This short half-life also means that any delay between thetime of driving and the blood draw could result in an appreciable
Case 5—A 44-year-old female was involved in a single-vehicle
drop in the blood zolpidem concentration, which should be taken
traffic accident. The subject had driven through a red traffic light,
into consideration in interpretation.
blacked out, and then driven down an embankment; however, she
Rush (15) has reviewed the performance impairing effects of
had no recollection of the event. The subject admitted being pre-
zolpidem and notes that the general consensus of these studies
scribed Ambien® and Remeron® (temazepam) for depression. The
was that zolpidem did cause significant psychomotor impairment,
subject was alert but stated she must have blacked out. The officer
equivalent to clinically effective doses of the sedative hypnotics
did not detect any apparent signs of impairment; however, the sub-
triazolam, temazepam, or midazolam. Specifically, the studies re-
ject was in considerable pain and could not perform any field so-
viewed found impairment in standard psychological tests such as
briety tests. Blood was drawn an hour and twenty-five minutes af-
picture recall, digit entry and recall, digit symbol substitution
ter driving, and the zolpidem concentration was 1.40 mg/L.
tasks, circular lights task, balance, time estimation, trails making,
and a variety of other tests of cognitive and psychomotor func-
6. Albin H, Vincon G, Vincon J, Hermann P, Thiercelin JF. Study of the
tion. Tolerance to the sleep latency effects of the drug has been
pharmacokinetics of zolpidem in healthy volunteers after repeated ad-
documented, making it most effective for treatment periods of
ministration: effect on antipyrene clearance. In: Sauvanet JP, Langer SZ,Morselli PL, editors. Imidazopyridines in sleep disorders: a novel exper-
less than 28 days. Tolerance to the psychomotor impairing effect
imental and therapeutic approach. New York: Raven Press, 1988;
Information from the manufacturer (16) indicates that the drug
7. Salvá P, Costa J. Clinical pharmacokinetics and pharmacodynamics of
should not be taken before driving, and in fact, that performance
zolpidem. Therapeutic implications. Clin Pharmacokinet 1995;29(3):142–53.
decrements might persist into the next day following use of the
8. Vandel S, Vandel B, Joanne C, Trocherie S, Bechtel P, Larribaud J. In-
drug. Only 1.1% of patients in pre-clinical trials reported daytime
fluence of ethnic origin on the clinical pharmacology of zolpidem. In:
drowsiness, however, and given the short half-life of the drug when
Sauvanet JP, Langer SZ, Morselli PL, editors. Imidazopyridines in sleep
properly managed hangover or residual effects should be unlikely,
disorders: a novel experimental and therapeutic approach. New York:
but risk of subjective feelings of sedation increases with an in-
9. Bianchetti G, Dubruc C, Thierclin JF, Bercoff E, Bouchet JL, Emiriau
creasing dose (17). The Physicians Desk Reference (16) notes that
JP, et al. Clinical pharmacokinetcs of zolpidem in various physiological
patients taking zolpidem may experience effects similar to those
and pathological conditions. In: Sauvanet JP, Langer SZ, Morselli PL,
associated with alcohol, and recommends that zolpidem not be
editors. Imidazopyridines in sleep disorders: a novel experimental and
taken with alcohol, since the effects would be additive.
therapeutic approach. New York: Raven Press, 1988;255–63.
10. Pichard L, Gillet G, Bonfils C, Domergue J, Thenot JP, Maurel P. Ox-
Vermeeren et al. (18) have reported on the impairment of actual
idative metbolism of zolpidem by human liver cytochrome P450S. Drug
driving performance resulting from use of zopiclone and zaleplon,
two other recently introduced hypnotic drugs used in the treatment
11. Singh BN Effects of food on clinical pharmacokinetics. Clin Pharma-
of insomnia. They found that zopiclone (7.5 mg), with a half-life of
3.5 to 6 h administered within 10 h of the driving test, produced an
12. Levine B, Wu SC, Smialek JE. Zolpidem distribution in postmortem
cases. J Forensic Sci 1999;44(2):369–71.
increase in lateral drift (weaving) equivalent to a blood alcohol
13. Harvengt C, Hulhoven R, Desager JP, Coupez JM, Guillet Ph, Fuscau E,
concentration of 0.10 g/100 mL. Zaleplon, on the other hand, with
et al. Drug interactions investigated with zolpidem. In: Sauvanet JP,
a much shorter half-life of 0.9 to 1.1 h, produced less next-day se-
Langer SZ, Morselli PL, editors. Imidazopyridines in sleep disorders: a
dation, and no driving impairment when administered as little as 5
novel experimental and therapeutic approach. New York: Raven Press,1988;165–73.
h prior to the driving test. Zolpidem, with a half-life of around 2 h,
14. Roger M, Dallot JY, Salmon O, Neveux E, Gitton JP, Gerson M, et al.
could reasonably be expected to exhibit a potential for hangover ef-
Hypnotic effect of zolpidem in geriatric patients: a dose finding study.
fects, intermediate between these two related hypnotic drugs.
In: Sauvanet JP, Langer SZ, Morselli PL, editors. Imidazopyridines in
Given the specific role of zolpidem as a sleep inducer, its simple
sleep disorders: a novel experimental and therapeutic approach. New
pharmacokinetics, and the known relationship between fatigue,
15. Rush CR. Behavioral pharmacology of zolpidem relative to benzodi-
sleepiness, and decrements in driver performance and the associ-
azepines: A review. Pharm Biochem Behav 1998;61(3):253–9.
ated increased accident risk, it appears reasonable to conclude that
16. Physicians Desk Reference. 53rd edition. Medical Economics Company,
even normal doses of the drug have the potential to affect driving
in a negative way for several hours after use.
17. Borberly AA, Youmbi-Balderer G, Jaggi-Schwarz K. Zolpidem (10 and
20 mg): Hypnotic action and residual effects after a single bedtime dose. In: Sauvanet JP, Langer SZ, Morselli PL, editors. Imidazopyridines in
References
sleep disorders: a novel experimental and therapeutic approach. NewYork: Raven Press, 1988;205–10.
1. Meeker JE, Baselt RC. Six cases of impaired driving following recent
18. Vermeeren A, Danjou PE, O’Hanlon JF. Residual effects of evening and
use of the sleep inducer zolpidem (Ambien®). Presented at the American
middle-of-the-night administration of zaleplon 10 and 20 mg on memory
Academy of Forensic Sciences Annual Meeting, Nashville, TN, Febru-
and actual driving performance. Hum Psychopharm Clin Exp 1998;13
2. Logan BK, Case GC, Gordon A. Carisoprodol, meprobamate and driv-
19. Tharp V, Burns M, Moscowitz H. Development and field test of psy-
ing impairment. J Forensic Sci 2000;45(3):619–23.
chophysical tests for DWI arrest. DOT-HS-8-01970, March 1981.
3. Goeringer K, Raymon L, Christian GD, Logan BK. Postmortem forensic
toxicology of selective serotonin reuptake inhibitors: A review of phar-
Additional information and reprint requests:
macology and report of 168 cases. J Forensic Sci 2000;45(3):633–48.
4. Mattila MJ, Vanakoski J, Kalska H, Seppälä T. Effects of alcohol, zolpi-
Director, Bureau of Forensic Laboratory Services
dem, and some other sedatives and hypnotics on human performance and
memory. Pharm Biochem Behav 1990;59(4):917–23.
5. Greenblatt DJ, Harmatz JS, von Moltke LL, Ehrenberg BL, Harrel L,
Corbett K, et al. Comparative kinetics and dynamics of zaleplon, zolpi-
dem, and placebo. Clin Pharmacol Ther 1998;64:553–61.
Perfect Touch Home Health Care, Inc. PATIENT SERVICES HANDBOOK During the initial phase of care, the Perfect Touch Home Health Care, Inc. registered nurses will visit you for ____________ times a week. The following services are available, should your plan of care indicate such services: Home Health Aide will visit you _____ times a week. Physical Therapy will evalu
SUSPENSION ORALE COMPOSITION Ivermectine…………………….…………………………….………………………. 0,10 g Triclabendazole…………………………………………………….……………….…5,00 g Albendazole……………………………………………………………….……….2,50 g Sélénium (sf. sélénite de sodium, 5H2O)……�
 and half-lives for both the 10 and 20 mg doses were 1.7 and 2 to 2.2
drugs subject to first-pass metabolism by P450 3A4 (11), and this
h, respectively, and both doses effectively induced sleep. The phar-
may increase bioavailability of zolpidem.
and half-lives for both the 10 and 20 mg doses were 1.7 and 2 to 2.2
drugs subject to first-pass metabolism by P450 3A4 (11), and this
h, respectively, and both doses effectively induced sleep. The phar-
may increase bioavailability of zolpidem.