Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Cybertherapy.info
GIUSEPPE RIVA, BRENDA K. WIEDERHOLD, ENRICO MOLINARI (Eds.)Virtual Environments in Clinical Psychology and Neuroscience1998 Ios Press: Amsterdam, Netherlands. GAIT AND PARKINSONÕS DISEASE: A CONCEPTUAL MODEL FOR AN AUGMENTED-REALITY BASED THERAPEUTIC DEVICE Abstract. This chapter presents an augmented-reality based therapeutic device designed to overcome gait problems associated with ParkinsonÕs Disease (PD). A normal model of gait is proposed followed by a model of Parkinsonian gait with the goal of construction of a gait enabling therapeutic device. The fundamental underlying tenet of the model is that vision pathology is responsible for the majority of Parkinsonian gait pathology. The basis for such a claim is the well documented phenomenon known as Kinesia Paradoxa, whereby in the presence of certain so-called visual cues a PD subject can be transformed from a totally immobile, helpless victim of this disease into a near normal walking individual. Several gait-enabling devices are also described. Introduction
The original motivation for this investigation was the desire to construct vision-based
therapeutic devices designed to overcome gait problems associated with ParkinsonÕs Disease(PD). The basis for such an attempt is the well documented phenomenon known as KinesiaParadoxa [1], whereby in the presence of certain so-called visual cues a PD subject can betransformed from a totally immobile, helpless victim of this disease into a near normalwalking individual. An effective vision-based device has indeed been constructed [2,3],although the device needs to be further perfected and refined. In the course of developingsuch a device it quickly became apparent that there was a need for a model of Parkinsoniangait in order to identify and quantify the parameters involved in gait enablement. This model,described below, undergoes constant revision and although it remains essentially unprovenspeculation, it has proven invaluable as a predictive tool of how Parkinsonians react indifferent and novel environments. The ultimate test of any such model is its ability toeffectively define new and better answers. Indeed, as the model evolved, new and differentapproaches to gait enablement were predicted and on construction proved effective. Several ofthese prototypes are described at the end of this chapter. It should also be noted that since thismodel is based on observing the phenomenon rather than neurophysiology, neurologic termshave been redefined with slight yet significant differences [4]. A General Model of Gait
Gait can be thought of as learned motor activity of the lower extremities which when
performed results in movement of the subject in the environment. By varying the variousparameters of gait, (stride length, velocity, heel and toe strike, timing etc.) one can perform aninfinite variety of gaits. Like any other learned information (motor or sensory or cognitive) aparticular gait can be newly learned or overlearned. A newly learned gait exists in short-termmemory. Characteristics of a given environment determine the particular characteristics of anewly learned gait. Once the environment changes, the newly learned gait is no longerneeded and like short-term memory is quickly forgotten and replaced by a different newly
GIUSEPPE RIVA, BRENDA K. WIEDERHOLD, ENRICO MOLINARI (Eds.)Virtual Environments in Clinical Psychology and Neuroscience1998 Ios Press: Amsterdam, Netherlands.
learned gait tailored to new environmental conditions. While the environment does vary, thereare a few environmental conditions that recur repeatedly and are present most of the time. Thisresults in repeated learning of a select few newly learned gaits until the learned information istransformed in the brain into what is termed overlearned information. Overlearned informationdiffers from newly learned information in several important ways. The most importantdistinction is that once initiated, an overlearned motor package can be performedunconsciously or automatically. This allows our conscious attention to be directed to anothertask and is the basis for efficient simultaneous task performance [5]. I would suggest that thisis mediated by the basal ganglia [6] and can be thought of as its evolutionary purpose.
Newly learned gait is defined or cued by the external environment (for example, fording a
stream by stepping on randomly protruding stones) and is ephemeral whereas the overlearnedmotor package is predefined and permanently stored in the brain. An internal cue prompts theperformance of the entire overlearned motor program as a unit but I would suggest that theessential parameter, which triggers this internal cue, is what I call minimal threshold stridelength. For example, if one physically moves the lower extremity of a totally akinetic PDperson beyond the minimal threshold stride length he will be able to complete at least onestep. The following concepts of stride length are, I believe, part of normal gait function.
1) Initiating Stride: a consciously taken stride, which always follows a position where the
feet are separated by less than a threshold stride length stride. The length of the strideis defined by environmental conditions but the stride itself is under conscious control. It is possible to have a series of initiating steps or it is possible to have a singleinitiating step followed by unconscious automatic gait. In the absence of pathology theenvironment determines which option occurs.
2) Threshold Stride Length: the minimal inter-pedal distance required to access automatic
gait. When this minimum is reached the stride serves as a template for access andperformance of automatic gait, which will occur if the environment is compatible withautomatic gait.
3) Sub Threshold Stride Length: a stride where the inter-pedal distance is less than that of
a Threshold Stride Length. A sub-threshold stride length can be as little as no stridelength whatsoever (for example, when one is standing still with feet side by side) tojust slightly less than the threshold stride length. In normal people environmentalconditions, which result in stride lengths, which fall below this minimal threshold,result in externally cued, consciously controlled gait. A conscious, initiating stride willalways follow a sub threshold stride length stride.
To summarize, gait can be performed in two different modes; conscious mode and
unconscious (automatic) mode. Conscious, newly learned gait is externally cued and itsparameters change constantly to adapt to the changing conditions of the environment. Automatic gait is prerecorded or predefined. An externally cued stride serves as a templateand when certain critical parameters match an automatic (overlearned) motor package thatpackage is accessed. Whenever the environment permits we function in the automatic mode (itcan be thought of as the default mode). This allows us to perform more complex tasks byassembling overlearned motor packages. When the environment is incompatible with theautomatic mode we function in the conscious mode and then revert to the automatic modewhen the environment allows it.
Sensory information is required to evaluate the environment and make the determination
that a specific program can be performed under the current environmental conditions. Theappropriate mode (overlearned versus externally cued) is selected as a result of a dynamicinteraction between the environment and the brain. This interaction is mediated via sensoryinformation, which is perceived primarily (but not exclusively) through the sensory organknown as the eye.
The function of sensory information derived from subject - environment interactions is to
acquire information about the external environment (environment based sensory information)and to acquire information about how the environment responds as we interact with it (subjectinduced sensory information). The stimuli resulting in the former originate in the environmentwhile the latter are dependent on the subject for their existence. In regards to motor functionenvironment based sensory information is required to monitor the environment to assess its
GIUSEPPE RIVA, BRENDA K. WIEDERHOLD, ENRICO MOLINARI (Eds.)Virtual Environments in Clinical Psychology and Neuroscience1998 Ios Press: Amsterdam, Netherlands.
compatibility with specific motor activity, i.e. it defines the motor activity. Subject inducedsensory information directly influences the characteristics of the motor activity beingperformed (if possible, what you see is what you get). Thus, the processing of visual data canbe functionally organized into two distinct categories, which have evolved in response to twotypes of visually perceived sensory information.
1) conscious vision (seeing): visually sensed data plus conscious processing. The data
perceived through conscious vision only becomes meaningful after it has beenanalyzed on a higher cognitive level - filtered through the eye of experience. Forexample identifying an object in a room as a chair or recognizing a face.
2) unconscious vision: visually sensed data which does not require conscious
interpretation, it is processed without conscious awareness. Unconscious vision takesplace in the presence of visual data, which is consistent with the motor activity ofwhich it is a consequence (e.g. the apparent motion of the environment as a subjectwalks through it). Non-conforming visual data is the prompt, which results in a shiftfrom unconscious to conscious vision and results in the subject consciously alteringhis motor function to adapt to a perceived change in the environment. A Proposed Model For PD Gait
In PD I would propose that the underlying cause of the majority of gait problems is
impairment in the visual processing of motion data. Specifically, this impairment is aninability to properly process motion, which falls below a certain velocity, and small changesin the velocity of motion i.e. acceleration and deceleration. This may in turn manifest itself as(or be a consequence of) an impairment in depth perception (data which originates at greaterdistances from the observer will appear to exhibit lower velocity optical flow and lower rate ofexpansion) [7,8,9]. This impairment is the underlying pathology of all gait problemsassociated with PD although the presence of what I call the T-factor can make some of thesegait problems even more malignant and will be discussed shortly. This impairment spans arange of gait problems ranging from the dopamine deficient state (e.g. akinesia) to those ofthe fully medicated state (e.g. dyskinesia) [10]. Indeed, I would suggest that akinesia anddyskinesia are manifestations of the same underlying visual pathology. The difference is theformer is being expressed in the absence of dopamine and the latter in the presence ofdopamine. This theory is based on the discovery that visually accelerating optical flow abovea certain minimal threshold can overcome akinesia, festination, freezing and dyskinetic gait. There are numerous ways to create environments where optical flow is accelerated. Forexample walking on a moving sidewalk, roller-skating, bicycling or any of a number of totalimmersion virtual reality scenarios. PD subjects who exhibit ambulatory dyskinesia willfrequently speed up their gait (i.e. accelerate their optical flow) to facilitate the suppression ofdyskinetic gait. Also, note that running overcomes dyskinesia for the same reason. Andfinally walking over regularly spaced objects, the classic scenario described in kinesiaparadoxa, also serves to accelerate optical flow. In fact it is not the ÒobjectnessÓ of walkingover an array of objects which enables gait but rather their role as reference markers on thereal world whose apparent motion serves to augment the visibility of optical flow as we walkover them. This is analogous to watching the dashed lines on a highway Òmove towards usÓas we drive over them thereby enhancing the visibility of optical flow.
When under medicated this visual pathology is perceived as an inability to generate the
required weight-bearing stride length for a particular gait the environment requires at anygiven time. When under medicated the only available externally cued stride length (if any) isthe very small 2-3Ó stride length associated with festinating gait. In order to enable gait whichaccelerates from a standstill to cruising speed one must be able to process optical expansion(the perception that objects appear to enlarge as we approach them) at low velocities andthrough small changes in velocity. Since this ability is compromised in PD, gait initiationproblems occur because stride lengths fall short of the demands of the environment. For thesame reason the self-cueing automatic gait program, (though undamaged) is inaccessible, inspite of the fact that the environment is potentially compatible with its performance. This isbecause conscious stride lengths (if any) do not approach the stride length parameters necessary
GIUSEPPE RIVA, BRENDA K. WIEDERHOLD, ENRICO MOLINARI (Eds.)Virtual Environments in Clinical Psychology and Neuroscience1998 Ios Press: Amsterdam, Netherlands.
to create the template to switch it on. Even if the automatic gait package were accessed, itwould break down because the same pathology exists in the peripheral processing of data [7]which is essential for sustaining the automatic gait package. In the absence of normalperipheral processing peripherally perceived data will seem inconsistent with what the brainwould expect relative to the motor activity it is performing. Thus, the automatic motorprogram cannot be sustained, and the result is the freezing associated with a state ofundermedication.
Consistent with this hypothesis is the observation that activities, which result in accelerated
or augmented optical flow immediately, suppress dyskinesia. Examples include bicycling,skating, skateboarding, skiing (including riding on a chair lift), running and walking on amoving sidewalk. In summary, conscious externally cued gait (e.g. when trying to initiategait) requires the perception of the expansion component of optical flow or augmentedcentrally perceived optical flow of virtual motion. In its absence the result is akinesia.
The PD subject is often thought of as being more dependent than normals on visual
feedback of the self-perception of motion for initiating and sustaining ambulation. I wouldsuggest that this dependency on optical flow is the same in normal and PD subjects. Whatdiffers is the ability to perceive it. Normally, when gait is internally cued we monitor theoptical flow of the environment (virtual motion) visually but below the level of consciousawareness, in a manner similar to the way we can monitor the subtle motion of being in a boaton the ocean i.e. below the level of conscious awareness. (Nevertheless, such sensory inputcan impact on our motor skills - e.g. motion sickness). Freezing is the pathological inability tosustain unconscious, automatic gait in spite of the environment being compatible withautomatic gait and the subjectÕs intention to achieve it. Freezing occurs when there isinsufficient, erroneous, or misinterpreted visual perception of the optical flow generated byambulation. Once frozen the subject is forced to change to an externally cued gait. But veryoften this same pathology manifests itself as an inability to produce an initiating stride ofadequate length to conform to the demands of the environment. This is what I would call gaitinitiation problems which can be defined as the inability to produce an initiating stride ofadequate length to conform to the demands of the environment - a failure to meet oneÕsconscious expectations of stride length. Consider the following analogy. You are stopped at ared light at an intersection on a steep incline. The parked car to your right begins to back up. You ÔseeÕ this peripherally but initially your brain perceives this as apparent (not real) motionand concludes that you are moving forward. The resulting conflict between what the brain ispredicting should happen based on the motor program it is running (foot on the brake) andthe accompanying visual feedback results in a kind of reflexive slamming on the brakes. Thebrain cannot produce motor activity, which is inconsistent with predicted visual feedback. Sustaining unconscious, automatic gait requires the processing of virtual motion (opticalflow) which is generally perceived via peripheral vision. Whenever peripheral optical flowdisappears or appears to disappear freezing results. For example, doorways frequently inducefreezing in PD subjects, but I would argue it is not the doorway but rather the opaque wallsaround the doorway which precipitate freezing by obstructing oneÕs ability to perceive opticalflow.
If one is already in motion and the environment requires a change in velocity the result
would be festination in the presence of a need to decelerate and freezing if acceleration isrequired. Festination occurs whenever we resist an accelerating force imposed on us by theenvironment (for example, going downhill or maneuvering around an obstacle in our path)and our maximum externally cued stride length is on the order of 2 to 3 inches. To stop (i.e. neutralize the force of acceleration, and a center of gravity displaced forward beyond the fallpoint) requires that one take many of these small steps in a very short period of time to avoid afall. If the environment compels one to accelerate, one must elongate oneÕs stride within thesame time interval as previous strides. With only a 2 or 3 inch externally cued stride availablethis becomes an impossible maneuver and results in freezing. Taking a step requires adeliberate forward displacement of oneÕs center of gravity, which puts one in peril of falling. The perceived availability of a subsequent stride of adequate length to catch up to thisdisplaced center of gravity and save us from falling is what gives us the confidence to placeourselves in this unbalanced position. Conversely if one perceives an inability to extend theleg (either far enough or quickly enough) the fear of falling inhibits the attempt at ambulation. Note how getting up from a chair requires a similar displacement of oneÕs center of gravity.
GIUSEPPE RIVA, BRENDA K. WIEDERHOLD, ENRICO MOLINARI (Eds.)Virtual Environments in Clinical Psychology and Neuroscience1998 Ios Press: Amsterdam, Netherlands.
The perceived inability to adequately extend the leg to catch oneself results in consistentundershooting of the forward propulsion needed to get up from the chair (except in thepresence of the weight bearing pathologic tone Ð see ÒT-factorÓ discussion to follow). Akinetic subjects have little difficulty negotiating stairs. Again, this is because walkingup/down stairs is really walking with greatly reduced forward displacement of oneÕs center ofgravity and as a result it is ambulating with minimal stride length (assuming stride length isdefined as the length of a stride in the horizontal axis). Also, walking backwards is oftenpossible when akinetic. This is a consequence of human anatomy. Anatomically, walkingbackwards can take place without posterior displacement of oneÕ s center of gravity.
Motion, both real and virtual, can be perceived centrally or peripherally. Virtual motion can
be perceived without conscious attention and this is the basis by which unattended, automaticgait is sustained. When motion is perceived the brain makes a best guess determination basedon experience (i.e. sensory conditioning) whether that motion is real or virtual. The ability todistinguish these two categories of motion is essential to the normal performance of gait. Under certain circumstances real motion can be perceived as virtual motion or vice versa. Indeed, such perceptive ÒmistakesÓ can be the basis of both gait pathology and therapeuticdevices. Sensory conditioning has taught us which characteristics of perceived motion aremost reliable indicators of whether that perceived motion should be functionally interpreted asreal or virtual motion. Motion perceived as real can define or select a gait motor package. Motion perceived as virtual sustains the performance and influences the quality ofperformance of that motor program. Dyskinetic gait is an example of what happens when thebrain tries to perform an automatic gait package in the presence of impaired perception orprocessing of virtual motion.
The visual perception of self-motion requires the perception of virtual motion to be
perceived. The characteristics of the perception of self-motion (e.g. is the motion fluid ordisjointed) are a visual reflection of the characteristics of the motor program being performed. As long as this reflection is consistent with what experience has conditioned us to expect thenperformance of the motor package is normal. If this visual reflection is at odds with whatexperience has taught us is the appropriate feedback then this conflict must be resolved eitherby adjusting the performance of the motor program to conform to the feedback or if this isphysically impossible the program stops. This is why monitoring the environment through theviewfinder of a video camera with image stabilization technology suppresses dyskineticgait.or plantar tactile feedback). An analogous situation might be the person who is moderatelyintoxicated and insists that his behavior has been unaffected.
In spite of normal motor function the manner in which this perceived motion behaves is
also a function of how it is referenced to the subject. In the absence of pathology apparentmotion of a subject walking at speed is monitored peripherally. In the presence of referencemarkers on the floor, apparent motion can be tracked in the central field of view. Looking atan outstretched hand while walking (head referencing) results in apparent motion whichexhibits constant velocity (the head moves with constant velocity in gait) whereas if one looksat oneÕs feet apparent motion starts, accelerates, decelerates and stops as each foot goesthrough the swing and stance phase of gait. Both behavior patterns, though different, arenormal and expected with normal gait. Deviation from expected behavior of this apparentmotion can be a consequence of many and varied causes (for example, orthopedic problems,alcohol intoxication, environmental forces). This model proposes that in PD there is animpairment in seeing or processing low velocity motion or small changes in velocity ofmotion. If this is the case then one would predict different gait behavior when apparentmotion is head referenced (for example walking while looking at outstretched hands (whereapparent motion velocity is constant) versus walking while looking at ones feet (whereapparent motion varies and motion would be perceived abnormally). Indeed, masking of feetand head referencing apparent motion ameliorates dyskinetic gait.
To this point this discussion has been limited to pathology which is a consequence of a
vision perception/processing impairment. However, as PD progresses disturbances of theautonomic nervous system result in increased muscle tone. This increased tone results in anincrease in contraction in the major flexion muscle groups and is seen as the stooped posturecommon to so many PD people (simian posture). I call this the T-factor (ÒTÓ for increasedtone and tension) whose presence comes and goes as a consequence of the combination of
GIUSEPPE RIVA, BRENDA K. WIEDERHOLD, ENRICO MOLINARI (Eds.)Virtual Environments in Clinical Psychology and Neuroscience1998 Ios Press: Amsterdam, Netherlands.
environment-induced anxiety and disturbances in the dynamic equilibrium of variousneurotransmitters (on/off cycling).
The presence of T-factor seems to be an augmentation of the fight or flight characteristics
of the autonomic nervous system and results in a much more malignant form of akinesia anddyskinesia. When muscles undergo isometric contraction (for example as occurs in the lowerextremities while maintaining a standing posture) the additive result of T factor tone andisometric muscle tone results in rigidity - which together with vision pathology comprise theprinciple components of this more malignant form of akinesia and freezing. If such a subjectassumes a crawling position then his arms will have posture maintaining isometric tone andthe result is rigidity in the upper extremity and an inability to take a ÒstepÓ with oneÕs arm. The cogwheel rigidity test is a manifestation of the effects of T-factor when additional tone isinduced in a non-weight-bearing extremity.
In the absence of T-factor, akinesia and related gait pathology are induced by aberrant
perceptions of the environment. Appropriate visual manipulations of environmental y inducedperceptions can overcome this gait pathology - the PD subject is physical y capable of ambulation. It is the perception of the inability to take a step, which effectively inhibits ambulation. However, in the presence of T-factor the subject becomes physically incapable of advancingthe lower extremity and manipulating vision pathology will be less effective. If however, onecan initiate ambulation it very often can be sustained because the posture maintaining tone oflower extremity muscles is reduced as the extremities cycle through the various phases of gaitthereby reducing one of the two components of tone which contribute to rigidity. Table 1. Key characteristics of the model Vision only T-factor only
One can frequently observe PD subjects overcoming a freeze by momentarily leaning
against a wall. This results in a brief period of reduced weight-bearing - a transient reductionin tone which facilitates ambulation. At subnormal levels of dopamine T- factor results insevere akinesia. While medicated the result is freezing which occurs in performance anxietysituations (trying to get to a ringing phone or crossing a street with approaching traffic).
Table 2. Definition of key terms
1) externally cued gait (conscious walking): gait where the gait parameters are defined by the environment. 2) internally cued gait (automatic, unconscious walking): gait which is pre-programmed or overlearned. 3) freezing: vision-based pathology resulting in the inability to sustain unconscious, automatic gait in spite
of the environment being compatible with automatic gait and the subjectÕs intention to achieve it.
4) gait initiation failure: the inability to produce an initiating stride of adequate length to conform to the
demands of the environment Ð a failure to meet oneÕs conscious expectations of stride length.
5) festination: a pathologic component of conscious gait which results in a stride which is too small to
result in smooth, controlled deceleration in the presence of environmental conditions that require a need todecelerate.
6) conscious cessation of gait: a conscious successful neutralization of a displaced center of gravity can occur
7) falling: festination, which does not catch up to a displaced center of gravity. 8) conscious vision: central field vision (seeing). 9) unconsious vision: peripherally processed motion, perceived without conscious attention10) initiating stride: a consciously taken stride, which always follows a position where the feet are separated
by less than a threshold stride length stride.
11) threshold stride length: the minimal inter-pedal distance required to access automatic gait. 12) sub-threshold stride length: a stride where the inter-pedal distance is less than that of a threshold stride
13) T-factor: pathologically increased muscle tone, an exaggerated response to normal tone inducing stimuli.
GIUSEPPE RIVA, BRENDA K. WIEDERHOLD, ENRICO MOLINARI (Eds.)Virtual Environments in Clinical Psychology and Neuroscience1998 Ios Press: Amsterdam, Netherlands.
Note that T-factor pathology is independent of vision based pathology. It is possible to be
akinetic and freeze in the absence of T-factor i.e. vision pathology alone for example freezingin a doorway. It is also possible to freeze in the absence of vision pathology, i.e. T-factoralone which occurs while ÒonÓ under performance anxiety scenarios. A Brief Discussion of Gait Enabling Devices
The fundamental underlying principle of all gait-enabling devices is their ability to augment
the ÒperceivabilityÓ or velocity of low speed optical flow.
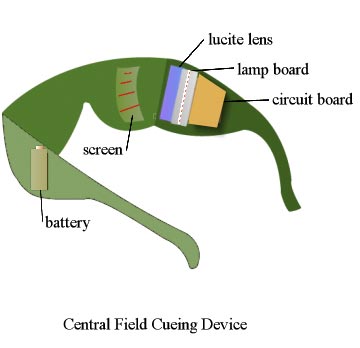
· Central Field Cueing Device (Figure 1): As mentioned above array of objects or
markers linearly arranged on the floor at stride length intervals serve as visual cues andcan enable gait in akinetic Parkinsonians. The Central Field Cueing Device projects thevirtual equivalent of these markers onto the real world without impairing oneÕs abilityto see the real world. This device requires conscious attention and results in conscioustype walking even when the environment is potentially compatible with automaticwalking. However, if the subject is capable of unconscious walking he can learn toignore the virtual visual imagery when the environment allows automatic walking.
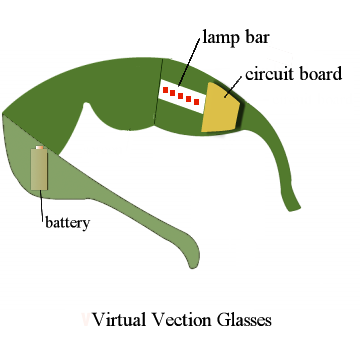
· Virtual Vection Glasses (Figure 2): These glasses provide a scrolling (anterior to
posterior) array of lights at the extreme periphery of the eye. The lights are of coursereal but are interpreted as virtual i.e. apparent motion and provide the subject withfeedback that he is walking. This data is processed below the level of consciousattention Ð only the motion not the objects are ÒseenÓ. It will sustain unconscious gaitbut cannot initiate or sustain conscious gait.
· Elevated Foot Gear: This is a very different technology which is based on the same
principle of augmenting and accelerating optical flow. Vision geometry suggests thatelevating the eyes above their normal height will accelerate optical flow and this canovercome freezing (see Figure 3). The problem with this approach is that the subjectwill eventually functionally adapt to the elevated eye position and then the benefits ofthe approach are lost.
· Auditory/Vibratory Feedback: This is a non-vision mediated approach to gait
enablement and as such does not really address the underlying pathology. However,this approach is useful as a means of sustaining automatic gait by promoting thresholdstride length strides assuming one is functioning in an environment that is compatiblewith automatic gait. The device cannot initiate gait but can facilitate sustainingautomatic gait. The device employs the use of momentary switches in the shoes toprovide auditory or vibratory feedback during the swing phase of gait of eachextremity. Figures 1 and 2: Central field cueing device and virtual vection glasses
GIUSEPPE RIVA, BRENDA K. WIEDERHOLD, ENRICO MOLINARI (Eds.)Virtual Environments in Clinical Psychology and Neuroscience1998 Ios Press: Amsterdam, Netherlands. Figure 3. Optical flow per stride is that segment of the floor, which appears to pass under foot as we advance the foot in gait. Due to vision geometry the optical flow per stride increases as thesubjectÕs eyes elevate relative to the floor. The velocity of the optical flow increases because theincrement of time required to take the stride is unchanged.
All of the above have been clinically tested in unblinded, unscientific, informal trials with
varying degrees of success. There are in fact numerous other approaches to augmenting theperceived or actual velocity of optical flow. Many of these have been built and successfullytested but were abandoned due to the constraints of social acceptability or cost ofdevelopment. All of the devices are in prototype form only and are not currently available tothe general public. However, a modest amount of financial and engineering resources wouldyield great dividends in terms of a useful therapeutic gait-enabling device. Conclusions
In conclusion it is the underlying tenet of this paper that most of the gait pathology
associated with PD is vision-based. Future research should answer such questions as whichparameters of the visual process exhibit this pathology. Is it a perceptive problem of the retina[3,4], and/or a vision-processing problem in the brain? Is there a problem in ÒseeingÓmotion, changes in motion, or depth [1] perception? The entire phenomenon of KinesiaParadoxa has been regarded as a curious anomaly of PD. It should be thoroughly studiedbecause it is an important clue in understanding this phenomenon.
Fundamental research in neurology cannot be overestimated in its importance for finding
solutions to problems of PD and ultimately the cure. However, much can be learned by aphenomenological based investigation, which can potentially provide interim solutions muchmore rapidly. The ultimate test of any such model is its ability to effectively define new andbetter answers to the problems of PD. The concepts expressed in the conceptual modeldescribed above are only now being subjected to scientific scrutiny and it is hoped that suchinvestigation will result in further revision and refinement. These solutions result in improvedquality of life of those currently afflicted with PD and this has been and remains the primaryobjective of these efforts. References
Glickstein, M J. Stein. Paradoxical movement in ParkinsonÕs disease. TINS,14,480-482,1991.
Riess, T., Weghorst, S., Augmented Reality in the Treatment of ParkinsonÕs Disease, InteractiveTechnology and the New Paradigm for Healthcare. IOS Press 1995, 298-302
.Spinney, L. Seeing is Unfreezing. New Scientist, 2/15/97 pp38-40.
Marsden, David C., ParkinsonÕs Disease, Chapter 2. pages 57-98. Chapman and Hall Medical, 1990
Malapani, C., B. Pillon, B. Dubois, Y. Agid. Impaired simultaneous cognitive task performance in
GIUSEPPE RIVA, BRENDA K. WIEDERHOLD, ENRICO MOLINARI (Eds.)Virtual Environments in Clinical Psychology and Neuroscience1998 Ios Press: Amsterdam, Netherlands.
ParkinsonÕ disease: A dopamine-related dysfunction. Neurology, 44:319-326, 1994
Hoover, J., P. Strick, Multiple output channels in the Basal Ganglia. Science, 259,1993
J.P.Harris, J.E. Calvert, O.T. Phillipson. Processing of spatial contrast in peripheral vision inParkinsonÕs disease. Brain, 115(pt5):1447-57, 1992 Oct
Haug, B., Trenkwalder,C., Arden, G., Oertel, Paulus. Visual Thresholds to Low-Contrast,Luminance Contrast Stimuli in ParkinsonÕs Disease. Movement Disorders, vol 9, No.5, 1994 pp563-570
Price MJ Feldman RG Adelberg D. Kayne H. Abnormalities in color vision and contrast sensitivityin ParkinsonsÕ disease. Neurology, 42(4):887-90, 1992
Marsden, David C., and J.D. Parkes, Success and problems in long-term levodopa therapy inParkinsonÕs Disease. Lancet, 12:345-349, 2977
The Bible and the Newspaper: What is Truth? Scripture lessons: John 14:1-6, 18:33-38 For decades, in sermons and articles I've commended to my congregations the instruction of the great theologian Karl Barth, that Christians must live with the Bible in one hand and the newspaper in the other. Only now I learn that he never said that, at least not in so many words. Scholars at the Princeton Th
Doctors Assail Growing Use of Antipsychotic Drugs for Dement. http://www.nytimes.com/2008/06/24/health/24deme.html?page. June 24, 2008 Doctors Say Medication Is Overused in DementiaBy LAURIE TARKAN Correction Appended Ramona Lamascola thought she was losing her 88-year-old mother to dementia. Instead, shewas losing her to overmedication. Last fall her mother, Theresa Lamascola, of the
 GIUSEPPE RIVA, BRENDA K. WIEDERHOLD, ENRICO MOLINARI (Eds.)Virtual Environments in Clinical Psychology and Neuroscience1998 Ios Press: Amsterdam, Netherlands.
GIUSEPPE RIVA, BRENDA K. WIEDERHOLD, ENRICO MOLINARI (Eds.)Virtual Environments in Clinical Psychology and Neuroscience1998 Ios Press: Amsterdam, Netherlands.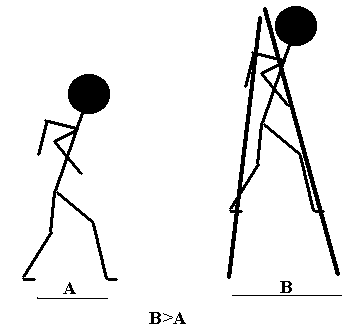 GIUSEPPE RIVA, BRENDA K. WIEDERHOLD, ENRICO MOLINARI (Eds.)Virtual Environments in Clinical Psychology and Neuroscience1998 Ios Press: Amsterdam, Netherlands.
GIUSEPPE RIVA, BRENDA K. WIEDERHOLD, ENRICO MOLINARI (Eds.)Virtual Environments in Clinical Psychology and Neuroscience1998 Ios Press: Amsterdam, Netherlands.