Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Foreverhomegreyhounds.org
Chiara Noli DVM, DipECVD INTRODUCTION Dr Chiara Noli graduated atthe University of Milan in
Leishmaniasis is a disease of human beings and animals caused
by the protozoan parasite of the genus Leishmania. Dogs usually
develop the systemic (visceral) form of infection, with a highly
variable clinical appearance. Canine leishmaniasis may be difficult to
diagnose and frustrating to treat. Dogs are considered the main
reservoir for visceral leishmaniasis in humans. Diploma of the EuropeanCollege of VeterinaryDermatology. Since 1996 sheETIOLOGICAL AGENT works as dermatologyconsultant andLeishmania organisms belong to the genus Protozoa, the order
Kinetoplastida and the family Trypanosomidae. The parasite
requires two different hosts, a vertebrate and an insect, to complete
practice in Milan and in other clinics in Northern Italy. She is
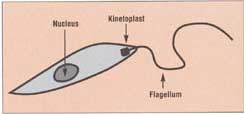
its cycle. The flagellate (promastigote) form is about 10–15 µm long
Past-President of the Italian Society of Veterinary Dermatologyand Board Member of the European Society of Veterinary
and is found in the insect vector and in laboratory cultures
Dermatology. Dr Noli is author of a number of Italian and(Figure 1). In the vertebrate host the parasite is observed in the international papers and of two book chapters. She lectures at
amastigote form (i.e., without flagellum), smaller (2–5 µm), and with
national and international meetings and at veterinary
a visible rod-shaped kinetoplast (Figure 2). The latter is a
mitochondrial structure rich in DNA, associated with the flagellum. The amastigotes are often seen in the intracellular position,particularly in macrophages, where they are able to survive and
KEY POINTS
Several Leishmania species and subspecies, responsible for
● Canine visceral leishmaniasis is a severe systemic
different clinical diseases in man and in the dog, have been identified
disease caused by the diphasic protozoan parasite
(Table 1). Their classification is very complicated: initially they were Leishmania infantum in the Old World and
classified following parasite morphology, insect vector, type of
lesions, serological tests, and geographical distribution (1). Todaymore advanced techniques, involving isoenzymatic patterns, DNA
● The geographical distribution of the disease is
peptide mapping, monoclonal antibodies, cell membrane structure
dependent on its insect vector, the sandflyPhlebotomus spp. in the Old World and Lutzomyiaspp. in the New World.
● Common clinical signs are skin lesions, weight loss,
anorexia, lymphadenopathy, ocular lesions, nasalbleeding, locomotory problems, and muscle atrophy.
● Chronic enteritis and renal failure are the most
● Frequent clinical laboratory findings are polyclonal
Figure 1 Schematic drawing of Leishmania spp. promastigotes.
hyperglobulinemia, hypoalbuminemia,hyperprotinemia, a slight increase in liver enzymes,non-regenerative anemia and thrombocytopenia,azotemia, and creatininemia.
● The definitive diagnosis is obtained by direct
observation of the parasites or serological means.
● The best available therapy today is the combined
use of pentavalent antimonial agents withallopurinol.
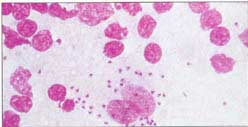
● The prognosis for a complete cure is guarded. Figure 2 Amastigotes of Leishmania infantum in a macrophage from a
● Dogs are the main reservoirs for human visceral
cytological preparation of a fine needle aspiration biopsy of anaffected lymph node-Hemacolor, 1000ן.Courtesy of Dr. Fabia Scarampella.
analysis, and fatty acid analysis have identified at least 17 species
and subspecies (2). The most accepted classification worldwide is
based on isoenzyme electrophoretic analysis. Populations of
Leishmania species, their distribution and the
parasites with similar isoenzyme patterns are called zymodemes. disease they cause in dogs and humans
Another classification is based on analysis of kinetoplast DNA with restriction enzymes and recognizes different schizodemes. Old World Leishmania infantum EPIDEMIOLOGY Leishmania infantum is responsible for the Old World canine
New World
visceral leishmaniasis. This species, with different zymodemes, is
present in all countries around the Mediterranean Sea, in Portugal,
West, East and North Africa, the Middle East, India, and China (2,
Leishmania braziliensis Mucocutaneous
3). Its geographical distribution reflects the living area of the insectvector Phlebotomus spp. This is a small (2–3 mm), silent, nocturnal,blood-sucking sandfly belonging to the family Psychodidae.
is rarely seen in very young and very old dogs because of the long
Phlebotomi are mostly found in rural areas between 100 and 800 m
incubation period (usually more than four months) and the very low
above sea level and spend their life in a limited area, not exceeding
Visceral leishmaniasis in human beings is caused by the same
In some endemic areas of the Mediterranean the incidence of
parasites but is much less common than the canine variety. Most
seropositivity is about 5–15% of the canine population (4–8). Of
human patients have an immunosuppressive disease, such as HIV, or
seropositive dogs, 20–40% are asymptomatic carriers and may
are receiving anti-tumor chemotherapy. Direct transmission from
represent an unrecognized reservoir of the infection for other dogs
dogs to humans without an insect vector is probably impossible,
and human beings (6–8). In some areas the incidence of clinical
although whether contact with open mucosal lesions is entirely
disease is about 3.5 new cases per 100 dogs per year.
The endemic area, and the total number of affected animals, has
been increasing in recent years (4, 6). This could reflect greater
PATHOMECHANISM OF INFECTION
mobility of dog owners with their pets and/or a change in theclimatic conditions that favor the sandflies’ survival in new areas.
The insect vector sucks blood from an infected vertebrate and
Leishmania chagasi is the microorganism that causes the
ingests the amastigote parasites. These multiply in the intestinal
visceral disease in dogs and humans in the New World. This parasite
tissues and transform into promastigotes. The flagellum enables
is inoculated by the bloodsucking sandfly Lutzomyia spp. and its
them to migrate into the insect’s sucking apparatus. With each blood
distribution includes Central and South America and small endemic
meal parasites are deposited into the skin of a new host. They are
areas in North America (Ohio, Alabama, Michigan) (9). In Oklahoma
internalized by macrophages and other dendritic cells, where they
a case involving L. infantum has been described (2). The visceral
can survive and multiply. Leishmanial organisms are able to live in
disease caused by L. chagasi is very similar to the Old World visceral
the endothelial reticulum of host cells because they neutralize the
leishmaniasis, which will be described later.
host cell’s pH and detoxify oxygen metabolites. In macrophages the
Other species of Leishmania which may infect dogs and humans
parasites multiply by binary fission until they rupture the cell and
are L. braziliensis in Brazil, L. tropica in the Mediterranean area,
and L. mexicana in Central America and Texas, USA (2). While the
It has recently been recognized (15) that Langerhans cells and
latter has never been associated with clinical disease in dogs
other dendritic cells may also be infected by the parasite. These cells
(although antibodies against it have been found in the serum of
process and present parasitic antigens on their surface and are able
animals living with affected owners), L. braziliensis and L. tropica
to prime naive T helper (Th) cells and direct their response to the
can cause cutaneous nodules and mucosal ulceration in dogs (10,
infection (16). Resistance to infection depends on a strong Type 1
11). Recently L. mexicana has been isolated from nodular cutaneous
T-helper response (Th1), which involves production of cytokines
lesions in a cat in Texas (12). Rodents, and not dogs, are considered
such as interferon gamma (IFNg), tumor necrosis factor (TNF),
the main reservoir of these species of Leishmania.
interleukin (IL) 2 and IL 12. These cytokines stimulate the cell-
The cases of canine leishmaniasis diagnosed in non-endemic
mediated immunity which eliminates the infection. Animals that
areas are usually in animals which have been imported from endemic
mount a strong Th1 response may have transitory positive serum
areas or which have been living there for some time. Occasionally,
antibody titers or may temporarily harbor the parasites before they
infections following even a short vacation have been reported.
However, autochthonous cases have occasionally been described in
In other individuals disease occurs as a consequence of a Type 2
countries where Phlebotomus spp. are absent (13, 14). In these
T-helper response (Th2), with production of IL4, IL5, IL6 and IL10,
cases the affected animals were born in non-endemic countries and
which in turn promote B-cell proliferation and antibody production.
had never traveled abroad, although they had been in contact with
Unfortunately these antibodies are not protective and may even be
infected animals. This suggests the existence of an alternative insect
detrimental, due to the formation of immune complexes and their
vector – possibly a tick – or other ectoparasite. In one case a dog
subsequent deposition in basement membranes. Antibody-mediated
born in a non-endemic area from an affected bitch developed the
opsonization of parasites may even increase phagocytosis by
disease, suggesting the possibility of transuterine transmission (14).
macrophages and their subsequent parasitosis, according to some
The disease may occasionally be transmitted as a result of blood
authors (2). The cell-mediated immune system of susceptible dogs is
impaired, and lymphocytes have decreased proliferative capacities in
There is no age, breed, or sex predilection for the infection,
vitro if stimulated with Leishmania antigens (17, 18).
although it is thought that toy breeds are less affected, as they often
Infected animals may present with either reaction pattern – that
have an indoor lifestyle. Furthermore, in endemic areas, the disease
is, either they develop a progressive disease with a fatal outcome, or
T H E W O R L D ’ S L E A D I N G A U T H O R I T Y O N P E T C A R E A N D N U T R I T I O N Relative prevalence (%) of different signs in cutaneous leishmaniasis (signs with a prevalence of >4% only) (2, 3, 20, 25)
Generalized lymphadenomegaly, symmetrical
Skin lesions (see Table 3) Figure 3 Dog with leishmaniasis: weight loss and generalized scaling
Acute form of leishmaniasis: fever and generalized
lymphadenopathy and absence of skin lesions
Relative prevalence (%) of different skin lesions (on
Severe renal failure without other signs of leishmaniasis 4
total of affected animals) (3, 20, 25)
they stay asymptomatic. However, in the natural disease both Th1and Th2 cellular subtypes are activated and the variability of the
clinical signs and severity of the disease depends on the balance
between these two systems (17). Asymptomatic animals represent
20–40% of the seropositive population (6–8). Of these about 80% will
The incubation period is very long – between one month and
seven years. In this period the microorganisms disseminate widely,
with a predilection for the bone marrow, lymph nodes, spleen, and
Damage caused by the parasite depends on two factors (19):
● Direct action on the tissues, resulting in the formation of non-
suppurative inflammatory lesions in skin, liver, intestines,kidneys, eyes, and bones.
● Indirect damage caused by immune complex deposition in the
joints and in the basement membranes of kidneys, blood vessels,and eyes, resulting in vasculitis, glomerulonephritis,polyarthritis, and uveitis. CLINICAL DISEASE
Several organs may be affected, as parasites have been found in
every part of the body, except, probably, the central nervous system. For this reason leishmaniasis may have several different clinical features. The relative prevalence of the different signs reported in the literature is summarized in Table 2. Figure 4 Dog with alopecia and scaling dermatitis on the ear.
The main presenting signs are weakness, decreased physical
activity, skin disease and weight loss (Figure 3). The dogs usually
(22) as well as acute fatal hemorrhagic enteritis (20) have both been
appear much older than they are because of the prominent muscular
described associated with leishmaniasis. Enteritis may be the result
atrophy, particularly on the head. Anorexia, if present, is probably
of direct parasitic damage (granulomatous enteritis) or consequence
related to renal failure. Weakness and decreased activity may be the
of the renal failure. A case of acute hemorrhagic pancreatitis has
consequences of anemia, muscle atrophy, polyarthropathy, or
chronic renal failure. Locomotory problems are not very frequent and
A moderate to severe renal insufficiency is often seen in affected
include shifting leg lameness, due to immune-mediated polyarthritis,
dogs. Histopathologically, two types of renal lesions have been
polymiositis, and bone lesions, in which parasites are found in
described (14): membranous glomerulonephritis and an extra-
granulomatous inflammatory groups (20, 21).
membraneous glomerulonephritis, both a consequence of immune-
Leishmanial organisms multiply in the macrophages of the liver,
complex depositions. Proliferative lesions have rarely been seen.
causing a chronic active hepatitis and, occasionally, palpable liver
Associated proteinuria may lead to nephrotic syndrome and
enlargement, vomiting, polyuria and polydipsia, anorexia, and weight
uremia, which is the main cause of death in affected dogs. An
loss. Chronic ulcerative colitis with large bowel diarrhea and melena
acute, rapidly fatal renal insufficiency, without other signs of
Characteristicappearance ofulceration due tovasculitis on thepinnae.Figure 5 Histological appearance of leishmaniasis in the skin (alopecic scaling form): numerous parasitic bodies are seen in macrophages in the subepidermal dermis-Hematoxilin-Eosin, 500ן. Arrows: macrophages full of parasitic bodies. Figure 8 Nodular leishmaniasis: several small cutaneous nodules are visible on the elbow.
rest of the body. Histologically, a diffuse infiltrate of macrophages,lymphocytes and plasma cells is observed in the dermis and
Figure 6 Nasal depigmentation and ulceration and epistaxis.
occasionally subcutis. Parasites, which may be seen in high numbers
inside macrophages (Figure 5), reach the skin by vascular dissemination and their presence in the dermis represents the direct
cause of the dermatitis. Dogs with this form are the most immune
Heart disease and thrombosis have been described (26, 27), but
competent of all affected animals (16).
seem rather infrequent. Epistaxis, often unilateral, is frequentlyseen, and is considered the result of both ulcerative lesions of the
Ulceration (23%) (Figures 6 and 7), particularly affecting bony
nasal mucosa and/or impaired coagulation, due to hyperglobulinemia
prominences, mucocutaneous junctions and extremities. Histological
and thrombocytopenia (2). Clinicians should note that
features include ulceration with a mixed infiltrate and very few
concurrent ehrlichiosis may complicate leishmaniasis in some
parasites. Ulceration may occur due to the direct action of the
areas of the world, and, particularly, may contribute to the
parasites or to the necrotizing vasculitis caused by immune complex
hematological abnormalities cited above.
deposition (25). Dogs with this pattern probably have an
Lymphadenopathy, local or generalized, is one of the most
consistent signs, although occasionally it may be absent. There is a
Multiple nodules of variable sizes, from a few millimeters to
proliferation of B-cell regions, and a depletion of T-cells.
10 cm (12%) (Figure 8). Histologically there are accumulations of
Cytologically the lymph nodes appear strongly reactive, with the
macrophages and high numbers of parasites are observed. Dogs with
presence of plasma cells, eosinophils, and macrophages, some of
this reaction pattern may have an extremely ineffective immune
response against the infection (16) as Langerhans cells are
Antibodies in the aqueous humor and cerebrospinal fluid,
spongiform neuronal degeneration in the brain and cerebellum,mobilization of glial cells, and accumulation of amyloid have recently
A generalized sterile pustular dermatosis (4%) on the trunk.
been described, associated with visceral leishmaniasis in dogs (28).
Histological features include subcorneal pustules with mild dermal,
Skin lesions are frequent in canine leishmaniasis. The relative
non-suppurative infiltrate and very low numbers of parasites. The
prevalence of the different cutaneous signs is shown in Table 3. A
pathogenesis of this form is unknown.
study by Ferrer and co-workers established an association between
In some dogs more than one pattern may be present, perhaps
the type of skin lesions and the level or immunocompetence of the
reflecting the balance between a cell-mediated and a predominantly
affected dogs (29). They recognized four main patterns of
antibody-mediated response. Other less frequent skin lesions
macroscopic and microscopic skin lesions, with different prognostic
associated with leishmaniasis are nasal and digital hyperkeratosis,
onychogriphosis (Figure 9), paronychia, nasal and oral Symmetrical alopecia and a silvery scale (Figure 4) is the
depigmentation, localized hyperpigmented hyperkeratotic plaques
most common presentation, and is reported in 60% of dogs with skin
similar to nevi, ulcerative stomatitis, and nodular dermatofibrosis
disease. The lesions often start on the head and then spread to the
without renal lesions, which disappear with treatment (20). T H E W O R L D ’ S L E A D I N G A U T H O R I T Y O N P E T C A R E A N D N U T R I T I O N Clinical laboratory findings in dogs with visceral leishmaniasis (2, 3, 19, 20, 25)
Hyporegenerative, normocytic normochronic anemia
Leukopenia (normal or low lymphocyte count)
scleritis, and retinal hemorrhage. Iridocyclitis has been observed indogs undergoing treatment and is considered by one author (13) asan allergic manifestation, similar to post-kala-azar leishmaniasis inhumans. CLINICOPATHOLOGICAL FINDINGS
Clinical laboratory abnormalities and their relative prevalence
Figure 10 Ocular lesions: blepharitis, keratoconjunctivitis sicca and
(as reported in the literature) are summarized in Table 4.
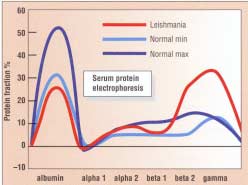
The most frequent abnormality is hyperglobulinemia, due to
polyclonal B-cell activation and antibody production. Hypoalbuminemia may be present and is the result of protein-losing nephropathy, liver disease, and malnutrition. Serum protein electrophoresis has a typical form, strongly suggesting leishmaniasis (Figure 11): a decrease of albumin is associated with an increase in beta- and gamma-globulins. Beta-1 and beta-2 globulins increase in the initial phase of the disease, followed by beta-3 and gamma- globulins. Monitoring serum protein electrophoresis is considered the best way of assessing response to treatment.
Thrombocytopenia and non-regenerative anemia may be the
result of chronic leishmaniasis but the potential for concurrentdiseases to complicate the hematological picture should not beoverlooked. DIFFERENTIAL DIAGNOSES
The differential diagnoses of leishmaniasis are legion, since its
clinical appearance is extremely variable. The alopecic desquamative
Figure 11 Characteristic appearance of serum protein electrophoresis
dermatitis, if not associated with systemic signs, may look similar to
(red line) as it appears during leishmaniasis.
demodicosis, keratinization disorders, sebaceous adenitis, and
Recently a mucosal form, characterized by tissue proliferation on the
pyoderma. The ulcerative lesions have to be differentiated from lupus
penis, tongue, in the nose, and in the mouth, has been described
erythematosus, other causes of vasculitis, deep mycoses, and
(30). In addition, histological features of interface band-like
cutaneous neoplasia. Differential diagnoses of the cutaneous
lymphoplasmocytic cellular dermatitis mimicking lupus
nodules are several skin tumors, sterile or infective granulomas, and
erythematosus have been described with leishmaniasis (3).
nodular dermatofibrosis. Any pustular diseases, including pyoderma,
Ocular lesions involve mainly the anterior segment of the eye
pemphigus foliaceus, and demodicosis, are differential diagnoses.
(Figure 10). Periorbital dermatitis and associated blepharitis is one
If systemic signs are present, leishmaniasis may be confused
of the most common clinical signs. Keratoconjunctivitis sicca may
with other infections, such as ehrlichiosis; clinically they may be
occur, probably due to the direct destructive action of the parasites
very similar, although in ehrlichiosis platelet counts are often
on the lachrymal apparatus (31). Other lesions include
extremely low and petechiae and hemorrhages are often seen. The
granulomatous conjunctivitis refractory to usual treatments,
generalized lymphadenopathy has to be differentiated from
keratitis, granulomatous uveitis, immune complex-mediated anterior
neoplastic lymphoproliferative diseases (malignant lymphoma).
uveitis associated with corneal edema and closed-angle glaucoma,
Polyarthritis, glomerulonephritis, vasculitis, and ulcerative skin
lesions are features observed also in systemic lupus erythematosus
more numerous in the alopecic hyperkeratotic or nodular
(SLE). Furthermore the histological appearance of lupus
dermatitides, but can be very scarce or absent in other cutaneous
erythematosus and of leishmaniasis may be very similar. The
forms, such as the ulcerative or the pustular form. In order to
differentiation of leishmaniasis from SLE may be very difficult, as up
increase the sensitivity of this test, immunohistochemical and
to 30% of the dogs with visceral leishmaniasis may have a (weakly)
immunocytochemical techniques have been developed (34). These
positive antinuclear antibody (ANA), 10% may have a (weakly)
methods achieve the selective demonstration of the parasites by
positive Coombs test (19) and 13% may have a positive lupus
Leishmania spp. can be cultured and isolated from infected
Affected animals may have other concomitant diseases, possibly
tissues in Novy-MacNeal-Nicolle (NMN) medium, where they can be
due to their weak cell-mediated immune responses, such as
observed in the promastigote form. Sensitivity tests to different
demodicosis (25), dermatophytosis (3), and hemoparasitosis such as
drugs may be performed on these cultures. Parasite cultures are not
routinely used in veterinary medicine, because they are difficult andexpensive to perform and because they do not always yield positive
DIAGNOSTIC PROCEDURES
The diagnosis of canine visceral leishmaniasis is difficult for
Serological tests
Several serological tests, which measure circulating antibodies,
● The clinical signs are very variable and may look similar to other
have been developed. Among these, indirect immunofluorescence
(IFAT), Dot-ELISA and direct agglutination test (DAT) are currently
● The histopathological appearance is extremely nonspecific, and
commercially available (18, 35–38). These tests usually have a high
may be similar to that of other infectious or immune-mediated
sensitivity and specificity (80–100%) but cannot be used as the only
means of diagnosis as they may give false positive results in some
● Currently, no available diagnostic test can offer a specificity and
healthy, resistant dogs which have previously come into contact with
the parasite. False negative results may also occur in some affecteddogs which have not produced antibodies (prepatent phase) (20, 36).
The clinical appearance of the affected dog may suggest the
In the latter case it is advisable to repeat the test after six to eight
diagnosis but confirmation of the diagnosis is necessary. Three main
weeks. Furthermore, the serologic titers are not proportionate to the
severity of the clinical disease (36, 38) and are not suitable as a
● Parasitological techniques, whose aim is to visualize the
means of monitoring treatment efficacy because antibody titers may
remain measurable, even after clinical cure (33).
● Serologic tests, which identify circulating anti-leishmanial
Molecular methods
● Molecular methods (polymerase chain reaction), where parasite
A polymerase chain reaction (PCR) technique has been
DNA is amplified and detected in host tissues.
developed recently and is a highly sensitive, and specific, diagnostictest for leishmaniasis (39). Parasitic kinetoplast DNA in liver, spleen,
Parasitological techniques
skin, lymph node, and bone marrow biopsies or blood is selectively
These have a specificity of 100%, but may have a very low
identified and amplified (33), and both fresh and formalin-fixed
sensitivity. The identification of leishmanial organisms in cytological
paraffin embedded tissue can be used for this technique. This test
preparations made from fine needle aspiration biopsies of lymph
can identify the presence of parasites, even in animals which have
nodes and bone marrow is rapid and easy. Bone marrow samples
been clinically cured for years (40). Unfortunately, PCR for
may be collected with a normal needle from the costochondral
Leishmania spp. is currently only available in specialized
junctions or with a spinal needle from the iliac crest or sternum. The
cytological smears are best stained with May-Gruenewald-Giemsa,and the parasites appear as small oval bodies (2–5 µm) containing a
TREATMENT
dark nucleus and a small kinetoplast in a perpendicular position (Figure 2). In bone marrow smears leishmanial organisms are found
Although treatment in the dog achieves clinical cure, it rarely
almost exclusively in macrophages, whereas in cytological
results in complete elimination of the parasites and recurrences are
preparations from lymph nodes they are frequently observed in an
frequent. No drug has yet been developed that safely and quickly
extracellular position, probably due to cell rupture during the sample
eliminates the infection. Current research aims at new therapeutic
collection and preparation. No relationship has been observed
protocols with drugs already in use and the development of new
between the severity of the clinical disease and the number of
drugs (41). Current treatment protocols are summarized in Table 5.
parasites found in cytological smears (20).
Before starting treatment, a complete blood count, biochemical
Leishmanial organisms may also be observed occasionally in
profile and urine analysis (including a quantitative test such as
impression cytological preparations obtained from beneath crusts
urine protein:creatinine ratio) should be performed in order to
and scales, or by fine needle aspiration biopsies from cutaneous
assess the renal and hepatic status. Furthermore, it is necessary to
nodules. Unfortunately, the sensitivity of cytology as a diagnostic
obtain a serum protein electrophoresis profile as a basal value for
tool for canine leishmaniasis is low: bone marrow smears may be
subsequent comparison and evaluation of treatment efficacy.
positive in only about 50–70% of the infected animals (25, 33), andlymph node smears in only about 30% of the cases. This technique
Pentavalent antimonials
also relies strongly upon the skill of the person performing it and on
N-methylglucamine (meglumine) antimonate is currently the
the time devoted to searching for the parasites in the smear, which
drug of choice for canine visceral leishmaniasis. In some countries
should not be less than 10 minutes per sample.
this drug is not available and sodium stibogluconate is used in its
Leishmanial organisms may also be observed in histological
place. Their mechanism of action is not clear: they may inhibit some
sections stained with Hematoxylin-Eosin or with Giemsa. They are
parasite glycolytic enzymes. Meglumine antimonate is not absorbed
T H E W O R L D ’ S L E A D I N G A U T H O R I T Y O N P E T C A R E A N D N U T R I T I O N Allopurinol
Allopurinol is a hypoxantine analog. Leishmanial organisms are
Treatment regimens for canine visceral
not able to synthesize purines and have to use the host molecules. leishmaniasis
Allopurinol is incorporated into the parasite’s RNA and alters proteinsynthesis, inducing synthesis of abnormal proteins. As mammals are
able to synthesize purines, this drug has a very low toxicity for these
species. Allopurinol has a parasitostatic effect, and is best combined
with other antileishmaniacal drugs, such as meglumine antimoniate
(see above) or amphotericin B (see below) in order to potentiate
10–30 mg/kg every 12 hours PO 9–12 months
their effect and obtain longer remission periods. There are few
Amphotericin B 0.5–0.8 mg/kg twice weekly
reports of the successful use of allopurinol alone (38), although this
can represent the sole therapeutic choice in countries where
antimonial compounds are not readily available (47).
interrupt for 2 weeks ifcreatinine > 25 mg/l
Amphotericin B
Amphotericin B is a polyenic antibiotic produced by
Streptomyces nodosus, currently indicated by intravenous
administration for systemic and deep mycoses. It acts by irreversibly
binding to ergosterole, a main component of the leishmanid cell
membrane, causing its disruption and parasite death. Amphotericin
B has some affinity to mammalian cholesterol and is toxic, causing a
decrease in renal blood perfusion, renal filtration, creatinine
clearance, and focal tubular necrosis. Other side effects include
phlebitis, hyperthermia, and vomiting (48). In order to minimize the
side effects it is diluted in 5% dextrose or in saline and administered
by slow intravenous infusion (up to 5 hours). The drug is
administered on alternate days at a dose rate of 0.15–0.5 mg/kg untila cumulative dose of 8–12 mg/kg has been given. Plasma creatinine
if given by mouth and must be injected, preferably every 12 hours, as
should be measured before each administration in order to assess
it has a very short half-life and is quickly eliminated in urine (42).
renal function. Although amphotericin B is 400 times more effective
Subcutaneous injection is preferred to intramuscular or intravenous
than meglumine antimonate against Leishmania spp. its use is
administration because of higher bioavailability (43) and a longer
limited to cases resistant to meglumine antimoniate because of its
half-life (42, 44). Meglumine antimonate, since it is readily excreted
toxic potential and difficult administration. Recently a new protocol
through the kidneys, does not significantly accumulate and has a
has been successfully used by Lamothe to treat 39 cases (48).
very low toxicity. Side effects in the dog are painful local swellings at
Intravenous injections (over 5–30 seconds) at a dosage of
the site of injection, gastrointestinal problems (44), anorexia,
0.5–0.8 mg/kg are given twice weekly until a total dosage of
6–16 mg/kg is reached. Creatinine is measured weekly during this
The initial course of treatment is 50 mg/kg every 12 hours for
period. Drug administration is interrupted for two weeks if creatinine
20 days. This is repeated if no obvious improvement is observed. If,
values become significantly (> 20%) elevated. With this protocol the
after 40 days of treatment, no response is obtained, the Leishmania
investigator obtained up to a 90% clinical cure rate, with only 10%
strain is considered resistant and other therapeutic options must be
chosen. Resistant strains have been repeatedly described, probably
Recently, the efficacy and toxicity of a liposome-encapsulated
due to inappropriate use of the drug by veterinarians or medical
amphotericin B have been evaluated in dogs (49). This formulation is
much less nephrotoxic, as less than 1% is excreted through the
The use of meglumine antimonate does not prevent recurrences,
kidneys, and seems to be effective, although frequent recurrences
which take place in about 75% of cases after 6–8 months (41, 44).
have been observed. The major problem with this formulation of the
Combination with allopurinol increases efficacy and decreases
recurrence rate. Recent protocols (20, 36) advocate the use ofmeglumine antimonate (100 mg/kg every day) until the remission of
Aminosidine
clinical signs in combination with allopurinol (10 mg/kg every
Aminosidine is an aminoglycosidic antibiotic, derived from
8 hours or 20 mg/kg every 12 hours) for 9–12 months. The dogs are
Streptomyces chrestomyceticus, with antimicrobial action against a
monitored with serum protein electrophoresis and if a recurrence is
wide range of microorganisms. It acts by inhibiting normal ribosomal
suspected then meglumine antimoniate is administered again. If the
function and causes abnormal protein production. It is administered
disease does not recur within the first year then allopurinol is
parenterally (IM or SC), as it is not absorbed by mouth, at a dose of
withdrawn and the dog is monitored every 3–6 months for the rest of
5–10 mg/kg twice daily. As with every other aminoglycoside,
aminosidine can be nephro- and ototoxic and should be given only to
Liposome-encapsulated meglumine antimonate may be
dogs with adequate renal function. Some studies have observed that
commercially available in the future. This formulation has the
it gives better results in combination with meglumine antimoniate
advantage of obtaining higher serum concentrations, with decreased
than when the two products are used alone (50).
renal excretion and lower toxicity. Furthermore, liposomes arephagocytosed by macrophages and can exert their action in the
Immunomodulation
cytoplasm and lysosome system where the parasites are located (46).
Prednisolone may be used in dogs with renal insufficiency, if the
use of meglumine antimonate is contraindicated. A dose of 1 mg/kg
of prednisolone is given daily, with allopurinol and appropriate
supportive therapy until renal values (plasma creatinine and urea)
REFERENCES
return to normal. The prednisolone is then suspended and
meglumine antimonate administered at half-dose (50 mg/kg daily)
1. Hommel, M. The genus Leishmania: biology of the parasites and
clinical aspects. Buletin de l’Institut Pasteur 1978; 75: 5–102.
and then, if tolerated, at full dose (20).
Therapy with IFN γ and IL12 has been investigated in human
2. Slappendel, R. J., Ferrer, L. Leishmaniasis. In: Green, C. E. (ed).
medicine. These cytokines induce the shift from a Th2 to a Th1 type
Infectious Diseases of the Dog and Cat, 2nd edn. Philadelphia:
of reaction, thus potentiating the cell-mediated immune system
which is able to eliminate the infection. It is possible that this
3. Kontos, V. J., Koutinas, A. F. Old World Canine Leishmaniasis.
treatment option may be available for dogs in the future. Compendium 1993; 7: 949–959. 4. Mancianti, F., Gramiccia, M., Gradoni, L., Pieri, S. Studies on canine Monitoring therapy
leishmaniasis control. Evolution of infection of different clinical forms of
The best way to monitor the therapeutic effect is serial
canine leishmanasis following antimonial treatment. Transactions of the
evaluation of total plasma proteins and serum protein
Royal Society of Tropical Medicine and Hygiene 1988; 82: 566–567.
electrophoresis. These sequential values are compared with baseline
5. Mansueto, S., Miceli, M. D., Di Rosa, S. et al. Unusual increase of
values obtained before treatment is initiated. Serological titers alone
visceral leishmaniasis of adult in Sicily. Giornale di Malattie Infettive e
are not suitable for the evaluation of the response to treatment as
Parassitologia 1987; 39: 83–88.
they are not related to the severity of the disease (36, 38). A complete
6. Moretti, A., Piergili Fioretti, D., Farinelli, M. Leishmaniosi canina.
cure should be confirmed by a negative cytological examination,
Obiettivi e Documenti Veterinari 1995; 10: 19–25.
disappearance of all clinical signs, normalization of all blood values,
7. Ozon, C., Marty, P., Veyssière, C., Haas, P., Le Fichoux, Y. Résultats
and two negative PCR results performed six months apart (33).
d’une enquête sur la leishmaniose canine effectuée pendant une courte période chez les vétérinaires praticiens des Alpes-Maritimes. Pratique Médical Chirurgienne des Animaux de Compagnie 1995; 30: 199–201. PROGNOSIS 8. Fisas, R. Estudio sobre la estructura y dinamica del foco de
The aim of therapy is to eliminate the parasite and definitively
leishmaniasis del Priorat. Doctoral Thesis, University of Barcelona,
cure the dog. Unfortunately, this is the exception rather than the
rule, as recurrence rates are very high. It has been stated that
9. Bravo, L., Frank, L. A., Brenneman, K. A. Canine leishmaniasis in the
affected dogs have a 75% probability of surviving at least four years if
United States. The Compendium on Continuing Education 1993; 15:
they are given a course of 21–42 days of meglumine antimoniate and
subsequent treatments at every recurrence (2). Dogs having a
10. Pirmez, C., Coutinho, S. G., Marzochi, M. C. A., Nunes, M. P.,
compromised renal function have the worst prognosis. A recent
Grimaldi, G. Canine American cutaneous leishmaniasis: A clinical and
study reported that dogs can be maintained in clinical remission for
immunological study in dogs naturally infected with Leishmania
years with long-term intermittent administration of allopurinol (51). braziliensis in an endemic area of Rio de Janeiro, Brazil. American
In the USA, where sporadic outbreaks of the disease have been
Journal of Tropical Medicine and Hygiene 1988; 38: 52–58.
described, pentavalent antimonial compounds are not readily
11. Morsy, T. A., Schnur, L. F., Feinsod, F. M. et al. Natural infections of
available and are not registered for use in dogs. Euthanasia of
Leishmania tropica major in domestic dogs from Alexandria, Egypt.
infected animals is often performed in order to prevent the
American Journal of Tropical Medicine and Hygiene 1987; 37: 49–52.
transmission of the disease (which is potentially hazardous to
12. Barnes, J. C., Stanley, O., Craig, T. M. Diffuse cutaneous
human beings). However, it has been determined that a dog’s
leishmaniasis in a cat. Journal of the American Veterinary Medical
infective potential correlates with the presence of clinical signs
Association 1993; 202: 416–418.
(especially skin lesions), and treated animals in clinical remission
13. Slappendel, R. J. Canine Leishmaniasis. A review based on 95 cases
are not a source of infection (52). Thus euthanasia should be
in the Netherlands. Veterinary Quarterly 1988; 10: 1–16. 14. Diaz-Espineira, M. M., Slappendel, R. J. A case of autochthonous canine leishmaniasis in the Netherlands. Veterinary Quarterly 1997; PREVENTION AND CONTROL 19: 69–71. 15. Saint-André Marchal, I., Marchal, T., Moore, P. F., Magnol, J. P.,
Prevention and control of canine and human leishmaniasis can
Bourdoiseau, G. Infection of canine Langerhans cells and interdigitating
be achieved by control of sandflies and by taking steps to avoid
dendritic cells by Leishmania infantum in spontaneous canine
exposure to them. In endemic areas dogs should not spend the night
leishmaniasis. Revue de Médecine Vétérinaire 1997; 148: 29–36.
outdoors and fine mesh nets should be applied to the windows. A
16. Fondevila, D., Vilafranca, M., Ferrer, L. Epidermal
recent study demonstrated that the application of a repellent
immunocompetence in canine leishmaniasis. Veterinary Immunology
deltamethrin collar to dogs can protect them from sandflies’ bites
and Immunopathology 1997; 56: 319–327.
and prevent Leishmania infection (53). 17. Pinelli, E., Killink-Kendrick, R., Wagenaar, J. et al. Cellular and
The elimination of all clinically affected dogs has not improved
humoral immune response in dogs experimentally and naturally infected
the human infection rate where it has been imposed (54). However,
with Leishmania infantum. Infection and Immunity 1994; 62:
treatment of all seropositive (symptomatic and asymptomatic dogs)
has significantly decreased the prevalence of new infection cases in
18. Bourdoiseau, G., Bonnefont, C., Hoareau, E. et al. Specific IgG1 and
endemic areas (4). In the future, new prophylactic tools, such as
IgG2 antibody and lymphocyte subset levels in naturally Leishmaniainfantum-infected treated and untreated dogs. Journal of Veterinary Immunology and Immunopathology 1997; 59: 21–30. Acknowledgment 19. Ferrer, L. Leishmaniasis. In: Kirk, R. W., Bonagura, J. D. (eds).
I would like to thank Dr Pedro Ginel of the Veterinary Faculty of
Current Veterinary Therapy XI, Philadelphia: Saunders, 1992:
the University of Cordoba, Spain, for critically reviewing the
20. Denerolle, P. Leishmaniose canine: difficulté du diagnostic et du traitement. Pratique Médicale et Chirurgienne des Animaux de T H E W O R L D ’ S L E A D I N G A U T H O R I T Y O N P E T C A R E A N D N U T R I T I O N REFERENCES Compagnie 1996; 31: 137–145.
identification of asymptomatic carriers by polymerase chain reactionand immunoblotting. American Journal Tropical Medicine and21. Spreng, D. Leishmanial polyarthritis in two dogs. Journal of Small Hygiene 1996; 55: 273–277. Animal Practice 1993; 34: 559–563. 41. Oliva, G., Cortese, L., Ciaramella, P., De Luna, R. Trattamento 22. Ferrer, L., Juanola, B., Ramos, J. A., Ramis, A. Chronic colitis due to
terapeutico della leishmaniosi del cane. Veterinaria 1996; 10: 115–127. Leishmania infection in two dogs. Veterinary Pathology 1991; 28: 342–343. 42. Tassi, P., Ormas, P., Madonna, M. et al. Pharmacokinetic of N- methylglucamine antimoniate after intravenous, intramuscular and 23. Carrasco, L., de Lara, F. C., Martin, E. et al. Acute haemorrhagic
subcutaneous administration in the dog. Research in Veterinary
pancreatitis associated with canine visceral leishmaniasis. VeterinaryScience 1994; 56: 144–150. Record 1997; 141: 519–521. 43. Valladares, J. E., Alberola, J., Esteban, M., Arboix, M. Disposition of 24. Benderriter, T., Casanova, P., Nashkidachvili, L., Quilici, M.
antimony after the administration of N-methylglucamine antimoniate to
Glomerulonephritis in dogs with canine leishmaniasis. Annals of
dogs. Veterinary Record 1996; 138: 181–183. Tropical Medicine and Parasitology 1988; 82: 1–7. 44. Slappendel, R. J., Teske, E. The effect of intravenous or 25. Ciaramella, P., Oliva, G., De Luna, R. et al. A retrospective clinical
subcutaneous administration of meglumine antimoniate (Glucantime) in
study of canine leishmaniasis in 150 dogs naturally infected by
dogs with leishmaniasis. A randomised clinical trial. The VeterinaryLeishmania infantum. Veterinary Record 1997; 141: 539–543. Quarterly 1997; 19: 10–13. 26. Font, A., Durall, N., Domingo, M. Cardiac tamponade in a dog with 45. Gramiccia, M., Gradoni, L., Orsini, S. Decreased sensitivity to
visceral leishmaniasis. Journal of the American Animal Hospital
meglumine antimoniate (Glucantime) of Leishmania infantum isolated
Association 1991; 21: 481–487.
from dogs after several courses of drug treatment. Annals of Tropical27. Font, A., Closa, J. M., Molina, A., Mascort, J. Thrombosis and and Medical Parasitology 1992; 86: 613–620.
nephrotic syndrome in a dog with visceral leishmaniasis. Journal of46. Valladares, J. E., Freixas, J., Alberola, J. et al. Pharmacokinetics of Small Animal Practice 1993; 34: 466–470.
liposome-encapsulated meglumine antimoniate after intramuscular and
28. Garcia-Alonso, M., Nieto, C. G., Blanco, A. et al. Presence of
subcutaneous administration in dogs. American Journal of Tropical
antibodies in the aqueous humour and cerebrospinal fluid during
Medicine and Hygiene 1997; 57: 403–406. Leishmania infantum infections in dogs. Pathological features at the
47. Lester, S. J., Kenyon, J. E. Use of allopurinol to treat visceral
central nervous system. Parasite immunology 1996; 18: 539–546.
leishmaniasis in a dog. Journal of the American Veterinary Medical29. Ferrer, L., Rabanal, R., Fondevila, D., Ramos, J. A., Domingo, M. Skin Association 1996; 209: 615–617.
lesions in canine leishmaniasis. Journal of Small Animal Practice48. Lamothe, J. Essai de traitement de la leishmaniose canine par
1988; 29: 381–388.
l’amphotéricine B (39 cas). Pratique Médicale et Chirurgienne des30. Font, A., Roura, X., Fondevila, D. et al. Canine mucosal Animaux de Compagnie 1997; 32: 133–141.
leishmaniasis. Journal of the American Animal Hospital Association49. Oliva, G., Gradoni, L., Ciaramella, P. et al. Activity of liposomial
1996; 32: 131–137.
amphotericine B (AmBisome ND) in dogs naturally infected with
31. Roze, M. Manifestations oculaires de la leishmaniose canine. Recueil Leishmania infantum. Journal of Antimicrobial Chemotherapy 1995;
de Médecine Vétérinarie 1986; 162: 19. 36: 1013–1019. 32. Moreno, P., Lucena, R., Ginel, P. J. Evaluation of primary 50. Oliva, G., Gradoni, L., Cortese, L. et al. Comparative efficacy of
haemostasis in canine leishmaniasis. Veterinary Record 1998; 142:
meglumine antimoniate and aminosidine sulphate, alone or in
combination, in canine leishmaniasis. Annals of Tropical Medicine and Parasitology 1998; 92: 165–171. 33. Ferrer, L. Leishmaniasis: update in diagnosis and therapy. In: Proceedings of the Fourteenth Annual Congress of the European 51. Ginel, P. J., Lucena, R., Lopez, R., Molleda, M. J. Use of allopurinol Society of Veterinary Dermatology, Pisa, 1997: 33–36.
for maintenance of remission in dogs with leishmaniasis. Journal of Small Animal Practice 1998; 39: 271–274. 34. Ferrer, L., Rabanal, R., Domingo, M., Ramos, J., Fondevila, D. Identification of L. donovani amastigotes in canine tissues by 52. Alvar, J., Molina, R., San Andreas, M. et al. Canine leishmaniasis:
immuneperoxidase staining. Research in Veterinary Science 1988; 44:
clinical, parasitological and entomological follow-up after chemotherapy. Annals of Tropical Medicine and Parasitology 1994; 88: 371–378. 35. Mancianti, F., Pedonese, F., Poli, A. Evaluation of dot enzyme-linked 53. Killick-Kendrick, R., Killick-Kendrick, M., Focheux C. et al. Protection
immunosorbent assay (dot-ELISA) for the serodiagnosis of canine
of dogs from bites of phlebotomine sandflies by deltamethrin collars for
leishmaniasis as compared with indirect immunofluorescent assay.
control of canine leishmaniasis. Medical and Veterinary EntomologyVeterinary Parasitology 1996; 65: 1–9.
1997; 11: 105–111. 36. Ferrer, L., Aisa, M. J., Roura, X., Portus, M. Serological diagnosis and 54. Dietze, R., Barros, G.B., Teixeira, L. et al. Effect of elimination of
treatment of canine leishmaniasis. Veterinary Record 1995; 136:
seropositive canines on the transmission of visceral leishmaniasis in
Brazil. Clinics Infectious Diseases 1997; 25: 1240–1242. 37. Harith, A. E., Slappendel, R. J., Reiter, I. et al. Application of a direct agglutination test for detection of specific anti-leishmania antibodies in the canine reservoir. Journal of Clinical Microbiology 1989; 27: 2252–2257. 38. Vercammen, F., De Deken, R. Antibody kinetics during allopurinol treatment in canine leishmaniasis. The Veterinary Record 1996; 139: 264. 39. Rodgers, M. R., Popper, S. J., Wirth, D. F. Amplification of kinetoplast DNA as a tool in the detection and diagnosis of Leishmania. Experimental Parasitology 1990; 71: 267–275. 40. Berrahal, F., Mary, C., Roze, M. et al. Canine leishmaniasis:
Vacuum Erection Device Use in Elderly Men: APossible Severe Complication Robert L. Bratton, MD, and Harvey D. Cassidy, MD Erectile dysfunction affects up to 30 million Amer-erectile dysfunction. The patient had used a vac-ican men and their partners. Between the ages of 40uum erection device for the last 5 years withoutand 70 years, the probability of complete erectilecomplications. We rece
 Chiara Noli DVM, DipECVD
Chiara Noli DVM, DipECVD
 analysis, and fatty acid analysis have identified at least 17 species
and subspecies (2). The most accepted classification worldwide is
based on isoenzyme electrophoretic analysis. Populations of
Leishmania species, their distribution and the
analysis, and fatty acid analysis have identified at least 17 species
and subspecies (2). The most accepted classification worldwide is
based on isoenzyme electrophoretic analysis. Populations of
Leishmania species, their distribution and the
 Relative prevalence (%) of different signs in
Relative prevalence (%) of different signs in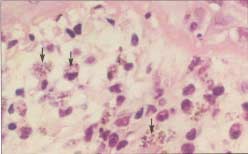




 Characteristicappearance ofulceration due tovasculitis on thepinnae.
Figure 5 Histological appearance of leishmaniasis in the skin
Characteristicappearance ofulceration due tovasculitis on thepinnae.
Figure 5 Histological appearance of leishmaniasis in the skin

 Clinical laboratory findings in dogs with visceral
Clinical laboratory findings in dogs with visceral
 lesions are features observed also in systemic lupus erythematosus
more numerous in the alopecic hyperkeratotic or nodular
(SLE). Furthermore the histological appearance of lupus
dermatitides, but can be very scarce or absent in other cutaneous
erythematosus and of leishmaniasis may be very similar. The
forms, such as the ulcerative or the pustular form. In order to
differentiation of leishmaniasis from SLE may be very difficult, as up
increase the sensitivity of this test, immunohistochemical and
to 30% of the dogs with visceral leishmaniasis may have a (weakly)
immunocytochemical techniques have been developed (34). These
positive antinuclear antibody (ANA), 10% may have a (weakly)
methods achieve the selective demonstration of the parasites by
positive Coombs test (19) and 13% may have a positive lupus
Leishmania spp. can be cultured and isolated from infected
Affected animals may have other concomitant diseases, possibly
tissues in Novy-MacNeal-Nicolle (NMN) medium, where they can be
due to their weak cell-mediated immune responses, such as
observed in the promastigote form. Sensitivity tests to different
demodicosis (25), dermatophytosis (3), and hemoparasitosis such as
drugs may be performed on these cultures. Parasite cultures are not
routinely used in veterinary medicine, because they are difficult andexpensive to perform and because they do not always yield positive
DIAGNOSTIC PROCEDURES
lesions are features observed also in systemic lupus erythematosus
more numerous in the alopecic hyperkeratotic or nodular
(SLE). Furthermore the histological appearance of lupus
dermatitides, but can be very scarce or absent in other cutaneous
erythematosus and of leishmaniasis may be very similar. The
forms, such as the ulcerative or the pustular form. In order to
differentiation of leishmaniasis from SLE may be very difficult, as up
increase the sensitivity of this test, immunohistochemical and
to 30% of the dogs with visceral leishmaniasis may have a (weakly)
immunocytochemical techniques have been developed (34). These
positive antinuclear antibody (ANA), 10% may have a (weakly)
methods achieve the selective demonstration of the parasites by
positive Coombs test (19) and 13% may have a positive lupus
Leishmania spp. can be cultured and isolated from infected
Affected animals may have other concomitant diseases, possibly
tissues in Novy-MacNeal-Nicolle (NMN) medium, where they can be
due to their weak cell-mediated immune responses, such as
observed in the promastigote form. Sensitivity tests to different
demodicosis (25), dermatophytosis (3), and hemoparasitosis such as
drugs may be performed on these cultures. Parasite cultures are not
routinely used in veterinary medicine, because they are difficult andexpensive to perform and because they do not always yield positive
DIAGNOSTIC PROCEDURES
 supportive therapy until renal values (plasma creatinine and urea)
REFERENCES
supportive therapy until renal values (plasma creatinine and urea)
REFERENCES