Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Acnr may june 2004.pdf
Involuntary Eye Movement Oscillations
Rhythmic or arrhythmic involuntary sustained to and tegmental pathway of the upward vestibulo-ocular reflex.
fro oscillations of the eyes are classified as either nys-
Multiple sclerosis, tumour, infarction and cerebellar
tagmus or saccadic (rapid conjugate eye movements)
degeneration are the commonest causes9. This type of
oscillations. There is an important distinction between
nystagmus is occasionally suppressed by clonazepam.
them. Saccadic oscillations are initiated by saccadic eye
Torsional nystagmus is a jerk nystagmus around the
movements, whereas in nystagmus the oscillations are ini-
anteroposterior axis. It is commonly associated with other
tiated by smooth eye drifts and the fast phase in jerk nys-
types of nystagmus. However, when it is pure it indicates
tagmus is corrective and not primary (Table 1) (Figure 1).
a lesion of the lateral medulla, involving the vestibular
This short review will describe the commonest types of
nuclei. Occasionally it may be due to a midbrain-thalam-
these ocular oscillations, their causation and manage-
ic lesion, involving the interstitial neucleus of cajal (INC.)
Professor Christopher Kennard is Professor of Gaze-evoked nystagmus is a common clinical observa-
tion with limited localising value. It is a jerk nystagmus
which is absent in the primary position and is only pre-
Faculty of Medicine,Imperial College London
Nystagmus is an oscillation initiated by a slow drift of the
sent on eccentric gaze. It is due to abnormal functioning
eye. This drift may be sinusoidal (pendular nystagmus) or
of the gaze-holding integrator neurons in the paramedian
be followed by a fast corrective (saccadic) eye movement
pontine reticular formation (PPRF) region, resulting
(jerk nystagmus). Although the direction of the nystag-
from impaired inputs from the cerebellar flocculus.
mus is conventionally described by the direction of its
Bilateral horizontal, together with vertical, gaze-evoked
quick phases (for example upbeat nystagmus) it is impor-
nystagmus commonly occurs with structural brainstem
tant to remember that it is the smooth eye movement
and cerebellar lesions, diffuse metabolic disorders and
Centre, Charing CrossHospital, London. He is
imbalance which reflects the underlying disorder (Table
drug intoxication. Treatment is not required since this
2). Nystagmus usually results from a disturbance in one of
type of nystagmus rarely causes severe visual problems.
the three mechanisms which hold gaze still – visual fixa-
Periodic alternating nystagmus (PAN) is a primary
Neurologists. He has aparticular interest in
tion, vestibulo-ocular reflex and the eccentric gaze hold-
position horizontal nystagmus that changes direction
in a crescendo-decrescendo manner, characteristically
The commonest form of jerk nystagmus is peripheral
approximately every 90 sec. Between each directional
the scientific and clinicalliterature on various
vestibular nystagmus, which most frequently results from
change there is a null period of 0 to 10 sec. It is usually
labyrinth or vestibular nerve dysfunction. Tonic vestibu-
associated with lesions affecting the nodulus or uvula of
lar input from the intact side is unopposed by input from
the cerebellum. There is a congenital form10, and acquired
the affected side causing drift of the eyes to that side. This
forms are due to Chiari malformations, multiple sclerosis,
type of nystagmus is usually mixed i.e. various combina-
fourth ventricle tumours, spinocerebellar degenerations
tions of horizontal, vertical and torsional components; it
and anticonvulsant intoxication. Baclofen has been
is always unidirectional, the quick phases beating away
shown to be an effective treatment for the acquired
from the underactive labyrinth; its intensity increases
when the eyes are turned in the direction of the quickphases; it is markedly suppressed by visual fixation (byusing Frenzel goggles); it is usually accompanied by verti-
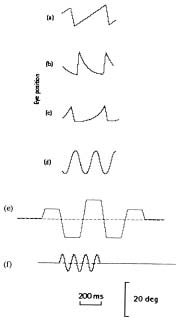
Figure 1. Wave forms and saccadic oscillations of nystagmus. (a)
go, which is of limited duration due to central compensa-
Constant velocity drift of the eyes.
tion. If nystagmus persists for more than a few weeks, it is
usually due to an abnormality of the central vestibular
by peripheral or central vestibulardisease and also with lesions of
pathways. Treatment with diphenhydramine, promet-
hazine, or prochlorperazine is appropriate for relief of the
accompanying nausea and should be stopped as soon as
sawtooth appearance. (b) Drift ofthe eyes back from an eccentric
possible since they can impair the normal compensatory
Several different types of central vestibular nystagmusEye position
are described, all of which show no change in intensity
exponential time-course withdecreasing velocity. This waveform
with the removal of visual fixation in contrast to periph-
eral vestibular nystagmus. Downbeat nystagmus may or
may not be present in the primary position. It beats
impaired neural integrator. (c)Drift of the eyes away from the
directly downwards and is often accentuated in lateral
gaze. When present in the primary position a disturbance
of the vestibulocerebellum, drug intoxication or an
(increasing velocity). Thiswaveform suggests an unstable
abnormality at the cranio-cervical junction, such as a
Type 1 Chiari malformation, are usually found6. These
causes include cerebellar degenerations, anticonvulsant
drugs, lithium intoxication and intra-axial brainstem
vertically in cerebellar disease. (d)Pendular nystagmus, which is
lesions. In about half of the patients with downbeat nys-
tagmus, no cause can be found. Treatment can be
attempted with clonazepam, baclofen, trihexyphenidyl or
acquired disease. (e)Macrosaccadic oscillations:
acetazolomide for the nystagmus associated with episod-
Upbeat nystagmus when present in the primary posi-
flutter: to-and-fro, back-to-backsaccades without an intersaccadic
tion, is usually associated with focal brain-stem lesions in
the tegmental gray matter, either at the pontomesen-
cephalic junction or at the pontomedullary junction,
involving the nucleus prepositus hypoglossi or the ventral
Pendular nystagmus is either congenital or acquired due
Oscillations without any intersaccadic interval (back-
to cerebellar and brainstem disease, usually multiple scle-
to-back) include opsoclonus, ocular flutter and conver-
rosis12. Acquired pendular nystagmus may have both hor-
gence-retraction saccadic pulses. Opsoclonus consists of
izontal and vertical components, and the amplitude and
multidirectional (including oblique and torsional) back-
phase relationships of the two sinewaves determine the
to-back saccades of varying amplitude. It has been sug-
trajectory of the eyes e.g. oblique, circular or elliptical13. It
gested that the disorder arises due to disordered pause cell
can affect one eye or both, equally or unequally, and is
function in the PPRF20. A variety of posterior fossa disor-
often symptomatic resulting in oscillopsia. It may be asso-
ders can give rise to the condition, including parainfec-
ciated with oscillations of other structures such as the
tious brain stem encephalitis, metabolic-toxic states or as
palate, head or limbs14. In some patients gabapentin or
a paraneoplastic (non-metastatic) disorder; in children it
memantine may reduce the amplitude of nystagmus and
is associated with occult neuroblastoma and in adults
with small cell carcinoma of the lung and carcinoma of
Congenital nystagmus is almost invariably a horizontal
the breast and uterus22,23. Both anti-Ri and anti-Hu anti-
conjugate nystagmus, which is unaltered by vertical posi-
bodies have been identified in paraneoplastic opsoclonus
tion. It is generally of jerk type with accelerating slow
in adults. It can also occur in neonates associated with
phases, and has an eccentric null position often leading to
myoclonus - 'dancing eyes and dancing feet.'24 This
a head turn or occasionally a head oscillation16. Fixation
appears to be a maturational deficit which usually
effort enhances congenital nystagmus. Less commonly the
resolves over approximately 6 weeks. Treatment may be
nystagmus is of a pendular type. Reversed optokinetic
with plasmapheresis or intravenous immunoglobulins21
nystagmus, beating in the direction of the target motion,
and drug treatments have included corticosteroids,
is a feature of congenital nystagmus17.
propanolol, verapamil, clonazepam and gabapentin. Latent nystagmus is a type of congenital nystagmus that
Ocular flutter consists of bursts of back-to-back saccades
is only present on monocular viewing and which then
in the horizontal plane only, observed in patients with
beats toward the viewing eye18. It is absent on binocular
multiple sclerosis and signs of cerebellar disease25. It can
viewing. If the patient has amblyopia in one eye latent
also be observed in patients recovering from opsoclonus.
nystagmus is present with both eyes viewing, when it is
A voluntary form of flutter (voluntary flutter) can be
induced by about 8% of the population, usually by con-vergence. It consists of salvoes of horizontal back-to-back
saccades. Lesions of the dorsal midbrain are often associ-
Saccadic oscillations are bursts of saccades, which may be
ated with upward gaze palsies and convergence-retraction
intermittent or continuous, causing a disruption of fixa-
nystagmus (Parinaud’s syndrome). This is incorrectly
tion. Two main types can be identified, those with brief
termed a nystagmus since it actually consists of asynchro-
periods of fixation between saccades (intersaccadic inter-
nous adducting saccades and should be redesignated con-
val approximately 200 msec) and those composed of
vergence-retraction saccadic pulses26. It may alternatively
be due to opposed vergence movements27.
The oscillations with intersaccadic intervals include
square wave oscillations consisting of sequences of
References
square wave jerks (SWJ), which can occur in Alzheimer’s
Kaminski HJ and Leigh RJ. (2002) The neurobiology of eye move-
disease and progressive supranuclear palsy. Macrosaccadicments: from molecules to behaviour. Ann N Y Acad Sci 956: 1-615. oscillations (up to 40 deg) straddle the intended fixation
Leigh RJ and Zee DS. (1999) The neurology of eye movements. New York: Oxford University Press.
position and show a crescendo-decrescendo pattern. This
Buttner U and Fuhry L. (1999) Drug therapy of nystagmus and
type of oscillation is usually observed in acute damage to
saccadic intrusions. Adv Otorhinolaryngol 55: 195-227.
the dorsal cerebellum involving the deep cerebellar
Leigh RJ and Tomsak RL. (2003) Drug treatments for eye move-
nuclei, as in demyelination, tumour or haematoma19. ment disorders. J Neurol Neurosurg Psychiatry 74: 1-4.
Serra A and Leigh RJ. (2002) Diagnostic value of nystagmus: spon-taneous and induced ocular oscillations. J Neurol Neurosurg
Table 1 – Definitions of types of ocular oscillation
Nystagmus – a sustained to and fro oscillation initiated
Halmagyi GM, Rudge P, Gresty MA, and Sanders MD. (1983)
Downbeating nystagmus. A review of 62 cases. Arch Neurol 40:
Saccadic oscillations – sustained oscillations initiated by
Averbuch-Heller L, Tusa RJ, Fuhry L, Rottach KG, Ganser GL,Heide W, Buttner U, and Leigh RJ. (1997) A double-blind con-trolled study of gabapentin and baclofen as treatment for acquirednystagmus. Ann Neurol 41: 818-825. Table 2 - Types of nystagmus and their mechanism Table 3 – Types of saccadic oscillations
Peripheral vestibularCentral vestibular – downbeat, upbeat, torsional,
Convergence-retraction pulses (nystagmus)Ocular bobbing
Barton JJ, Huaman AG, and Sharpe JA. (1994) Muscarinic antag-
18. Gresty MA, Metcalfe T, Timms C, Elston J, Lee J, and Liu C. onists in the treatment of acquired pendular and downbeat nys-
(1992) Neurology of latent nystagmus. Brain 115 ( Pt 5): 1303-
tagmus: a double-blind, randomised trial of three intravenousdrugs. Ann Neurol 35: 319-325.
19. Dell'Osso LF and Daroff RB. Nystagmus and saccadic intrusions
Fisher A, Gresty M, Chambers B, and Rudge P. (1983) Primaryand oscillations. 1999 In: Neuro-ophthalmology (3 ed.), edited
position upbeating nystagmus. A variety of central positional nys-
by Glaser JS. Philadelphia: Lippincott, Williams & Wilkins, 1999,
tagmus. Brain 106 (Pt 4): 949-964.
10. Gradstein L, Reinecke RD, Wizov SS, and Goldstein HP. (1997)
20. Averbuch-Heller L and Remler B. (1996) Opsoclonus. Semin
Congenital periodic alternating nystagmus. Diagnosis andManagement. Ophthalmology 104: 918-928; discussion 928-919.
21. Bataller L, Graus F, Saiz A, and Vilchez JJ. (2001) Clinical out-
11. Halmagyi GM, Rudge P, Gresty MA, Leigh RJ, and Zee DS. come in adult onset idiopathic or paraneoplastic opsoclonus-
(1980) Treatment of periodic alternating nystagmus. Ann Neurol
myoclonus. Brain 124: 437-443.
22. Hersh B, Dalmau J, Dangond F, Gultekin S, Geller E, and Wen
12. Lopez LI, Bronstein AM, Gresty MA, Du Boulay EP, and Rudge
PY. (1994) Paraneoplastic opsoclonus-myoclonus associated with
P. (1996) Clinical and MRI correlates in 27 patients with acquiredanti-Hu antibody. Neurology 44: 1754-1755. pendular nystagmus. Brain 119 (Pt 2): 465-472.
23. Luque FA, Furneaux HM, Ferziger R, Rosenblum MK, Wray SH,
13. Averbuch-Heller L, Zivotofsky AZ, Das VE, DiScenna AO, and
Schold SC, Jr., Glantz MJ, Jaeckle KA, Biran H, Lesser M, and et
Leigh RJ. (1995) Investigations of the pathogenesis of acquiredal. (1991) Anti-Ri: an antibody associated with paraneoplasticpendular nystagmus. Brain 118 ( Pt 2): 369-378. opsoclonus and breast cancer. Ann Neurol 29: 241-251.
14. Schwartz MA, Selhorst JB, Ochs AL, Beck RW, Campbell WW,
24. Hoyt CS, Mousel DK, and Weber AA. (1980) Transient supranu-
Harris JK, Waters B, and Velasco ME. (1986) Oculomasticatoryclear disturbances of gaze in healthy neonates. Am J Ophthalmol
myorhythmia: a unique movement disorder occurring in Whipple'sdisease. Ann Neurol 20: 677-683.
25. Schon F, Hodgson TL, Mort D, and Kennard C. (2001) OcularCorrespondence to:
15. Bandini F, Castello E, Mazzella L, Mancardi GL, and Solaro C. flutter associated with a localised lesion in the paramedian pontine
(2001) Gabapentin but not vigabatrin is effective in the treatmentreticular formation. Ann Neurol 50: 413-416. of acquired nystagmus in multiple sclerosis: How valid is the
26. Ochs AL, Stark L, Hoyt WF, and D'Amico D. (1979) OpposedGABAergic hypothesis? J Neurol Neurosurg Psychiatry 71: 107-
adducting saccades in convergence-retraction nystagmus: a patientwith sylvian aqueduct syndrome. Brain 102: 497-508.
16. Gresty M, Page N, and Barratt H. (1984) The differential diagno-
27. Rambold H, Kompf D, and Helmchen C. (2001) Convergencesis of congenital nystagmus. J Neurol Neurosurg Psychiatry 47:
retraction nystagmus: a disorder of vergence? Ann Neurol 50: 677-
17. Halmagyi GM, Gresty MA, and Leech J. (1980) Reversed optoki-netic nystagmus (OKN): mechanism and clinical significance. Ann
C O N T I N U I N G P R O F E S S I O N A L IFESS 2004 D E V E L O P M E N T PROFESSIONAL DEVELOPMENT IN 9th ANNUAL MEETING INTERNATIONAL FUNCTIONAL EVIDENCE BASED HEALTH CARE ELECTRICAL STIMULATION SOCIETY Three Part-time, Award-Bearing, Postgraduate Courses 'GETTING FES INTO CLINICAL PRACTICE' Certificate, Diploma, MSc in Evidence Based Health Care including a special session on Neuromodulation Next intake starting 20 September 2004 - apply now “I was amazed at the insight into the NHS I gained” “I have found this year inspiring and would recommend it unreservedly” “the invaluable education to be obtained makes well worthwhile the additional
IFESS is the International Functional Electrical Stimulation Society
Short updating skills courses for health professionals:
and this is the first time that the meeting has been held in the UK. NEW for 2004 - Research Skills for Health Professionals
The first 2 days of the conference will be primarily clinical, with the
A series of 1-day courses starting May 10th 2004
second two days looking more closely at the technology behind the
Ethics in Health Care
clinical advances. Delegates will be able to register for just the first
"the quality of the teaching staff was outstanding”
two days or for the whole conference. Systematic Reviews "the teaching was of an exceptional standard and highly enjoyable"
A number of training courses in FES techniques will be held before
Randomised Controlled Trials
the conference on the 4th and 5th of September. See the conference
“a really practical course, very enjoyable, demystifying and well taught”
web site for further details on the conference and training courses. Health Status Measurement “invaluable opportunities to network and learn from other candidates”
End of early registration discount 15 June 2004
Qualitative Research Methods "the imaginative teaching illustrated the processes perfectly"www.ifessnet2004.tk For further details and to book contact Chris Bamford: This meeting is organised by FESnet, the UK FES network,Tel: +44 (0)1865 286941 Fax: +44 (0)1865 286934 [email protected] www.conted.ox.ac.uk/health
http://www.merck.com/includes/print-friendly.html Merck and AstraZeneca Agree to Amend Partnership WHITEHOUSE STATION, N.J., June 27, 2012 – Merck (NYSE: MRK), known as MSD outside theUnited States and Canada, announced today that Merck and AstraZeneca have amended theoption agreement related to their partnership known as AstraZeneca LP (AZLP). The updated agreement provides that AstraZe
Anatomy of a Proactive Password Changer Department of Mathematics and Computer Science 1. Introduction The issue of poor user selection of passwords has been discussed in many papers [6][7] and need not berepeated here. Among the techniques used to overcome these problems are random generation of passwords[3], challenge-response techniques [5], key crunching [4], and the examination of us

 Involuntary Eye Movement Oscillations
Involuntary Eye Movement Oscillations Barton JJ, Huaman AG, and Sharpe JA. (1994) Muscarinic antag-
18. Gresty MA, Metcalfe T, Timms C, Elston J, Lee J, and Liu C.
Barton JJ, Huaman AG, and Sharpe JA. (1994) Muscarinic antag-
18. Gresty MA, Metcalfe T, Timms C, Elston J, Lee J, and Liu C.