Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Doi:10.1016/j.ijoa.2005.01.002
International Journal of Obstetric Anesthesia (2005) 14, 212–218Ó 2005 Published by Elsevier Ltd. doi:10.1016/j.ijoa.2005.01.002
A comparison of epidural ropivacaine 0.75% and bupivacaine0.5% with fentanyl for elective caesarean section
Departments of Anaesthetics, St. Mary’s Hospital, London, County Hospital, Hereford and Homerton Hospital,London, UK
Background: Early studies suggested that ropivacaine had clinical advantages over bupivacaine with respect to car-diotoxicity and motor block, and that it was suitable for epidural caesarean section. This study was set up to compareepidural 0.75% ropivacaine with a popular bupivacaine/fentanyl mixture for elective caesarean section. Methods: Eighty women having elective caesarean section under epidural anaesthesia were randomly allocated toreceive 20 mL of either 0.75% ropivacaine or 0.5% bupivacaine plus fentanyl 100 lg. Supplementation with 2% plainlidocaine was used where necessary. Times were recorded for onset of sensory block, density and duration of motorblock, and the need for supplementation. Results: There was no difference between the groups in the time (mean [SD]) to achieve sensory blockade to cold toT4 (ropivacaine 15.8 [5.6] min, bupivacaine/fentanyl 18.7 [9.1] min, P = 0.13) or to S1 (ropivacaine 18.3 [4.6] min,bupivacaine/fentanyl 17.4 [7.6] min, P = 0.59), or in the need for supplementation. However, ropivacaine produced amotor block that was denser (median Bromage score ropivacaine 3, bupivacaine/fentanyl 1.5, P = 0.0041), and oflonger duration (ropivacaine 237 [84] min, bupivacaine/fentanyl 144 [76] min, P < 0.0001). Conclusions: This study suggests that epidural 0.75% ropivacaine without opioid may be used as an alternative tobupivacaine 0.5% with fentanyl for elective caesarean section, but it does not induce anaesthesia any faster and mayresult in a denser, more prolonged, motor block. Ó 2005 Published by Elsevier Ltd.
Keywords: Anaesthesia, obstetrical; Anaesthesia, epidural; Caesarean section; Anaesthesia, local: bupivacaine; Anaesthesia, local:ropivacaine
Of all the solutions in use for providing de novo epi-
dural anaesthesia in the UK, the most popular is proba-
Regional anaesthesia is widely considered the technique
bly a mixture of 0.5% bupivacaine with fentanyl
of choice for caesarean section, and although de novo
50–100 lg. Lidocaine 2% plain or with epinephrine
epidural anaesthesia is currently much less popular than
(popular in North America) is rarely used as a first line
spinal anaesthesia, it is still an important technique.
agent in the UK. However, any mixture of bupivacaineand fentanyl is unlicensed, and since it is not commer-cially available, needs to be made up on an individualbasis. This task is time-consuming and increases the
risks of contamination or drug administration errors.
Ropivacaine 0.5% has been shown to be an effective
Given as an oral presentation at the Obstetric Anaesthetists’
Association Annual Meeting, Nottingham, UK, in May 2002. No
agent for providing epidural anaesthesia for caesarean
additional funding was required for this study.
section, providing similar, satisfactory conditions to
N. Christelis, Department of Anaesthetics, St. Mary’s Hospital,
0.5% bupivacaine.Other workers have used 0.75%
London, J. Harrad, Department of Anaesthetics, County Hospital,
ropivacaine and also found it to be effective.Irestedt
Hereford, P.R. Howell, Department of Anaesthetics, Homerton
and colleagues showed that 20 mL of 0.75% ropivacaine
was enough to provide satisfactory conditions for cae-
Correspondence to: Dr Nick Christelis, Department of Anaesthetics,
sarean, and preferable to the higher dose of 25 mL that
St. Mary’s Hospital, Praed Street, London W2 1NY, UK. E-mail:
produced excessively high sensory blockade.
Epidural ropivacaine and bupivacaine with fentanyl for caesarean section
This study was set up to investigate how plain 0.75%
been given by the investigator, the study solution was
ropivacaine (licensed for epidural use in the UK), com-
given by the second anaesthetist who then left the theatre
pared to the popular (unlicensed) bupivacaine-fentanyl
and took no further part in the case. The solution was given
mixture when establishing de novo epidural block for
slowly over 2 min whilst maintaining verbal communica-
elective caesarean section. The primary aim was to
tion with the patient. All assessments (preoperative, intra-
ascertain if there was any difference in speed of onset
between the two solutions, and secondary aims were to
investigators who were unaware of which epidural solu-
compare the success and quality of sensory blockade,
tion had been administered. The timing period for the
and the extent and duration of motor blockade.
study began once all the study solution had been given.
Electrocardiogram (ECG) and pulse oximetry were
started upon arrival in theatre. An automated sphygmo-manometer recorded maternal arterial pressures every
5 min. All women received a further 1000 mL of Gelo-fusin during surgery. Hypotension (systolic pressure
Following ethics committee approval, this double-blind
<100 mmHg, or a 20% drop from baseline, or symptoms
randomised controlled trial was undertaken at Homerton
of nausea, dizziness or faintness) was treated using addi-
Hospital. Statistical advice had been sought in the plan-
tional fluids and/or ephedrine 3–6 mg boluses.
ning stage and power analysis suggested that 32 patients
The extent of sensory blockade was determined using
were required in each group to detect a 5-min difference
ethyl chloride spray and checked every two minutes un-
in onset time of sensory blockade (80% power,
til surgery began. Recorded times included the time to
P < 0.05). Eighty pregnant women booked for elective
achieve bilateral T4 to S1 sensory blockade, and the
caesarean section were recruited and gave written in-
time the anaesthetists considered the patient ready for
formed consent. All women were ASA I or II, at P36
surgery (Ôready for surgery’ time). In line with clinical
weeks of gestation with a singleton fetus, and over 18
practice, surgery was not allowed to start until bilateral
years old. Women in labour, those unable to communi-
T4 to S1 sensory blockade and bilateral sympathetic
cate in English, those who had had significant back sur-
blockade (warm, dry feet) were demonstrated.
gery, injury or scoliosis, and those known to have an
If the sensory block was inadequate 20 min after the
allergy to amide local anaesthetics were excluded. Wo-
study solution had been given, or if the patient required
men in whom there was any concern about fetal well-
intraoperative supplementation of the block, 2% plain
lidocaine was given via the epidural route to a maximum
All women were premedicated with oral ranitidine
of 10 mL. However, if more than 10 mL of 2% lidocaine
150 mg and metoclopramide 10 mg. On arrival in the
was required for supplementation the subject was with-
theatre suite they were given 25 mL of 0.3 M sodium
drawn from the study and received either spinal or gen-
citrate orally. Hartmann’s solution 1000 mL was given
intravenously. The epidural was performed by either a
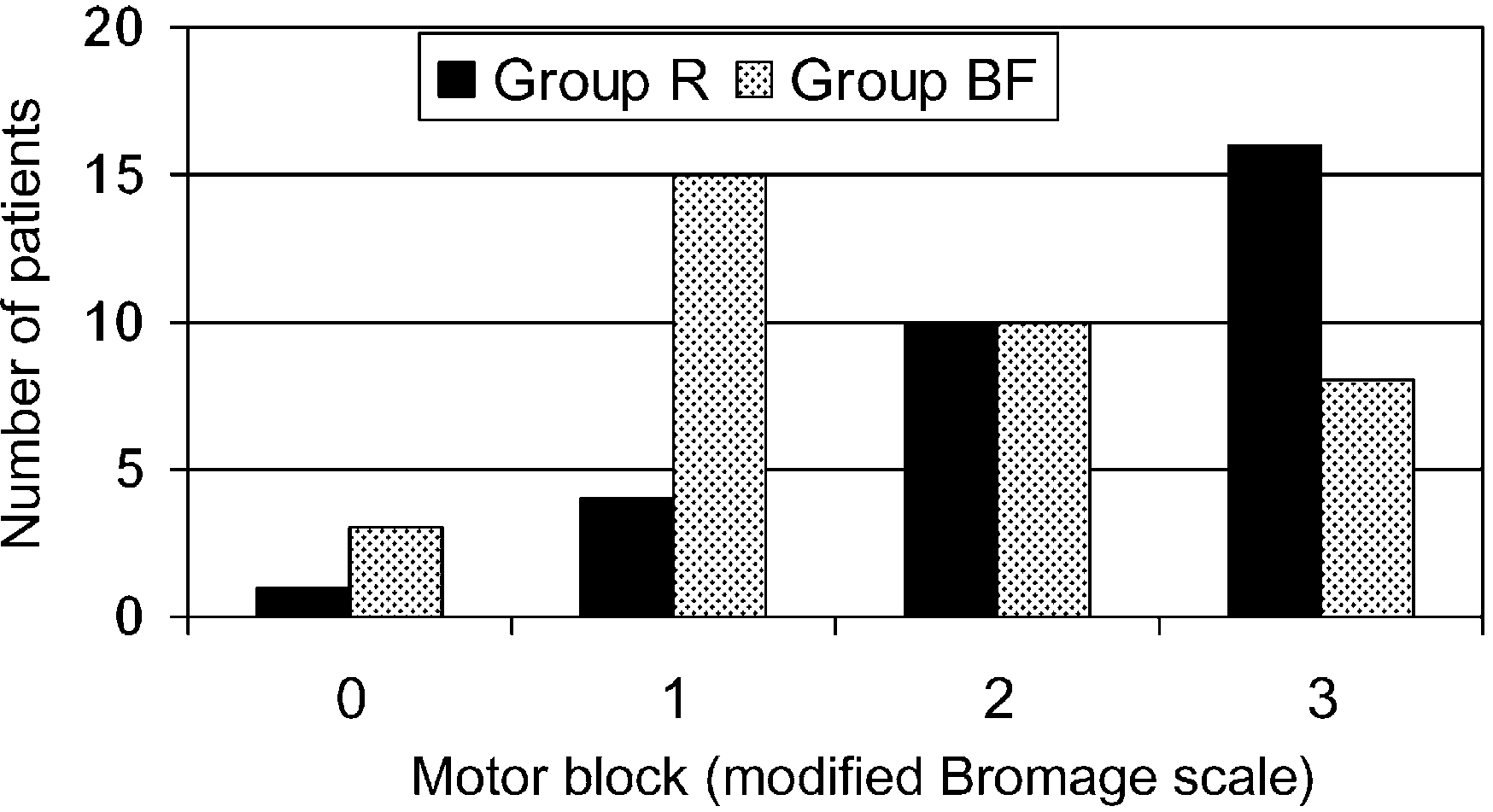
Bilateral motor block was assessed immediately be-
consultant anaesthetist or a trainee with the patient in
fore surgery, at the end of surgery and every 30 min
the sitting or lateral position. The epidural space was
postoperatively until full regression had occurred. A
identified according to normal practice in the L2-3
modified four-point Bromage scale was used (grade
or L3-4 interspace with a 16-gauge Tuohy needle,
0 = able to move hips, knees, feet and lift legs up, grade
bevel cephalad, using a midline approach, with loss
1 = able to move knees and feet, grade 2 = only able to
of resistance to either air or saline. An epidural cathe-
move feet, grade 3 = unable to move hips, knees or feet).
ter was inserted with 3 cm left in the epidural space,
and subjects were then positioned supine with approx-
(6 L minÀ1) via a Hudson mask until delivery of the
imately 15° uterine tilt to the left (ensuring that the
baby, whereupon Syntocinon 10 units (in two divided
abdominal bump looked displaced), and 5° head-up.
doses) and a single dose of antibiotics (co-amoxiclav
A second anaesthetist, not involved in the study, pre-
1000 mg/200 mg) were given intravenously. Assessment
pared and administered the study solution according to
of the baby, according to obstetric protocol, included
instructions found within a pre-randomised, sealed, num-
routine preoperative fetal heart monitoring using a cardi-
bered envelope. Subjects were randomly allocated to re-
otocograph, Apgar scores at 1, 5 and 10 min after deliv-
ceive either 20 mL of 0.75% ropivacaine (group R) or
ery and umbilical cord gas analysis.
20 mL of 0.5% bupivacaine plus fentanyl 100 lg (group
The postoperative analgesic regimen used for all
BF). The hubs of the 20-mL syringes were covered with
women was standard for this hospital at the time of
opaque tape to prevent the investigators detecting the dif-
the study. This comprised intravenous morphine via a
ference in volumes administered (20 mL vs. 22 mL). Five
patient-controlled device (bolus morphine 1 mg, lock-
minutes after a 3-mL test dose of 2% plain lidocaine had
out time 5 min, no background infusion), as well as
International Journal of Obstetric Anesthesia
paracetamol (1 g four times daily) and diclofenac
the outcome of patients following administration of the
(50 mg three times daily) regularly.
In the recovery room, subjects were asked to com-
In group R, 30 women developed a bilateral T4-S1
ment on any pain or discomfort they had felt during sur-
sensory block after just the initial bolus dose of epidural
gery (none, mild, moderate or severe), and whether they
study solution, and two women were removed from the
felt itchy at all (none, mild or severe). The investigating
study due to an obviously inadequate block. Six women
anaesthetist was asked how effective they considered the
were given additional boluses of 2% lidocaine. One of
epidural to have been (poor, fair, good or excellent).
these women never achieved a satisfactory T4-S1 block,
Twenty-four hours after surgery subjects were asked
and was subsequently given spinal anaesthesia. Two wo-
similar questions about their recall of intraoperative pain
men in group R “collapsed” during or immediately after
injection of the initial bolus dose and were withdrawn
Advice from a university lecturer in statistics had
due to suspected intravascular placement of the epidural
been sought in the design of the study, and data were
catheter (one turned out to be a transient vasovagal faint
analysed using two-tailed Student t, v2, Fisher’s exact
– vide infra). Surgery was therefore allowed to start in
and MannWhitney tests as appropriate using the follow-
35 women in group R, and seven of these required intra-
ing software: Excel 2000 (Microsoft Corp., Redmond
operative supplementation according to the protocol.
VA) and Number Cruncher Statistical Systems (NCSS)
Four of these women were subsequently removed from
2000 (NCSS Inc., Kaysville UT). A value of P < 0.05
the study due to intraoperative discomfort, two contin-
was considered statistically significant.
uing under epidural analgesia but requiring protocol-breaking supplementation, and two requiring conversionto general anaesthesia.
In group BF, 26 women achieved a T4-S1 sensory
block after the initial bolus dose alone and the other
There were no statistically significant differences be-
14 required additional boluses of 2% lidocaine. Three
tween the two groups with respect to pre-test variables
of these women were removed from the study since they
such as patient characteristics or technical issues relating
did not achieve a T4-S1 block despite 10 mL of 2% lido-
to siting the epidural. A flow chart () summarises
caine; they received spinal anaesthesia. Surgery was
Good T4-S1 block: Good T4-S1 Good T4-S1 successful case block - start bupivacaine ready for + fentanyl Intraoperative T4-S1 block pain / discomfort: test dose of not present: supplementation given pre-op 2% lidocaine 2% lidocaine supplement Failed or ropivacaine inadequate block: patient withdrawn from study “collapse”
Flowchart depicting the progress and outcome of women in the study. The figures in square boxes represent the number of subjects;
BF = bupivacaine/fentanyl group; R = ropivacaine group.
Epidural ropivacaine and bupivacaine with fentanyl for caesarean section
therefore allowed to start in 37 women in group BF,and intraoperative supplementation was required byten women, one of whom was taken out of the studyas she required protocol-breaking supplementation forintraoperative pain.
Analysing the data, there was no significant differ-
ence between the two local anaesthetic solutions in thetime taken to achieve bilateral T4 or S1 sensory block,or to be ready for surgery However, the den-sity of motor blockade at the start of surgery was greaterin group R than group BF (P = 0.0041) (and
Motor block immediately before surgery.
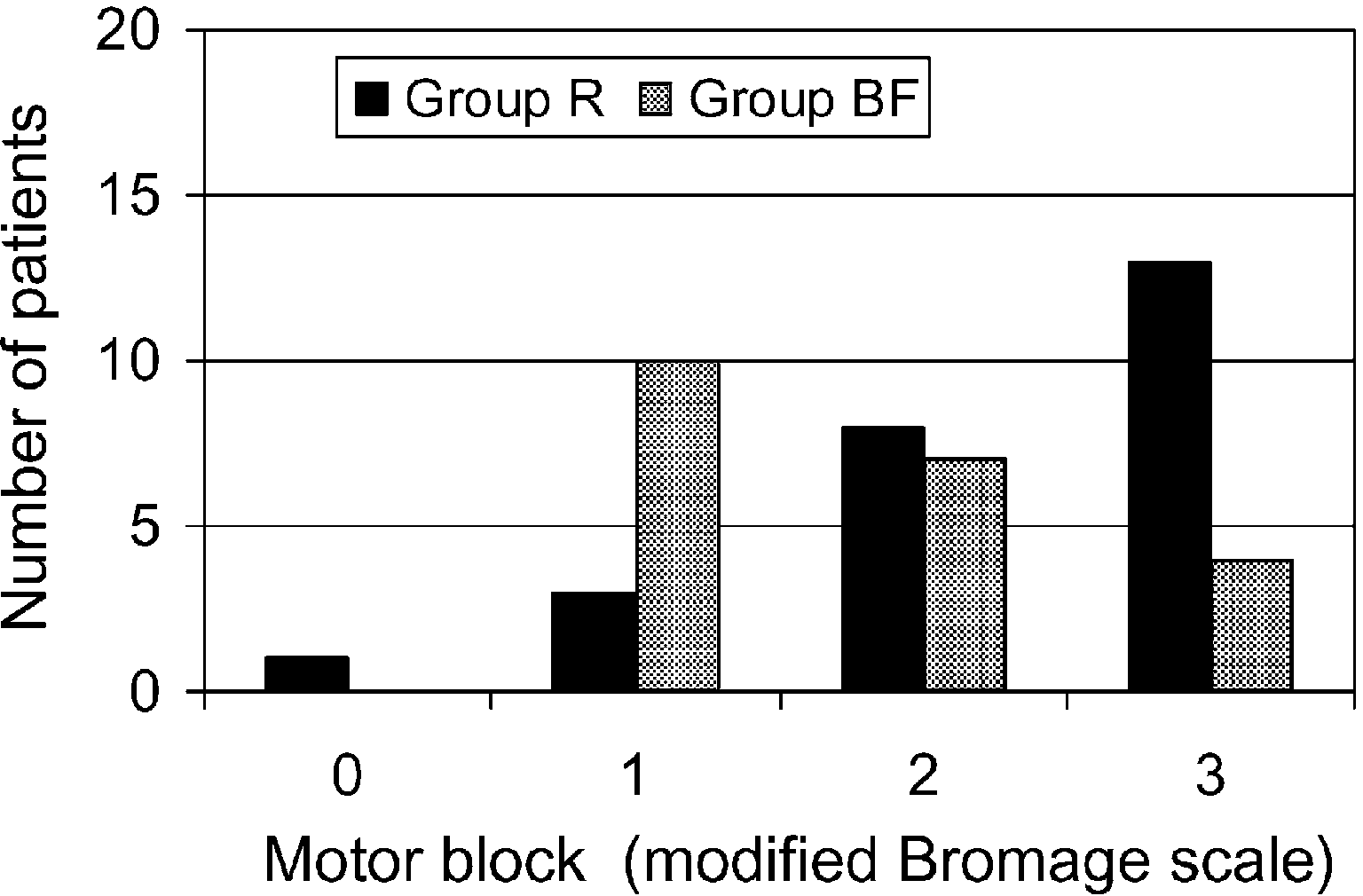
there was a highly significant difference in the durationof motor blockade, taking much longer to wear off com-pletely in group R compared to group BF (R237 € 84 min, BF 144 € 76 min, P < 0.0001). Whenanalysed separately, the data for the subset of 46 womenwho required nothing but the test dose and study solu-tion showed similar results (with no differencein time to achieve T4 sensory block, but a densermotor block in group R at the start of surgery(P = 0.018) ), and a significantly prolonged motorblock (P = 0.00046) in group R.
There were no differences between the groups in
duration of surgery, exteriorisation of the uterus, esti-
Motor block immediately before surgery in the subset of
mated blood loss, or sterilisation procedure (
women in whom no supplementation was required, so they received
Slightly more intravenous fluids were administered in
group R (2250 mL) compared to group BF (2034 mL)(P = 0.03), and there was a trend to greater ephedrineusage in group R, but this did not reach statistical signif-
(Twenty-four hours after surgery, women in
icance (P = 0.07). Neonatal outcome was good in both
group BF recalled having had more intraoperative pain
groups, with only three babies delivered with Apgar
and discomfort than those in group R (P = 0.04) (
scores <7 at 1 min; all babies had Apgar scores P8 at
). Only one patient admitted to pruritus in the recovery
5 min, and 10 at 10 min after delivery. There was no dif-
room, and although the recall of pruritus had increased
ference in neonatal umbilical artery pH values (
by 24 h after surgery, there was no difference in inci-
Immediately after surgery, in the recovery room,
dence between the groups (R 27%, BF 31%, P = 0.75),
there was no difference between the groups in qualita-
and only two women in each group considered the itch-
tive assessments of intraoperative pain (nor
ing was severe. There was no difference in the 24-h
in the anaesthetists’ assessment of epidural success
consumption of intravenous morphine via a patient-con-
(87% of epidurals in group R were rated “excellent”
trolled device (R 27.7 € 18.6 mg, BF 30.3 € 17.9 mg,
or “good” compared to 75% in group BF, P = 0.60)
Sensory and motor block in all women who achieved a satisfactory T4-S1 sensory block, (including data for subset of women who
did not require additional lidocaine supplementation to achieve T4-S1 sensory block)
Values are mean (SD) or median (IQR [range]).
International Journal of Obstetric Anesthesia
Intraoperative data for all women who achieved a satisfactory T4-S1 sensory block
Values are mean (SD), median (IQR [range]) or number (proportion).
Patient assessments of the severity of intraoperative pain and discomfort immediately after the operation, and 24 h later
Values are number (proportion). a Follow-up data not available for all patients. There was a significant difference between groups R and BF 24 h post-op for severe pain anddiscomfort. P = 0.04.
cently, the same up-down sequential allocation tech-nique has been used to demonstrate that the motor
When ropivacaine was first released it was widely pro-
blocking potency of ropivacaine is similarly less than
moted as a potentially superior agent to bupivacaine be-
that of It is unclear whether these differ-
cause of lower toxicity and less motor block. Animal
ences in potency apply when using stronger anaesthetic
studies suggested that ropivacaine is less cardiotoxic
concentrations, but if this were the case, then having to
than bupivacaine, and in pregnant sheep it takes twice
use a larger dose of ropivacaine to achieve a satisfactory
the dose of ropivacaine to cause circulatory collapse
sensory block would erode much of the potential bene-
and death compared to bupivRopivacaine pro-
fits of reduced cardiotoxicity and motor blockade. There
duces fewer arrhythmias than bupivacaine in the isolated
have also been isolated reports of prolonged motor
perfused rabbit heartand when given to human volun-
teers by intravenous infusion it was better tolerated, and
important for women in labour than those undergoing
associated with less reduction in myocardial contractil-
operative delivery, persistent motor blockade may delay
ity and conductivity than bupivacaine.In addition,
postoperative mobilisation, and is greatly disliked by
early clinical studies showed that ropivacaine 0.5% pro-
duced less motor blockade than bupivacaine 0.5%.
In studies at caesarean section where epidural ropiva-
The other great hope for ropivacaine was the separa-
caine has been compared to bupivacaine, most have used
tion of sensory and motor blockade. Studies in both
0.5% solutions in similar doses and found them equally
obstetric and non-obstetric patients showed that epidural
ropivacaine produced less intense and shorter lasting
0.75% with bupivacaine 0.5%. Veneziani and colleagues
motor block than bupivacaine.This has been
found ropivacaine 0.75% with fentanyl clinically supe-
widely hailed as a significant advantage for obstetric pa-
rior to bupivacaine 0.5% with fentanyl using similar vol-
tients in whom motor block is both unnecessary and un-
umes (and consequently a 50% increase in dose)
Bjornestadt and colleagues found plain ropivacaine
However, several recent studies have challenged the
0.75% equally effective as bupivacaine 0.5%, but with
validity of both these apparent benefits of ropivacaine.
a similar 50% increase in dose of ropivacaine.From
The development of the concept of minimum local
these studies, which are largely underpowered to com-
anaesthetic concentration (MLAC) has suggested that
pare quality of sensory blockade, it is difficult to ascer-
ropivacaine, at least in weak concentrations as used for
tain whether or not ropivacaine and bupivacaine are
labour analgesia, is approximately 40% less potent than
equipotent at this end of the concentration spectrum.
bupivacaine with respect to sensory block.More re-
However, both 0.5% and 0.75% ropivacaine appear to
Epidural ropivacaine and bupivacaine with fentanyl for caesarean section
be effective solutions for providing epidural anaesthesia
is that blood had been seen in the epidural catheter when
it was first sited, but (in accordance with common prac-
One of the main stimuli for carrying out our study
tice) the catheter had been pulled back and flushed, and
was a local clinical impression that plain ropivacaine
had appeared to be safe to use. This is a salient reminder
0.75% produced an effective epidural block more
that epidural catheters are never truly safe, and that par-
quickly than the usual alternative, bupivacaine 0.5%
ticular care and vigilance is necessary when a bloody tap
with fentanyl 100 lg. However, the results of our study
has been observed. In addition, using epinephrine in the
do not support that contention, demonstrating similar
epidural solution might have aided in the early detection
onset times for sensory blockade. To our surprise, the
main difference observed was that ropivacaine 0.75%
The other patient who “collapsed” during the admin-
is associated with a much longer-lasting motor block
istration of the study solution (stopped after 14 mL)
and more varied Bromage scores than the bupivacaine-
developed bradycardia, hypotension and reduced level
of consciousness. This was initially feared to be the re-
block from ropivacaine took about 60% longer to wear
sult of local anaesthetic toxicity from accidental intrave-
nous administration, but it became clear quite quickly
Our data were analysed on a per-protocol basis,
that actually this was a vasovagal faint, and she recov-
including all subjects whether or not they needed addi-
ered rapidly after the administration of small doses of
tional lidocaine to achieve a satisfactory block. Similar
atropine and ephedrine. She was removed from the
results were found when separate analysis was per-
study, but went on to develop an excellent block after
formed on the subset of patients who needed no supple-
a total of 20 mL of the study solution (ropivacaine)
mentation of the study drugs; in other words, the results
and her caesarean section was performed under epidural
may be taken to reflect the true nature of the epidural
solutions under test (). The only difference ob-
In this study of 80 women undergoing caesarean sec-
served between this subset and the main dataset was that
tion under epidural anaesthesia, six (7%) were given
women in group BF achieved S1 sensory block 4 min
spinal anaesthesia and three (4%) were given general
faster than those in group R (P = 0.012).
anaesthesia. This failure rate is higher than one would
No difference in the incidence of hypotension was
wish in normal clinical practice, but importantly, only
detected between the groups. However, there was a sug-
two women required emergency intraoperative conver-
gestion that sympathetic blockade needed more aggres-
sion to general anaesthesia for pain and discomfort. This
sive management in the ropivacaine group; slightly
is consistent with the results from a recent survey of UK
more intravenous fluids were required, as well as a
practice, which showed that the mean rate of intraoper-
greater dose of ephedrine, although this did not reach
ative conversion from epidural to general anaesthesia
was 6%, with very wide inter-hospital variation.
Evidence suggests that ropivacaine is less cardiotoxic
The relatively poor performance of epidural anaes-
than bupivacaine on a mg-to-mg basis, and several pa-
thesia in this study was disappointing (supporting the
tients have been known to have received accidental
widespread popularity of spinal anaesthesia for elective
intravenous doses of strong ropivacaine with little seri-
caesarean section) and is probably a reflection of several
ous ill-effects.However, toxicity is still an important
factors. Firstly, this study was performed in a teaching
issue, and convulsions have been reported by other
establishment where the epidurals were performed by
workers.In only one of these cases was there any
a number of different anaesthetists of varying experi-
evidence of significant cardiac toxicity, which occurred
ence, and several of the failures appeared to be techni-
cal. Secondly, sensory block was tested with ethyl
chloride spray. Although using cold sensation is a
In our study, one patient experienced symptoms sug-
widely practised technique amongst obstetric anaesthe-
gestive of central nervous system toxicity (tinnitus, ver-
tists in the UK,it is now apparent that light touch
tigo and tingling around mouth and throat) after
may be a more reliable tool for assessing adequacy of
receiving 150 mg of ropivacaine. This was followed
the sensory block for pain-free surgery.
by a short period of loss of consciousness, but the car-
This study was designed to test whether one new li-
diovascular system was at no point compromised. There
censed drug could effectively replace the commonly
were no visible seizures and she recovered quickly, but
used unlicensed mixture of bupivacaine and fentanyl,
she was taken out of the study and given general anaes-
and the opioid was therefore omitted from the ropiva-
thesia for her caesarean section. She was considered to
caine group. However, since the licensing of drugs fre-
have received only a partial intravenous dose since she
quently lags behind clinical practice, and the use of
did develop a T8-S1 sensory block, so some of the dose
drugs “off-label” is widespread, particularly in obstet-
appears to have reached the epidural space. Of note here
rics, licensing is perhaps not such a significant issue.
International Journal of Obstetric Anesthesia
In addition, pruritus does not seem to have been a signif-
infusions of ropivacaine, bupivacaine and placebo in volunteers.
icant problem in group BF, and therefore withholding
11. Scott D B, Lee A, Fagan D, Bowler G M R, Bloomfield P, Lundh
fentanyl from the ropivacaine group was probably
R. Acute toxicity of ropivacaine compared with that of
unnecessary and unhelpful. Ropivacaine is also consid-
bupivacaine. Anesth Analg 1989; 69: 563–569.
erably more expensive than racemic bupivacaine plus
12. Brockway M S, Bannister J, McClure J H, McKeown D,
Wildsmith J A W. Comparison of extradural ropivacaine and
fentanyl, and the increased cost cannot be justified on
bupivacaine. Br J Anaesth 1991; 66: 31–37.
13. Morrison L M M, Emanuelsson B M, McClure J H, et al. Efficacy
Our results confirm that plain ropivacaine 0.75% can
and kinetics of extradural ropivacaine: comparison withbupivacaine. Br J Anaesth 1994; 72: 164–169.
be used as the local anaesthetic for epidural elective cae-
14. Capogna G, Celleno D, Fusco P, Lyons G, Columb M. Relative
sarean section. However, it showed no clinical advan-
potencies of bupivacaine and ropivacaine for analgesia in labour.
15. Polley L S, Columb M O, Naughton N N, Wagner D S, van de Ven
0.5% + fentanyl 100 lg, and, contrary to expectation,
C J M. Relative analgesic potencies of ropivacaine and
produced a denser and more prolonged motor block.
bupivacaine for epidural analgesia in labor: implications fortherapeutic indexes. Anesthesiology 1999; 90: 944–950.
16. Lacassie H J, Columb M O, Lacassie H P, Lantadilla R A. The
relative motor blocking potencies of epidural bupivacaine and
ropivacaine in labor. Anesth Analg 2002; 95: 204–208.
17. Buggy D J, Allsager C M, Coley S. Profound motor blockade with
The authors thank Mrs. Janice Thomas, Statistician at the Medical Col-
epidural ropivacaine following spinal bupivacaine. Anaesthesia
lege of St. Bartholomew’s Hospital, for her statistical advice in the de-
sign phase of the study, and Dr. Roshan Fernando of the Royal Free
18. Buggy D J, Hall N A, Shah J, Brown J, Williams J. Motor block
Hospital for his advice and assistance in analysing the results.
during patient-controlled epidural analgesia with ropivacaine orropivacaine/fentanyl after intrathecal bupivacaine for caesareansection. Br J Anaesth 2000; 85: 468–470.
19. Baldwin E S, Turner M A. Profound motor blockade with epidural
ropivacaine. Anaesthesia 2000; 55: 91.
1. Shibli K U, Russell I F. A survey of anaesthetic techniques used
20. Crosby E, Sandler A, Finucane B, et al. Comparison of epidural
for caesarean section in the UK in 1997. Int J Obstet Anesth 2000;
anaesthesia with ropivacaine 0.5% and bupivacaine 0.5% for
caesarean section. Can J Anaesth 1998; 45: 1066–1071.
2. Alahuhta S, Rasanen J, Jouppila P, et al. The effects of epidural
21. Veneziani A, Gambi D, Cecchi A, Messeri E, Santagostino G.
ropivacaine and bupivacaine for cesarean section on uteroplacental
Epidural anesthesia for cesarean section: a double blind
and fetal circulation. Anesthesiology 1995; 83: 23–32.
comparison of ropivacaine 7.5 mg/mL and bupivacaine 0.5 mg/mL
3. Datta S, Camann W, Bader A, VanderBurgh L. Clinical effects and
associated with fentanyl 100 mcg. Poster presentation: World
maternal and fetal plasma concentrations of epidural ropivacaine
Congress of Anaesthesiologists, Montreal; 2000.
versus bupivacaine for cesarean section. Anesthesiology 1995; 82:
22. Bjornestad E, Smedvig J P, Bjerkreim T, Narverud G, Kolleros D,
Bergheim R. Epidural ropivacaine 7.5 mg/ml for elective
4. Griffin R P, Reynolds F. Extradural anaesthesia for Caesarean
Caesarean section: a double-blind comparison of efficacy and
section : a double-blind comparison of 0.5% ropivacaine with
tolerability with bupivacaine 5 mg/ml. Acta Anaesthesiol Scand
0.5% bupivacaine. Br J Anaesth 1995; 74: 512–516.
5. Irestedt L, Emanuelsson B-M, Ekblom A, Olofsson C, Reventlid
23. Abouleish E I, Elias M, Nelson C. Ropivacaine-induced
H. Ropivacaine 7.5 mg/ml for elective Caesarean section. A
seizure after extradural anaesthesia. Br J Anaesth 1998; 80:
clinical and pharmacokinetic comparison of 150 mg and 187.5 mg.
Acta Anaesthesiol Scand 1997; 41: 1149–1156.
24. Muller M, Litz R, Hubler M, Albrecht D M. Grand mal convulsion
6. Morton C P J, Bloomfield S, Magnusson A, Jozwaik H, McClure J
and plasma concentrations after intravascular injection of
H. Ropivacaine 0.75% for extradural anaesthesia in elective
ropivacaine for axillary brachial plexus blockade. Br J Anaesth
Caesarean section: an open clinical and pharmacokinetic study in
mother and neonate. Br J Anaesth 1997; 79: 3–8.
25. Plowman A N, Bolsin S, Mather L E. Central nervous system
7. Santos A C, DeArmas P I. Systemic toxicity of levobupivacaine,
toxicity attributable to epidural ropivacaine hydrochloride.
bupivacaine, and ropivacaine during continuous intravenous
Anaesth Intensive Care 1998; 26: 204–206.
infusion to nonpregnant and pregnant ewes. Anesthesiology 2001;
26. Ruetsch Y A, Fattinger K E, Borgeat A. Ropivacaine-induced
convulsions and severe cardiac dysrhythmia after sciatic block.
8. Nancarrow C, Rutten A J, Runciman W B, et al. Myocardial and
Anesthesiology 1999; 90: 1784–1786.
cerebral drug concentrations and the mechanisms of death after
27. Bourne T M, deMelo A E, Bastianpillai B A, May A E. A
fatal intravenous doses of lidocaine, bupivacaine, and ropivacaine
survey of how British obstetric anaesthetists test regional
in the sheep. Anesth Analg 1989; 69: 276–283.
anaesthesia before Caesarean section. Anaesthesia 1997; 52:
9. Pitkanen M, Covino B G, Feldman H S, Authur G R. Chronotropic
and inotropic effects of ropivacaine, bupivacaine, and lidocaine in
28. Russell I F. Testing regional anaesthesia before Caesarean section.
the spontaneously beating and electrically paced isolated, perfused
rabbit heart. Reg Anesth 1992; 17: 183–192.
29. Howell P R, Madej T H. Administration of drugs outside of
10. Knudsen K, Beckmann Suurkula M, Blomberg S, Sjovall J,
Product Licence: awareness and current practice. Int J Obstet
Edvardsson N. Central nervous and cardiovascular effects of i.v.
Process, not Prozac Bapak defined the three words that make up the acronym Subud as: ‘ Susila means having the quality of humanity; budhi means the power of the greatness of God that is within the self of a human being; and dharma means the utmost surrender to the greatness of God by a human being….’ 59 SFO 1 As budhi is inherent, I infer that we al have the potential to be a Ga
APPLICATION FORM STUDENT INFORMATION (Please write in capital letters!) First Name(s) (please underline name used) GUARDIAN(S) INFORMATION Guardian 1 Guardian 2 Please tick if you are the child’s only guardian Square d'Argenteuil 5, B-1410 Waterloo, Belgium STUDENT INFORMATION Has the student had any type of learning support p
 Epidural ropivacaine and bupivacaine with fentanyl for caesarean section
therefore allowed to start in 37 women in group BF,and intraoperative supplementation was required byten women, one of whom was taken out of the studyas she required protocol-breaking supplementation forintraoperative pain.
Epidural ropivacaine and bupivacaine with fentanyl for caesarean section
therefore allowed to start in 37 women in group BF,and intraoperative supplementation was required byten women, one of whom was taken out of the studyas she required protocol-breaking supplementation forintraoperative pain.