Sildenafil Inhibits Altitude-induced Hypoxemia and Pulmonary Hypertension Jean-Paul Richalet, Pierre Gratadour, Paul Robach, Isabelle Pham, Miche`le De´chaux, Aude Joncquiert-Latarjet, Pascal Mollard, Julien Brugniaux, and Je´re´my Cornolo
Laboratoire Re´ponses cellulaires et fonctionnelles a` l’hypoxie, Universite´ Paris 13, Bobigny; Service de Physiologie et Explorations Fonctionnelles,ho
ˆpital Avicenne, Bobigny; Service d’Anesthe´sie-re´animation, ho
ˆtel Dieu, Lyon; Service de Physiologie, ho
Ecole Nationale de Ski et d’Alpinisme, Chamonix; Laboratoire de Physiologie, ho
Exposure to high altitude induces pulmonary hypertension that
responsible for the limitation in aerobic performance, among
may lead to life-threatening conditions. In a randomized, double-
which O2 transfer within the lungs, cardiac output, and tissue
blind, placebo-controlled study, the effects of oral sildenafil on
diffusion of O2 may play an important role (5). Altogether, acute
altitude-induced pulmonary hypertension and gas exchange in nor-
altitude-induced hypoxemia leads to an adverse condition where,
mal subjects were examined. Twelve subjects (sildenafil [SIL] n ϭ
at least, overall well-being is altered by AMS and reduction in
6; placebo [PLA] n ϭ 6) were exposed for 6 days at 4,350 m. Treat-
performance, and life is possibly threatened by the development
ment (3 ϫ 40 mg/day) was started 6 to 8 hours after arrival from sea
of high Ppa and HAPE. Any treatment or condition that limits
level to high altitude and maintained for 6 days. Systolic pulmonary
the increase in Ppa and reduces the altitude-induced hypoxemia
artery pressure (echocardiography) increased at high altitude be-
may be beneficial for humans acutely exposed to high altitude. fore treatment (ϩ29% versus sea level, p Ͻ 0.01), then normalized
The treatment currently recommended for HAPE is rapid
in SIL (Ϫ6% versus sea level, NS) and remained elevated in PLA
reoxygenation combined with a calcium-channel blocker (6, 7). (ϩ21% versus sea level, p Ͻ 0.05). Pulmonary acceleration time
The partial efficacy of this treatment and its systemic adverse
decreased by 27% in PLA versus 6% in SIL (p Ͻ 0.01). Cardiac output and systemic blood pressures increased at high altitude then
effects (hypotension), however, limit its use. Inhalation of nitric
decreased similarly in both groups. Pa
oxide has also been used, and has demonstrated its efficacy in
was higher and alveolar- arterial difference in O
this condition, but its use in the field is difficult (8). l-Arginine
2 lower in SIL than in PLA at rest and exercise (p Ͻ 0.05). The altitude-induced decrease in maximal O
supplementation has also been found to improve gas exchange
2 consump- tion was smaller in SIL than in PLA (p Ͻ 0.05). Sildenafil protects
at high altitude, further suggesting that the nitric oxide synthase
against the development of altitude-induced pulmonary hyperten-
(NOS)–nitric oxide system is involved in the hemodynamic
sion and improves gas exchange, limiting the altitude-induced hy-
changes in the lungs (9). Recently, sildenafil, a selective inhibitor
poxemia and decrease in exercise performance.
of type-5 phosphodiesterase, has been shown to lower Ppa andwas used successfully in the treatment of severe primary or
Keywords: cardiac output; exercise; gas exchange; hypoxia
secondary pulmonary hypertension (10–18). In most cases, sil-denafil was not given as a unique treatment but associated with
Exposure to high altitude leads to hypoxemia, which induces
inhaled nitric oxide, intravenous epoprostenol, or inhaled ilo-
several physiologic or pathophysiologic responses in normal hu-
prost. Only two studies have evaluated the effect of oral sildenafil
mans. Among those, the hypoxic pulmonary vasoconstriction
(50–100 mg, single dose) in normal subjects exposed to acute
leads to an increase in pulmonary artery pressure (Ppa), which
hypoxia, in a randomized double-blind study (13, 14): hypoxia-
may have adverse consequences. High Ppa has been recognized
induced increase in Ppa was almost abolished with sildenafil
to be one of the main causing factors of high-altitude pulmonary
and no important effect on systemic circulation was observed.
edema (HAPE), a serious acute condition that has a mortality
Deleterious effects of high altitude occur after several hours of
rate of 44% in untreated patients (1, 2). Moreover, ventilation–
exposure, however, and no double-blind controlled study has
perfusion mismatch has been correlated to increasing Ppa at
evaluated the effect of sildenafil on the adverse effects of pro-
high altitude, probably by the development of interstitial and
longed altitude exposure in normal humans. Sildenafil has also
perivascular edema, aggravating the hypoxemia (3). In the early
been reported to increase arterial Po2 (17) and improve physical
phase of exposure to high altitude, signs of acute mountain
performance (14, 15, 18) in various cases of severe pulmonary
sickness (AMS) may develop and have been shown to be
hypertension, but no study has explored the effect of a several-
worsened by aggravating hypoxemia, although the precise mech-
day treatment by sildenafil on these variables in normal subjects
anisms of AMS have not been elucidated (4). Altitude hypoxia
induces a dramatic decrease in physical aerobic performance, as
The objective of the present study was to explore the effects
assessed by the maximal O2 consumption (4). Several steps in
of oral sildenafil in normal subjects exposed for 6 days to an altitude
the oxygen transport from the ambient air to the cell can be
of 4,350 m, in a randomized double-blind placebo-controlledmanner. The hypothesis was that sildenafil would reduce thehypoxia-induced increase in Ppa and ameliorate the pulmonaryhemodynamics and gas exchange conditions, increasing the arte-
(Received in original form June 24, 2004; accepted in final form October 24, 2004)
rial Po2, alleviating the clinical symptoms, and limiting the reduc-tion in aerobic performance. Some of the results of this study
Supported by a grant from Pfizer S. A. France.
have been previously reported in the form of abstracts (19, 20).
Correspondence and requests for reprints should be addressed to Jean-Paul Richa-let, M.D., Ph.D., UFR. SMBH, 74 rue Marcel Cachin, 93017 Bobigny Cedex, France. E-mail: [email protected]
This article has an online supplement, which is accessible from this issue’s table
Subjects
Twelve male normal subjects (aged 29 Ϯ 6 years) participated in the
Am J Respir Crit Care Med Vol 171. pp 275–281, 2005 Originally Published in Press as DOI: 10.1164/rccm.200406-804OC on October 29, 2004
study. Anthropometric characteristics were as follows: height 181 Ϯ
Internet address: www.atsjournals.org
6 cm, body weight 79 Ϯ 11 kg. They were healthy, unacclimatized to
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
altitude, moderately trained subjects, with no particular medical history,
Vansbro, Sweden) until exhaustion, at Days Ϫ3, 2, 5, and 8. ECG was
and no previous episode of severe altitude sickness. They gave their
monitored continuously (Life Scope 6; Nihon Kohden, Tokyo, Japan)
informed consent to participate in the study, which was approved by
and arterial O2 saturation was obtained by ear oximetry (Ohmeda Biox
the Ethics Committee of Necker Hospital, Paris.
3740) on an ear lobe previously vasodilated by a capsaicin cream. PaO ,
PaCO , and pHa were measured by means of a blood gas apparatus
Procedure
(Model 220; Bayer Diagnostics, Leverkusen, Germany) from an arteri-
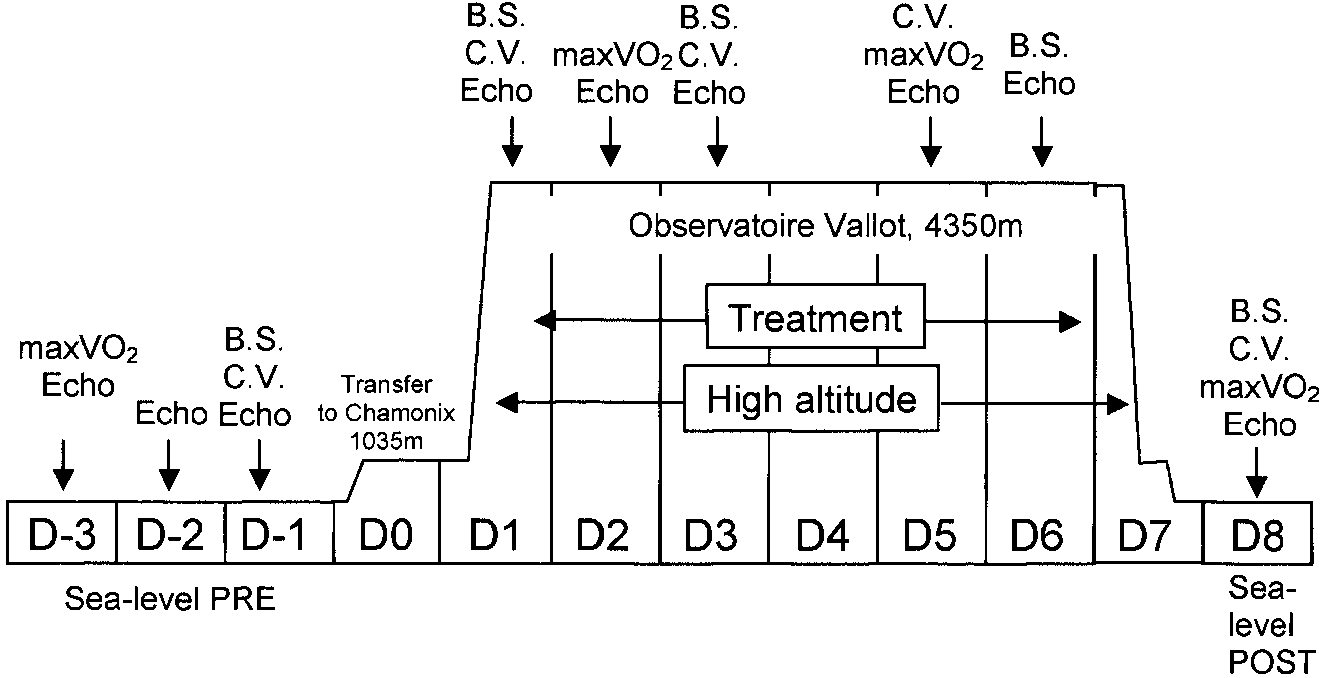
The following evaluations were performed during the 11-day experi-
alized blood sample. Cardiac output and an intrathoracic fluid index
mental period from Days Ϫ3 to 8 (Figure 1). Sea-level Petit-Ebersviller
were measured continuously by transthoracic impedencemetry (Physi-
measurements were performed in Bobigny (60-m altitude); then sub-
oflow PF-05 lab1; Manatec, France), from electrodes placed on the base
jects were transported to Chamonix (1,035 m) for 1 day and to Observa-
of the neck and on the medial line under the xyphoid (24, 25).
toire Vallot (4,350 m) by helicopter (21). Additional details on the
Color Vision Test
methods and equipment used are provided in an online data supple-ment.
Modifications in color vision in the red-green axis have been observedat high altitude and correlated with severity of AMS (26). Transient,
Clinical Questionnaire and Systemic
fully reversible, impairment of color discrimination has also been no-
Hemodynamic Parameters
ticed as a side effect of treatment with sildenafil (27). Color vision wasevaluated in the present study, using the Lanthony 15-Hue Desaturated
A daily questionnaire was filled three times a day (8:00–9:00 a.m.,
Test at Days Ϫ1, 3, 5, and 8. A color confusion index was calculated.
1:00–2:00 p.m., and 6:00–7:00 p.m.), including the Lake Louise consensus
The greater the number and importance of mistakes, the higher the
questionnaire, to evaluate the symptoms of AMS (22), and some specific
questions related to the possible adverse effects of sildenafil (headache,muscle pain, dyspepsia, flushing). A score of sleep disturbances was
Cyclic Guanosine Monophosphate and Sildenafil
evaluated in the morning (from 0, normal sleep, to 3, very poor sleep).
Blood sampling was performed at rest from an antecubital vein at Days
Ataxia and dyspnea were also evaluated (from 0 to 3) according to the
Ϫ1, 3, 6, and 8 to measure cyclic guanosine monophosphate (cGMP),
Lake Louise consensus (22). At the same moment, heart rate and O2
sildenafil concentration, and hematocrit, 1 to 2 hours after oral adminis-
saturation were evaluated by pulse oximetry (Ohmeda Biox 3740; Medical
tration. cGMP was measured by radioimmunoassay (cGMP RIA kit;
Supplies & Equipment Co.), and systemic systolic and diastolic blood
Immunotech, Marseille, France). Sildenafil plus desmethylsildenafil
pressure were evaluated in a supine position by sphygmomanometry.
concentration was measured by a liquid chromatography–tandem mass
Echocardiography
spectrometry method (29). Hematocrit was measured immediately bymeans of a microcentrifuge (Sigma 112, Osterode-am-Harz, Germany).
Subjects were examined by two observers on left decubitus or supineposition, using a portable ultrasound system equipped with a 2.5-MHz
Treatment
probe (Cypress; Acuson/Siemens, Erlangen, Germany). Complete two-
Subjects were randomly assigned to a placebo- (PLA, n ϭ 6) or silden-
dimensional, time movement (TM)-echography and Doppler parame-
afil- (SIL, n ϭ 6) treated group. Treatment (40 mg) started on Day 1
ters for left cardiac function were recorded following classical proce-
at 4,350 m at 8:00 p.m., 6 to 8 hours after arrival at Observatoire Vallot.
dures. Systolic pulmonary arterial pressure (sPpa) was calculated from
Treatment then was taken (40 mg orally) three times a day (8:00 a.m.,
the tricuspid gradient. The acceleration time of the pulmonary flow
2:00 p.m., and 8:00 p.m.) from Days 2 to 6. Sildenafil and placebo were
was taken as an index of pulmonary vascular resistance (23). At each
examination, all parameters were measured at least three consecutivetimes and the subjects were examined three times on baseline on Days
Statistics
Ϫ3, Ϫ2, and Ϫ1; five times during the altitude exposure on Days 1, 2,
Values are presented as mean Ϯ SD. A Mann-Whitney U test was
3, 5, and 6; and at recovery on Day 8 (sea level postexposure). Baseline
performed to compare the two groups and analyze the effects of treat-
normoxic values (sea level preexposure) were taken as the mean of
ment in each condition (symbol #). Values obtained at high altitude
values obtained at Days Ϫ2 and Ϫ1. Values at Days Ϫ2 and Ϫ3 were
after treatment (from Days 2–6) have also been compacted and analyzed
pooled and considered as initial values after 1 to 2 days of treatment;
with a Mann-Whitney U test to evaluate the overall effect of treatment
values at Days 5 and 6 were pooled and considered as final values after
at high altitude (symbol ϩ). A Wilcoxon paired test was used between
each condition and sea level to evaluate the effect of altitude exposureon each group (symbol *). Values of the two groups were pooled at
Maximal Exercise Test
Day 1 to evaluate, by a Wilcoxon paired test, the overall effect of
Maximal aerobic performance was evaluated through a step-by-step
hypoxia before treatment (symbol §). The symbols #, ϩ, *, and § appear in
progressive exercise test performed on a bicycle ergometer (Monark,
tables and figures. A p value less than 0.05 was considered as significant. Figure 1. Schematic
The whole study lasted 12 days, from Day Ϫ3 to Day 8. VO2max ϭ maximal exercise test; Echo ϭ echocardio-graphic examination; B.S. ϭ blood sampling; C.V. ϭcolor vision test; D ϭ day.
Richalet, Gratadour, Robach, et al.: Sildenafil, Pulmonary Hypertension, and Hypoxia
high altitude and was clearly higher in SIL than in PLA fromDays 2 to 6 (p Ͻ 0.001 [Figure 2C]). Tolerance
Exposure to high altitude and treatment were well tolerated by
Echocardiography
all subjects. Subject 4 (PLA) showed some low values of SaO
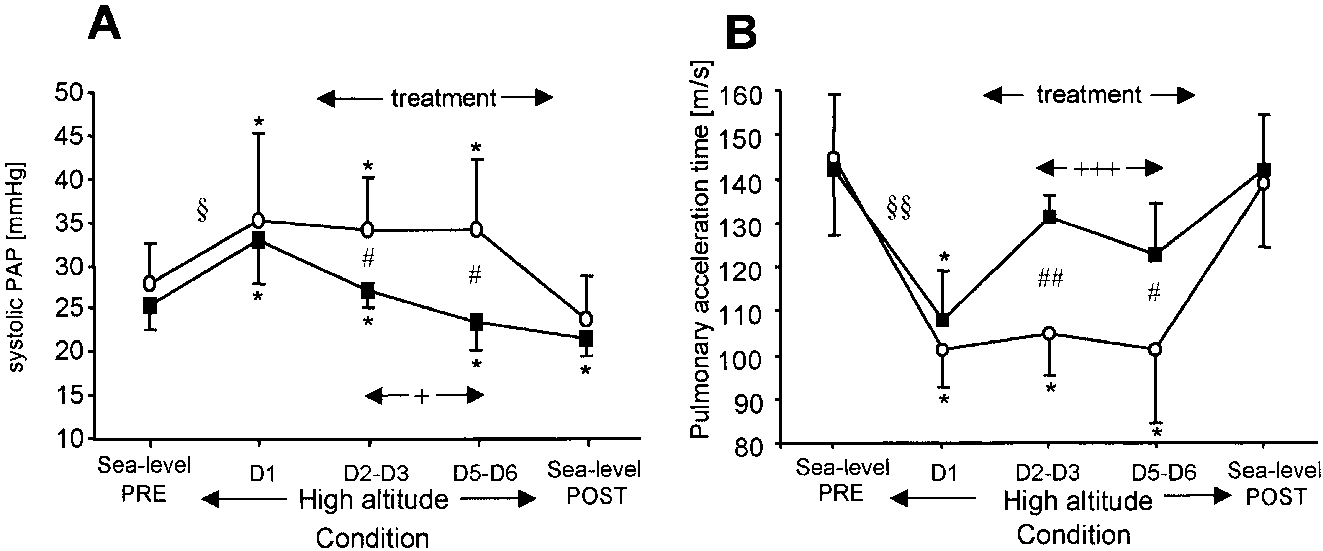
As expected, sPpa increased with acute exposure to high altitude
(under 60%) at various occasions at high altitude, without any
(Day 1) before treatment (Figure 3). After 1 to 2 days of treat-
abnormal clinical symptoms, except moderate headache and fa-
ment (Days 2–3), sPpa was significantly lower in SIL than in
tigue. His cardiac and lung auscultation and neurologic examina-
PLA (p ϭ 0.025). After 4 to 5 days of treatment (Days 5–6),
tion were strictly normal. He was maintained in the study and
sPpa was lower in SIL than in PLA (p Ͻ 0.05). At Days 5 to 6,
given inhaled O2 (1 L/minute) for 4 hours during sleep from
when compared with sea level, sPpa increased by 21% in PLA
Days 4 to 5, at distance from any test involved in the study. It
(p ϭ 0.03) and decreased by 6% in SIL (not significant [NS]).
is noteworthy that the significance of all results presented is not
Pulmonary acceleration time decreased in both groups at Day 1
modified if Subject 4 is excluded from the study. Frequency of
(before treatment) and returned to basal normoxic values in SIL
expected adverse events was not different between the two
but stayed low in PLA at high altitude (p ϭ 0.001, PLA versus
groups: one SIL and two PLA subjects suffered from dyspepsia;
SIL). All other echocardiographic parameters, especially those
three SIL and one PLA subjects showed flushing of the face;
exploring left ventricular function, were strictly normal and simi-
muscle pain was noticed by two SIL and three PLA subjects.
lar in the two groups (Table 2). The diameter of the left ventricle
All these complaints were occasional. Sildenafil treatment had
slightly decreased in diastole and systole, leading to a transient
no effect on color vision. Acute exposure to high altitude (Day 1)
increase in shortening fraction. Left atrium diameter and mitral
was associated with a slight alteration in color vision score in
early to late peak velocity ratio (E/A) progressively decreased
both groups (Day 1 versus sea level pre, p Ͻ 0.05); then values
with exposure to high altitude. Cardiac output measured by
returned to normal levels (Table 1).
Doppler increased from sea level at Day 1 and Days 2 to 3 inboth groups (p Ͻ 0.05), then returned to basal values, with no
Clinical Evaluation
Subjects suffered from AMS until Day 4; then the Lake Louisescore was not significantly different from normoxic baseline. Aerobic Performance and Gas Exchange
Lake Louise score tended to be lower in SIL group at Day 1
As expected, maximal O2 consumption decreased at high altitude
(p ϭ 0.054) before treatment and thereafter at Days 5 and 6,
(Day 2) and slightly (NS) increased with acclimatization (from
but the difference did not reach significance. Among clinical
Days 2–5) (Table 3 and Figure 2). The altitude-induced mean
symptoms, gastrointestinal symptoms and dizziness were similar
decrement in maximal O2 consumption was smaller in SIL (Ϫ29%
in the two groups (results not shown). Headache, which is both
at Day 2, Ϫ25% at Day 5) than in PLA (Ϫ39% at Day 2,
a symptom of AMS and a possible adverse effect of sildenafil,
Ϫ35% at Day 5) (p Ͻ 0.01, SIL versus PLA, Figure 2D). At
was not significantly modified by the treatment. Fatigue score
high altitude, PaO was higher in SIL than in PLA, either at rest
seemed slightly higher in PLA than in SIL, even after the return
(p Ͻ 0.05 at Days 5–6) or at exercise (p Ͻ 0.01 at Days 5–6).
to normoxia, but the differences did not reach significance. Sleep
Alveolar–arterial difference in Po2 at rest and at exercise de-
was significantly altered during the first 2 nights at high altitude,
creased in both groups at high altitude, but the decrease was
with no effect of sildenafil. Only scarce cases of ataxia or dyspnea
lower in PLA than in SIL (p Ͻ 0.001 at rest, p Ͻ 0.05 at exercise).
scores different from zero were noticed, with no effect of silde-
On return to sea level, at rest, PaO was lower and alveolar–
nafil (results not shown) (see Table 1).
arterial difference in Po2 higher than in basal level values. Asexpected, PaCO decreased and pHa increased at high altitude
Systemic Hemodynamic Parameters
(hyperventilation-induced hypocapnia and alkalosis); no differ-
Mean daily heart rate increased in both groups at high altitude
ence was found between the two groups. Cardiac output at rest,
(Figure 2A). Heart rate in SIL was significantly lower than in
measured by transthoracic impedencemetry, transiently in-
PLA from Days 2 to 6 (p Ͻ 0.01). Systolic and diastolic systemic
creased at high altitude (p Ͻ 0.05) and was similar in the two
arterial pressure increased transiently from Days 1 to 4, but was
groups. At ventilatory threshold, cardiac output was modified,
not modified by the treatment (Figure 2B). SaO decreased at
neither by altitude nor by treatment. Heart rate at ventilatory
TABLE 1. CLINICAL SYMPTOMS AND COLOR VISION Definition of abbreviations: a.u. ϭ arbitrary units; D1 to D5 ϭ first to fifth day at 4,350 m; PLA ϭ placebo; sea level post ϭ return to normoxic conditions; sea level
pre ϭ basal normoxic condition; SIL ϭ sildenafil.
* p Ͻ 0.05 versus sea level pre. § p Ͻ 0.05, D1 versus sea level pre for the whole group (placebo ϩ sildenafil). §§ p Ͻ 0.01, D1 versus sea level pre for the whole group (placebo ϩ sildenafil).
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Figure 2. Systemic hemodyna- mic parameters and exercise performance. *p Ͻ 0.05 versus sea level pre; #p Ͻ 0.05, ##p Ͻ 0.01 sildenafil versus placebo; §p Ͻ 0.05, §§p Ͻ 0.01 D1 versus sea level pre for the whole group; ϩϩp Ͻ 0.01, ϩϩϩp Ͻ 0.001 sildenafil versus placebo for pooled high altitude with treatment values.
threshold and at maximal exercise decreased at high altitude in
Serum cGMP, Serum Sildenafil, and Hematocrit
both groups. After the return to sea level, maximal heart rate
Serum cGMP increased from sea level at Day 1 before treatment,
remained lower than before the hypoxic exposure. The intratho-
then by 165% (p Ͻ 0.05) and 42% (NS) at Day 6 in SIL and
racic fluid index increased in both groups at high altitude (Day 2),
PLA, respectively (p Ͻ 0.05 SIL versus PLA) (Figure 4). Serum
then decreased only in SIL and stayed elevated in PLA (p Ͻ 0.05
sildenafil plus desmethylsildenafil concentration was below de-
tectable limit at Day Ϫ1 and Day 1 and increased in the SILgroup to 10.3 Ϯ 6.7 ng/mL and to 254 Ϯ 146.3 ng/mL at Day 2
Acclimatization to High Altitude
(cumulative dose of sildenafil ingested, 36 hours after first pill:160 mg) and Day 6 (cumulative dose of sildenafil ingested, 108
The physiologic parameters, characteristics of acclimatization
hours after first pill: 520 mg), respectively. Hematocrit was not
to high altitude (PaCO , pHa, heart rate), were modified from
modified by the treatment. In the whole group, mean hematocrit
Days 2 to 5 as expected. No difference was found between SIL
increased from 43.2 Ϯ 2.6% at sea level (Day Ϫ1) to 46.1 Ϯ 1.8
and PLA. PaCO at rest and at the ventilatory threshold decreased
at Day 3 (p Ͻ 0.001); 45.3 Ϯ 1.3 at Day 6 (p Ͻ 0.01); and was
from Days 2 to 5 (SIL: p Ͻ 0.03, PLA: NS); pHa at the ventilatory
still high at Day 8 (45.9 Ϯ 2, p Ͻ 0.001).
threshold increased (SIL: p Ͻ 0.03, PLA: NS). Heart rate at theventilatory threshold and at maximal exercise decreased from
DISCUSSION
Days 2 to 5 (p Ͻ 0.05 for PLA and SIL). Sildenafil treatment
This is the first double-blind controlled study evidencing the
had no effect on these parameters (Table 3).
beneficial effect of oral sildenafil (3 ϫ 40 mg/day for 6 days) in
Figure 3. Echocardiographic evaluation of pulmonary hemodynamics. PAP: pulmonary artery pressure. *p Ͻ 0.05 versus sea level pre; #p Ͻ 0.05, ##p Ͻ 0.01 sil- denafil (filled squares) versus placebo (open circles); §p Ͻ 0.05, §§p Ͻ 0.01 D1 versus sea level pre for the whole group; ϩp Ͻ 0.05, ϩϩϩp Ͻ 0.001 sildenafil versus pla- cebo for pooled high altitude with treatment values.
Richalet, Gratadour, Robach, et al.: Sildenafil, Pulmonary Hypertension, and Hypoxia
TABLE 2. ECHOCARDIOGRAPHIC PARAMETERS Definition of abbreviations: D1 to D6 ϭ first to sixth day at 4,350 m; PLA ϭ placebo; sea level post ϭ return to normoxic conditions; sea level pre ϭ basal normoxic
* p Ͻ 0.05 versus sea level. § p Ͻ 0.05, D1 versus sea level pre for the whole group (placebo ϩ sildenafil). §§ p Ͻ 0.01, D1 versus sea level pre for the whole group (placebo ϩ sildenafil).
normal subjects exposed to prolonged high-altitude hypoxia.
in blood oxygenation. No adverse effect, such as systemic hypo-
High-altitude hypoxia induces a specific pulmonary vasoconstric-
tension or alteration in color vision, was noticed. Only minor
tion and an acute sympathetic activation. Hence, after acute
adverse effects (muscle pain, dyspepsia) have been recorded.
exposure to 4,350 m all the subjects exhibited a decrease in SaO
Lastly, sildenafil hampered the hypoxia-induced decrease in ex-
and the expected changes in cardiac hemodynamics with an
ercise performance and did not interfere with acclimatization.
increase in heart rate, cardiac output, and systemic and pulmo-
The effect of sildenafil on Ppa, already observed in humans
nary pressures. Acclimatization then occurred with a decrease
suffering from primary or secondary pulmonary hypertension
in heart rate and an increase in ventilation.
(10–13, 15–18), has been found in normal subjects exposed to
The main observed effect of sildenafil was a suppression of
altitude-induced hypoxia. No adjunct treatment, such as nitric
the hypoxia-induced increase in Ppa, associated with an increase
oxide or epoprostenol, has been used in the present study sug-
TABLE 3. EXERCISE AND GAS EXCHANGE DATA
PaO , mm Hg
PA-PaO , mm Hg
PaCO , mm Hg Definition of abbreviations: ⌬IFT index ϭ variation of intrathoracic fluid from sea level pre; D2, D5 ϭ second and fifth day at
return to normoxic conditions; sea level pre ϭ basal normoxic condition; SIL ϭ sildenafil; Smax exercise ϭ ventilatory threshold.
* p Ͻ 0.05 versus sea level pre. # p Ͻ 0.05, SIL versus PLA. ## p Ͻ 0.01, SIL versus PLA.
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
development of the alveolar edema in HAPE (1, 2). Even innormal subjects, ventilation-perfusion mismatch has been shownto increase at high altitude with increasing Ppa, either by anonuniform pulmonary vasoconstriction or by increasing theinterstitial and perivascular edema (3). By lowering Ppa, silde-nafil could reduce the pulmonary capillary leak and limit thedevelopment of interstitial edema. The observed decrease inintrapulmonary fluid index with sildenafil is in favor of this hy-pothesis. This amelioration of blood oxygenation, in turn, canhave a beneficial effect on pulmonary vasculature, enhancingthe effect of the drug. On return to sea level, all parameterstended to return to sea level basal values. In both groups at rest,
Figure 4. Serum cGMP. *p Ͻ 0.05 versus sea level pre; #p Ͻ 0.05
however, PaO was lower and the alveolar-arterial difference in
sildenafil (filled squares) versus placebo (open circles); §§p Ͻ 0.05 D1
Po2 (a) higher than in basal conditions. This may not be linked
versus sea level pre for the whole group. ϩp Ͻ 0.05 sildenafil versus
placebo for pooled high altitude with treatment values.
related to a slight persistent interstitial edema or ventilation-perfusion mismatch after altitude exposure.
No significant adverse event was evidenced and the treatment
was well tolerated. The dose used (120 mg/day) is comparable
gesting that the inhibition of PDE5 by itself can have a vasodila-
with what is now commonly used (100–150 mg) in prolonged
tory effect on pulmonary circulation, probably by increasing the
treatment of pulmonary hypertension (15, 18). No clear effect
availability of cGMP within the pulmonary vasculature (13). In
has been shown on the clinical signs of AMS, even if a tendency
the present study, plasma level of cGMP increased with sildenafil
to lower the Lake Louise score was shown after 4 days of altitude
and was associated with a decrease in Ppa without significant
exposure. Headache being a possible adverse effect of sildenafil,
decrease in cardiac output. This is in accordance with a direct
however, its probable increase in treated subjects may have
effect of cGMP on pulmonary vascular smooth muscle cell rather
jeopardize a possible beneficial effect on overall AMS score
than an effect on cardiac function. Increase in Ppa at high altitude
because of a better blood oxygenation. The indication of silde-
was also confirmed by the decrease in pulmonary acceleration
nafil in the treatment of HAPE has not been addressed in the
time, as shown at Day 1, which has been considered as an index
present study because none of the subjects suffered from this
of pulmonary hypertension (23). Sildenafil restored this index
severe condition. The beneficial effect on Ppa strongly suggests,
to basal values as soon as in Days 2 to 3, whereas it stayed low
however, that this drug could be highly effective in this condition,
in PLA during the whole stay at high altitude. Although present
without adverse systemic effect, contrary to the classically pro-
at Days 2 to 3, the overall hemodynamic effects of sildenafil on
pulmonary circulation were more marked on Days 5 to 6 when
The beneficial effects of sildenafil on pulmonary circulation and
the plasma concentration of the drug was increased 25-fold.
gas exchange have been sufficient to limit the altitude-induced
All parameters of left ventricular systolic function (Table 3)
decrease in maximal aerobic performance. To the authors’
were not modified by the treatment, confirming that sildenafil has
knowledge, no pharmacologic treatment has been previously
no effect on cardiac contractility and left ventricular afterload.
shown to reduce this disabilitating effect of prolonged high-
Furthermore, sildenafil has been shown to have no or modest
altitude exposure. Sildenafil treatment did not interfere with
effects on systemic vasculature after a single dose of less than
the usual physiologic characteristics of acclimatization to high
100 mg (30). In the present study, sildenafil had no significant
altitude. The decrease in PaCO and increase in pHa indicating
effect on systemic circulation because systemic arterial pressure
a process of ventilatory acclimatization and the decrease in
and cardiac output transiently raised then returned to baseline
maximal heart rate, attributable to a progressive desensitization
values similarly in the two groups. Lastly, despite a lower heart
of cardiac -receptors (33), observed in the present study from
rate in the treated group, cardiac output did not significantly
Days 2 to 5, were not modified by the treatment. Similarly,
change suggesting a lack of negative effect of sildenafil on cardiac
an acute altitude-induced decrease in plasma volume probably
inotropism. The lowering effect on heart rate may be indirect,
accounts for the slight increase in hematocrit, without any sig-
by increasing SaO , or direct through a negative chronotropic
effect by increased cGMP (31). The decrease in E/A ratio, an
Sildenafil, by its vasodilating effect on pulmonary circulation,
index of left ventricular relaxation, observed in the two groups
(1 ) suppresses the altitude-induced pulmonary hypertension; (2 )
with exposure to high altitude was probably caused by a decrease
ameliorates pulmonary hemodynamics and gas exchange, lim-
in left ventricular filling as shown by the associated decrease in
iting the altitude-induced hypoxemia and favoring cardiovascu-
left arterial and systolic and diastolic left ventricular diameters.
lar adaptation to exercise; and (3 ) does not alter the normal
This phenomenon is probably linked to a lower venous return
physiologic processes of acclimatization. Further studies will de-
caused by an altitude-induced decrease in plasma volume pre-
termine if sildenafil can replace calcium blockers in the treatment
viously observed in the same conditions (32). In the present
study, plasma volume was not measured but indirect evidencecan be drawn from the acute increase in hematocrit from 43
Conflict of Interest Statement : J.-P.R. does not have a financial relationship with a commercial entity that has an interest in the subject of this manuscript; P.G.
does not have a financial relationship with a commercial entity that has an interest
in the subject of this manuscript; P.R. does not have a financial relationship with
associated with a lower alveolar-arterial O
a commercial entity that has an interest in the subject of this manuscript; I.P.
does not have a financial relationship with a commercial entity that has an interest
unchanged PaCO , is particularly interesting because it evidences
in the subject of this manuscript; M.D. does not have a financial relationship with
a better oxygen transfer within the lungs, probably because of
a commercial entity that has an interest in the subject of this manuscript; A.J.-L.
a better ventilation-perfusion adequacy or a decrease in lung
does not have a financial relationship with a commercial entity that has an interestin the subject of this manuscript; P.M. does not have a financial relationship with
diffusion impairment. Hypoxia-induced increase in Ppa has been
a commercial entity that has an interest in the subject of this manuscript; J.B.
shown to be one of the main mechanisms responsible for the
does not have a financial relationship with a commercial entity that has an interest
Richalet, Gratadour, Robach, et al.: Sildenafil, Pulmonary Hypertension, and Hypoxia
in the subject of this manuscript; J.C. does not have a financial relationship with
continuous IV epoprostenol in patients with pulmonary arterial hyper-
a commercial entity that has an interest in the subject of this manuscript.
tension. Chest 2003;123:1293–1295.
17. Ghofrani HA, Wiedemann R, Rose F, Schermuly RT, Olschewski H,
Acknowledgment : The authors are grateful to Eric Jaudinot and Ve´ronique
Weissmann N, Gunther A, Walmrath D, Seeger W, Grimminger F.
Chauveau (Pfizer France), Ghazwan Butrous (Pfizer Sandwich) for supporting the
Sildenafil for treatment of lung fibrosis and pulmonary hypertension:
project and providing sildenafil citrate, and Richard Hucker (Pfizer Sandwich) for
a randomised controlled trial. Lancet 2002;360:895–900.
the dosage of sildenafil. The authors thank all the volunteers for their participation
18. Ghofrani HA, Schermuly RT, Rose F, Wiedemann R, Kohstall MG,
in this study at Observatoire Vallot, the Laboratoire de Glaciologie et Ge´ophysiquede l’Environnement for the use of the facilities, Acuson/Siemens for providing the
Kreckel A, Olschewski H, Weissmann N, Enke B, Ghofrani S, et al.
echocardiographic device (Cypress), and Bayer Diagnostics for providing the
Sildenafil for long-term treatment of nonoperable chronic thromboem-
bolic pulmonary hypertension. Am J Respir Crit Care Med 2003;167:1139–1141.
19. Richalet J-P, Gratadour P, Pham I, Robach P, Joncquiert-Latarjet A. References
Sildenafil inhibits the altitude-induced pulmonary hypertension: a
1. Richalet J-P. High-altitude pulmonary oedema: still a place for contro-
double-blind placebo-controlled study [abstract]. Am J Respir Crit
versy? Thorax 1995;50:923–929.
2. Hackett PH, Roach RC. High-altitude illness. N Engl J Med 2001;345:
20. Richalet J-P, Robach P, Gratadour P, Pham I, Mollard P, Cornolo J,
Brugniaux J, Joncquiert-Latarjet A. Effects of sildenafil on pulmonary
3. Wagner PD, Sutton JR, Reeves JT, Cymerman A, Groves BM, Malconian
artery pressure and gas exchange at high altitude [abstract]. High AltMed Biol 2004;5:257.
MK. Operation Everest II: pulmonary gas exchange during a simulated
21. Richalet J-P. The Scientific Observatories on Mont Blanc. High Alt Med
ascent of Mt. Everest. J Appl Physiol 1987;63:2348–2359.
4. Richalet J-P, Herry J-P. Me´decine de l’alpinisme. Paris: Masson; 2003.
22. The Lake Louise Consensus on The Definition and Quantification of
5. Cerretelli P. Energy sources for muscular exercise. Int J Sports Med
Altitude Illness. In: Sutton JR, Coates G, Houston CS, editors. Hyp-
oxia and mountain medicine. Burlington, VA: Queen City Printers;
6. Oelz O, Ritter M, Jenni R, Maggiorini M, Waber U, Vock P, Ba¨rtsch P.
Nifedipine for high altitude pulmonary edema. Lancet 1989;8674:1241–
23. Tramarin R, Torbicki A, Marchandise B, Laaban JP, Morpurgo M.
Doppler echocardiographic evaluation of pulmonary artery pressure
7. Ba¨rtsch P, Maggiorini M, Ritter M, Noti C, Vock P, Oelz O. Prevention
in chronic obstructive pulmonary disease. A European multicentre
of high-altitude pulmonary edema by nifedipine. N Engl J Med 1991;
study. Working Group on Noninvasive Evaluation of Pulmonary
Artery Pressure. European Office of the World Health Organization,
8. Scherrer U, Vollenweider L, Delabays A, Savcic M, Eichenberger U,
Copenhagen. Eur Heart J 1991;12:103–111.
Kleger GR, Fikrle A, Ballmer PE, Nicod P, Bartsch P. Inhaled nitric
24. Yung GL, Fedullo PF, Kinninger K, Johnson W, Channick RN. Compari-
oxide for high-altitude pulmonary edema. N Engl J Med 1996;334:
son of impedence cardiography to direct Fick and thermodilution
cardiac output determination in pulmonary hypertension. Congest
9. Schneider J-C, Blazy I, De´chaux M, Rabier D, Mason NP, Richalet J-P.
Response of nitric oxide pathway to l-arginine infusion at the altitude
25. Richard R, Lonsdorfer-Wolf E, Charloux A, Doutreleau S, Buchheit
M, Oswald-Mammosser M. Non-invasive cardiac output evaluation
of 4,350 m. Eur Respir J 2001;18:286–292.
during a maximal progressive exercise test, using a new impedance
10. Atz AM, Wessel DL. Sildenafil ameliorates effects of inhaled nitric oxide
cardiograph device. Eur J Appl Physiol 2001;85:202–207.
withdrawal. Anesthesiology 1999;91:307–310.
26. Richalet J-P, Rutgers V, Bouchet P, Rymer J-C, Ke´rome`s A, Duval-
11. Prasad S, Wilkinson J, Gatzoulis MA. Sildenafil in primary pulmonary
Arnould G, Rathat C. Diurnal variations of acute mountain sickness,
hypertension. N Engl J Med 2000;343:1342.
colour vision and plasma cortisol and ACTH at high altitude. Aviat
12. Wilkens H, Guth A, Ko¨nig J, Forestier N, Cremers B, Hennen B, Bo¨hm
Space Environ Med 1989;60:105–111.
M, Sybrecht GW. Effect of inhaled iloprost plus oral sildenafil in
27. Laties AM, Fraunfelder FT. Ocular safety of Viagra (sildenafil citrate).
patients with primary pulmonary hypertension. Circulation 2001;104:
Trans Am Ophthal Soc 1999;97:115–125.
28. Bowman KJ. A method for quantitative scoring of the Farnsworth Panel
13. Zhao L, Mason NA, Morrell NW, Kojonazarov B, Sadykov A, Maripov
D-15. Acta Ophthalmol 1982;60:907–916.
A, Mirrakhimov MM, Aldashev A, Wilkins MR. Sildenafil inhibits
29. Eerkes A, Addison T, Naidong W. Simultaneous assay of sildenafil and
hypoxia-induced pulmonary hypertension. Circulation 2001;104:424–
desmethylsildenafil in human plasma using liquid chromatography-
tandem mass spectrometry on silica column with aqueous-organic
14. Ghofrani HA, Reichenberger F, Kohstall MG, Mrosek EH, Seeger T,
mobile phase. J Chromatogr B 2002;768:277–284.
Olschewski H, Seeger W, Grimminger F. Sildenafil increased exercise
30. Zusman RM, Morales A, Glasser DB, Osterloh IH. Overall cardiovascu-
lar profile of sildenafil citrate. Am J Cardiol 1999;83:35C–44C.
capacity during hypoxia at low altitudes and at Mount Everest base
31. Choate JK, Paterson DJ. Nitric oxide inhibits the positive chronotropic
camp: a randomized, double-blind, placebo-controlled crossover trial.
and inotropic responses to sympathetic nerve stimulation in the
Ann Intern Med 2004;141:169–177.
isolated guinea-pig atria. J Auton Nerv Syst 1999;75:100–108.
15. Michelakis ED, Tymchak W, Noga M, Webster L, Wu XC, Lien D, Wang
32. Robach P, Lafforgue E, Olsen NV, De´chaux M, Bouqueray B, Westerterp-
SH, Modry D, Archer SL. Long-term treatment with oral sildenafil is
Plantenga M, Westerterp K, Richalet J-P. Recovery of plasma volume
safe and improves functional capacity and hemodynamics in patients
after 1 week of exposure at 4,350 m. Pflugers Arch 2002;444:821–828.
with pulmonary arterial hypertension. Circulation 2003;108:2066–2069.
33. Richalet J-P. The heart and adrenergic system in hypoxia. In: Sutton JR,
16. Stiebellehner L, Petkov V, Vonbank K, Funk G, Schenk P, Ziesche R,
Coates G, Remmers JE, editors. Hypoxia: the adaptations. Toronto:
Block L-H. Long-term treatment with oral sildenafil in addition to
A PUBLICATION OF THE AMERICAN ASSOCIATION OF COMMUNITY PSYCHIATRISTS www.communitypsychiatry.org Community Psychiatrist behavioral healthcare must be closely coordinated and that preventive care is important, even as far back as early childhood. These elements could improve the efficiency with which providers use their time. Access would improve, permitting phased-in Medicaid eligib
Note: This review article was published in Theoria 73 (2007) but (due to editing error) without endnotes. Page numbers here as in published text. Kalle Grill, Royal Institute of Technology, Stockholm Department of Philosophy and the History of Technology You come home Friday night all stressed out after a hard day’s work. Nothing is planned for Saturday morning and you don’t feel like soc
 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
altitude, moderately trained subjects, with no particular medical history,
Vansbro, Sweden) until exhaustion, at Days Ϫ3, 2, 5, and 8. ECG was
and no previous episode of severe altitude sickness. They gave their
monitored continuously (Life Scope 6; Nihon Kohden, Tokyo, Japan)
informed consent to participate in the study, which was approved by
and arterial O2 saturation was obtained by ear oximetry (Ohmeda Biox
the Ethics Committee of Necker Hospital, Paris.
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
altitude, moderately trained subjects, with no particular medical history,
Vansbro, Sweden) until exhaustion, at Days Ϫ3, 2, 5, and 8. ECG was
and no previous episode of severe altitude sickness. They gave their
monitored continuously (Life Scope 6; Nihon Kohden, Tokyo, Japan)
informed consent to participate in the study, which was approved by
and arterial O2 saturation was obtained by ear oximetry (Ohmeda Biox
the Ethics Committee of Necker Hospital, Paris.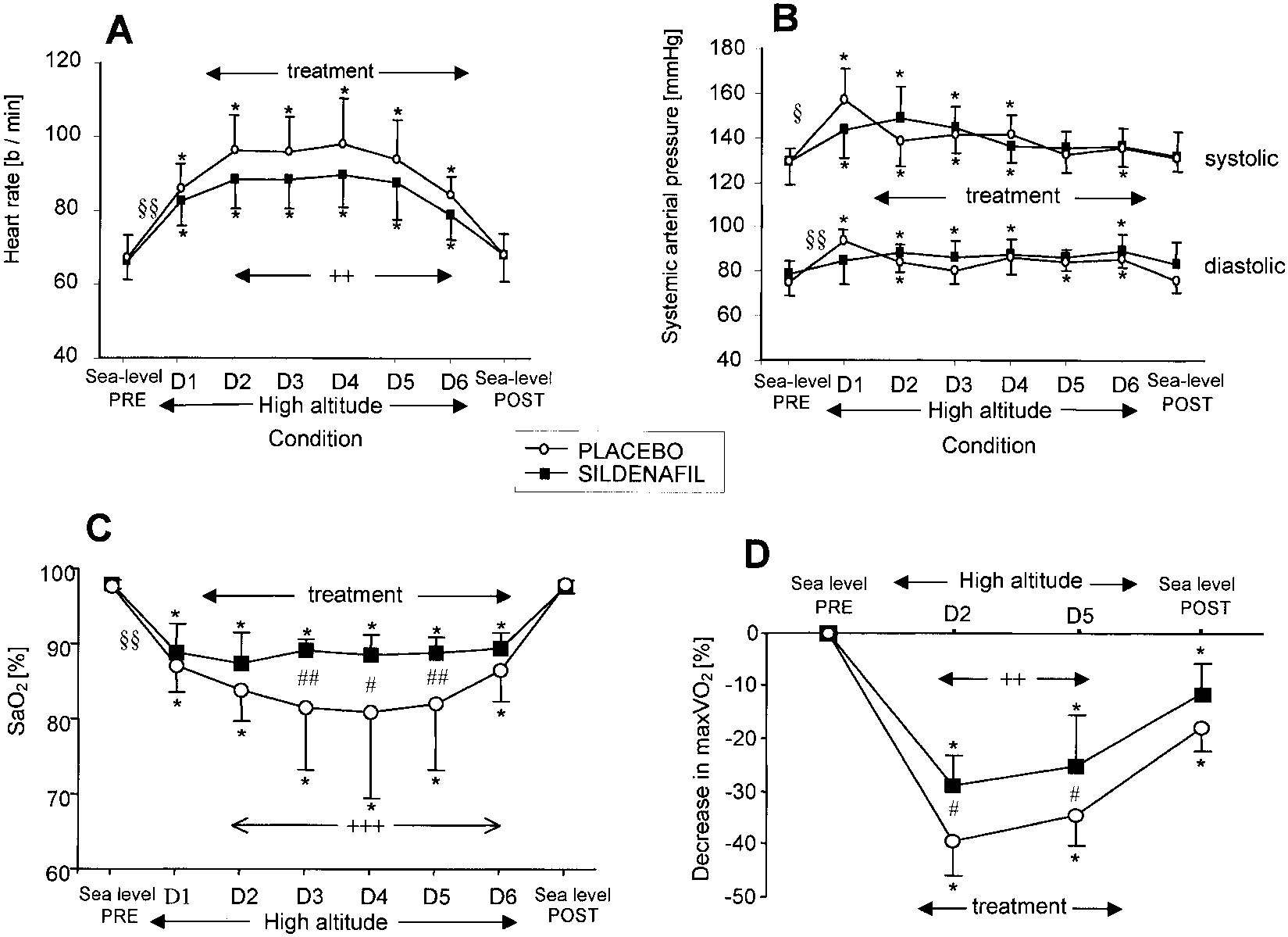
 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Figure 2. Systemic hemodyna-
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Figure 2. Systemic hemodyna-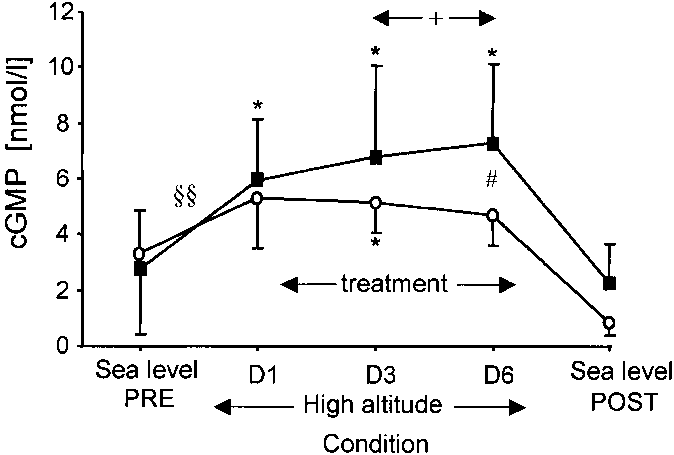 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
development of the alveolar edema in HAPE (1, 2). Even innormal subjects, ventilation-perfusion mismatch has been shownto increase at high altitude with increasing Ppa, either by anonuniform pulmonary vasoconstriction or by increasing theinterstitial and perivascular edema (3). By lowering Ppa, silde-nafil could reduce the pulmonary capillary leak and limit thedevelopment of interstitial edema. The observed decrease inintrapulmonary fluid index with sildenafil is in favor of this hy-pothesis. This amelioration of blood oxygenation, in turn, canhave a beneficial effect on pulmonary vasculature, enhancingthe effect of the drug. On return to sea level, all parameterstended to return to sea level basal values. In both groups at rest,
Figure 4. Serum cGMP. *p Ͻ 0.05 versus sea level pre; #p Ͻ 0.05
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
development of the alveolar edema in HAPE (1, 2). Even innormal subjects, ventilation-perfusion mismatch has been shownto increase at high altitude with increasing Ppa, either by anonuniform pulmonary vasoconstriction or by increasing theinterstitial and perivascular edema (3). By lowering Ppa, silde-nafil could reduce the pulmonary capillary leak and limit thedevelopment of interstitial edema. The observed decrease inintrapulmonary fluid index with sildenafil is in favor of this hy-pothesis. This amelioration of blood oxygenation, in turn, canhave a beneficial effect on pulmonary vasculature, enhancingthe effect of the drug. On return to sea level, all parameterstended to return to sea level basal values. In both groups at rest,
Figure 4. Serum cGMP. *p Ͻ 0.05 versus sea level pre; #p Ͻ 0.05