COLORECTAL CANCER RESEARCH UPDATES Month Ending May 18th, 2012
The following colorectal cancer research update extends from March 17th, 2012 – May 18th, 2012 inclusive and is intended for informational purposes only.
DRUGS / SYSTEMIC THERAPIES Metformin Provides a Survival Advantage in Patients with Type II Diabetes Effect of Erbitux, Xeloda and Radiotherapy Before Rectal Cancer Surgery Can Aspirin Help Ward Off Recurrence and Metastases? Use of Aspirin Post Diagnosis Improves Survival for Colon Cancer Patients Addition of Erbitux to Chemo as First Line Treatment for Kras Wild Type Metastatic Colorectal Cancer Perifosine Disappoints at Improving Survival Erbitux Plus Xeloda in the First Line Treatment of Advanced Colorectal Cancer in the Elderly Cetuximab After Colon Cancer Surgery Does Not Improve Disease Free Survival Intra-Arterial Infusion of Irinotecan-loaded Drug Eluting Beads (DEBIRI) versus Intravenous Therapy (FOLFIRI) for Hepatic Metastases Research Backs Using Panitumumab (Vectibix) in Colorectal Cancer Patients Deemed to be KRAS Wild Type Oncotype DX Colon Cancer Test Changes Treatment in Close to One Third of Patients Regorafenib Available in the U.S. Via Expanded Access Chemotherapy Using Xeloda Versus 5FU for Locally Advanced Rectal Cancer
SURGICAL THERAPIES Large Bowel Obstruction Can Be Treated Using a Stent RADIOTHERAPY / INTERVENTIONAL RADIOLOGY CT Scans Aid Colon Cancer Treatment PET Evaluation of Treatment Response to Neoadjuvant Therapy in Patients with Locally Advanced Rectal Cancer SCREENING Cutting Out Polyps Cuts Colorectal Cancer Deaths in Half Colon Cancer Awareness Programs Are Helping Pre-Cancerous Polyps May Be Hidden When Bowel Prep Inadequate Prior to Colonoscopy Study Looks at Adherence to CRC Screening Recommendations No Laxative Required for Certain Type of Virtual Colonoscopy Young Colon Cancer Patients Have Challenges with Treatment Costs A New Biomarker That Predicts Colorectal Lesions Choosing the Cancer Tests and Treatments That Are Truly Required GI Tests That Are Truly Required Genes Discovered That Cause Colorectal Cancer Recurrence New Colorectal Cancer Survivorship Program Established at North York General Hospital in Ontario 28. Study Highlights Need for Coordination of Care in Stage II and III Rectal Cancer Treatment NUTRITION / HEALTHY LIFESTYLE Meat Consumption and Colorectal Cancer Risk Obese Patients & Colorectal Cancer Survival Vitamins, Minerals, Essential Fatty Acids and Colorectal Cancer Starchy Foods Cut Bowel Cancer Risk Exercise Might Improve Survival in Colon Cancer Fish Consumption May Prevent Colorectal Cancers DRUGS / SYSTEMIC THERAPIES 1. Metformin Provides a Survival Advantage in Patients with Type II Diabetes (Mar. 25/12)
Patients with type II diabetes mellitus (DM) have an increased risk of colorectal (CR) polyps and CR cancer. The results of this study show that the use of the anti-diabetic agent metformin is associated with a reduced number of cancer-related deaths. Researchers retrospectively evaluated the medical records of 4758 patients seen at a single institution and determined that 424 patients were identified by their physicians as having type II DM and CR cancer. Data were subsequently acquired determining the patient’s age, body mass index (BMI), and disease date of diagnosis, stage, site of cancer, treatment, and survival. Patients with type II DM and CR cancer treated with metformin as one of their diabetic medications had a survival of 76.9 months as compared with 56.9 months in those patients not treated with metformin. Researchers demonstrated that type II diabetic patients treated with metformin had a 30% improvement in overall survival (OS) when compared with diabetic patients treated with other diabetic agents. Researchers concluded that colorectal cancer patients with DM treated with metformin as part of their diabetic therapy appear to have a superior OS. Garrett, CR, et al., Survival advantage observed with the use of metformin in patients with type II diabetes and colorectal cancer. British J of Cancer, 106, pp. 1374-1378 Effect of Erbitux, Xeloda and Radiotherapy Before Rectal Cancer Surgery (Mar.30/12)
The aim of this study was to investigate the efficacy and safety of neoadjuvant (pre-surgical) cetuximab (Erbitux), capecitabine (Xeloda), and radiotherapy for patients with locally advanced rectal cancer. Sixty- three eligible patients were selectively enrolled in this study. Neoadjuvant treatment consisted of cetuximab and capecitabine for 6 weeks and radiotherapy for 5 weeks. Surgical resection was performed 6-8 weeks after the completion of neoadjuvant treatment. KRAS mutation statuses were analyzed retrospectively after the cetuximab treatment. All the patients underwent a standardized postoperative follow-up for at least 3 years. A pathological complete response (pCR) was achieved in eight patients (12.7 %). Overall down-staging was found in 49 patients (77.8 %). The 3-year disease-free survival (DFS) rate and overall survival (OS) rate was 76.2 % and 81.0 %, respectively. The most common adverse events during neoadjuvant treatment were acneiform skin rash (82.5 %), radiodermatitis (46.0 %), and diarrhea (36.5 %). KRAS mutations were detected in 19 of 63 (31.2 %) tumors. The down-staging rate in patients with KRAS wild-type (WT) was significantly higher than patients with KRAS mutation. There was no significant difference in the pCR rate, 3-year DFS rate or 3-year OS rate between KRAS WT patients and KRAS-mutated patients. Investigators concluded that neoadjuvant treatment with cetuximab and capecitabine-based chemoradiotherapy is safe and well tolerated. The pCR rate, 3-year DFS rate and OS rate are not superior to the rate of neoadjuvant chemoradiotherapy using two or more cytotoxic agents. The KRAS WT is highly associated with tumor down-staging to cetuximab plus capecitabine- based chemoradiotherapy in patients with low anterior rectal cancer. Sun, Pei-Long, et al., Effect of neoadjuvant cetuximab, capecitabine, and radiotherapy for locally advanced rectal cancer: results of a phase II study. Internat J of Colorectal Disease. DOI: 10.1007/s00384-012-1446-2 Can Aspirin Help Ward off Recurrence and Metastases? (Mar. 23/12)
Two new studies showed that daily aspirin reduced the risk of dying of cancer by 37% and 46%, respectively. Daily aspirin use also reduced the risk of progressing to metastatic disease, particularly with colorectal cancer. The findings add to a body of evidence suggesting that cheap and widely available aspirin may be a powerful, if overlooked, weapon in the battle against cancer. But the research also poses difficult questions for doctors and public health officials, as regular doses of aspirin can cause gastrointestinal bleeding and other side effects. Past studies have suggested that the drawbacks of daily use may outweigh the benefits, particularly in healthy patients. One of the new studies examined patient data from dozens of large, long-term, randomized controlled trials involving tens of thousands of men and women. Researchers at the University of Oxford found that after three years of daily aspirin use, the risk of developing cancer was reduced by almost 25% when compared with a control group not taking aspirin. After five years, the risk of dying of cancer was reduced by 37% among those taking aspirin. A second paper that analyzed five large, randomized controlled studies in Britain found that over 6 1/2 years on average, daily aspirin use reduced the risk of metastatic cancer by 36% and the risk of adenocarcinomas -- common solid cancers including colon, lung and prostate cancer -- by 46%. Daily aspirin use also reduced the risk of progressing to metastatic disease, particularly in patients with colorectal cancer, the
studies reported. A third paper compared the findings of observational studies and randomized trials of aspirin. The study author maintains there is an urgent need for clinical trials of treatment regimens incorporating aspirin. "What really jumps out at you in terms of prevention is the striking 75% reduction in esophageal cancer and a 40 to 50% reduction in colorectal cancer, which is the most common cancer right now". "In terms of prevention, anyone with a family history would be sensible to take aspirin." But while some experts called the new findings "provocative" and "encouraging," mounting evidence about the preventive promise of aspirin puts health providers in a quandary. Aspirin also increases the risks of gastrointestinal bleeding and hemorrhagic strokes. The new studies, however, also found that the risk of bleeding in aspirin users diminished over time, and that the risk of death from brain bleeds was actually lower in the aspirin users than in the comparison group.
Rothwell, PM, et al., Effect of daily aspirin on risk of cancer metastasis: a study of incident cancers during randomized controlled trials. The Lancet, Vol. 379, Issue 9826: pp. 1591-1601 Rothwell, PM, et al., Effects of regular aspirin on long term cancer incidence and metastasis: a systematic comparison of evidence from observational studies versus randomized trials. The Lancet Oncology, Volume 13, Issue 5, Pages 518 - 527, May 2012 4. Use of Aspirin Post Diagnosis Improves Survival for Colon Cancer Patients (Mar.27/12)
The preventive role of non-steroid anti-inflammatory drugs (NSAIDs) and aspirin, in particular, on colorectal cancer is well established, according to the study authors. More recently, it has been suggested that aspirin may also have a therapeutic role. The aim of the present observational population- based study was to assess the therapeutic effect on overall survival of aspirin/NSAIDs as adjuvant treatment used after the diagnosis of colorectal cancer patients. Data concerning prescriptions were obtained and all patients diagnosed with colorectal cancer (1998–2007) were selected. Aspirin/NSAID use was classified as none, prediagnosis and postdiagnosis and only postdiagnosis. Patients were defined as non-user of aspirin/NSAIDs from the date of diagnosis of the colorectal cancer to the date of first use of aspirin or NSAIDs and user from first use to the end of follow-up. In total, 1176 (26%) patients were non-users, 2086 (47%) were prediagnosis and postdiagnosis users and 1219 (27%) were only postdiagnosis users (total n=4481). Compared with non-users, a survival gain was observed for aspirin users. In rectal cancer, aspirin use was not associated with survival. The NSAIDs use was associated with decreased survival. The study authors concluded that aspirin use initiated or continued after diagnosis of colon cancer is associated with a lower risk of overall mortality. These findings strongly support initiation of a placebo-controlled trial that investigates the role of aspirin as adjuvant treatment in colon cancer patients. Bastiaannet, E., et al., Use of aspirin postdiagnosis improves survival for colon cancer patients. British J of Cancer (2012) 106, pp. 1564-1570 Addition of Erbitux to Chemo as First Line Treatment for kras Wild Type Metastatic Colorectal Cancer (Mar. 27/12)
The previous CRYSTAL and OPUS randomized studies demonstrated that adding cetuximab (better known as Erbitux) to first-line chemotherapy in patients with KRAS wild-type metastatic colorectal cancer (mCRC) significantly improved treatment outcome compared with chemotherapy alone. The objective of this pooled analysis was to further investigate these findings in patients with KRAS wild-type tumours (tumours that do not harbor a genetic mutation in the kras gene) using extended survival data and following an enhancement in the ascertainment rate of KRAS and BRAF tumour mutation status from these studies. Pooled individual patient data from each study were analyzed for overall survival (OS), progression-free survival (PFS – time before the disease got worse) and best overall response rate (ORR) in patients evaluable for KRAS and BRAF mutation status. In 845 patients with KRAS wild-type tumours adding cetuximab to chemotherapy led to a significant improvement in OS and ORR . BRAF mutations (mutations in the BRAF gene) were detected in 70/800 evaluable tumours. No significant differences were found in outcome between the treatment groups in these patients. Prognosis was worse in each treatment arm for patients with BRAF tumour mutations compared with those with BRAF wild-type tumours. The study authors concluded that the analysis of pooled data from the CRYSTAL and OPUS studies confirms the consistency of the benefit obtained across all efficacy end-points from adding cetuximab to first-line chemotherapy in patients with KRAS wild-type mCRC. BRAF mutation does not appear to be a predictive biomarker in this setting, but is a marker of poor prognosis. Bokemeyer, Carsten, et al., Addition of cetuximab to chemotherapy as first line treatment for kras wild type metastatic colorectal cancer: pooled analysis of the crystal and opus randomized clinical trials. European J of Cancer. Published online March 27, 2012. 6. Perifosine Disappoints at Improving Survival (Apr. 2/12)
The results of this study showed that perifosine was no better than a placebo in improving survival time for people with late-stage colorectal cancer. Despite success in a smaller Phase II clinical trial, the X-PECT Phase III trial failed to meet its primary objective — longer survival time. X-PECT randomized 468 patients to receive either:
Xeloda® (capecitabine) plus perifosine, or Xeloda plus a placebo
Although final details were not provided, the perifosine group did not live longer than the patients who received a dummy pill. Patients in the trial had refractory colorectal cancer, tumors that had already gotten worse on at least two standard chemotherapy regimens. Had perifosine helped increase survival time, it would have been a significant new treatment for patients who have exhausted all their standard
treatment options. Based on these results, Keryx, the manufacturer of the drug, will not be pursuing FDA approval for perifosine for refractory colorectal cancer in the U.S.
http://fightcolorectalcancer.org/research_news/2012/04/disappointing_results_for_perifosine
7. Erbitux Plus Xeloda in the First Line Treatment of Advanced Colorectal Cancer in The Elderly
Single-agent cetuximab (better known as Erbitux) is safe and active in elderly patients with advanced colorectal cancer (CRC). A cetuximab–capecitabine combination has not previously been tested in elderly patients with advanced CRC. In this study, sixty-six patients with advanced CRC were treated with cetuximab and capecitabine (better known as xeloda). Thirty-nine additional patients were treated with a reduced dose of capecitabine. The overall response rate was 31.8%. KRAS status was determined in 58 patients (88%). Fourteen of 29 patients with wild-type KRAS tumors responded (48.3%), compared with six of 29 patients with mutant KRAS tumors (20.7%). The median progression-free survival (PFS – time before the disease got worse) interval was 7.1 months. The median PFS interval for patients whose tumors were wild-type KRAS was significantly longer than for those with mutant KRAS tumors (8.4 months versus 6.0 month). The study authors concluded that cetuximab plus capecitabine at a dose of 1,000 mg/m2 every 12 hours may be an alternative to more aggressive regimens in elderly patients with advanced wild-type KRAS CRC.
Sastre, Javier, et al., First line cetuximab plus capecitabine in elderly patients with advanced colorectal cancer: clinical outcome and subgroup analysis according to kras status from a Spanish ttd group study. The Oncologist. March 2012; Vol. 17, No. 3: pp. 339-345 Cetuximab After Colon Cancer Surgery Does Not Improve Disease Free Survival
This study reveals that patients who receive the drug cetuximab (better known as Erbitux) in addition to chemotherapy after undergoing surgery for stage III colon cancer do not have improved disease-free survival (time before the disease got worse). According to the researchers, the chance of cure among patients who undergo surgery for removal of stage III colon cancer is 50%. Several studies have demonstrated the benefit of chemotherapy following surgery in lowering the recurrence risk. For patients suffering metastatic colorectal cancer, cetuximab and panitumumab (Vectibix), alone or in conjunction with chemotherapy, have provided additional benefit than chemotherapy alone. This benefit, however, is limited to patients with tumors expressing the wild-type [a strain used as a standard reference to compare any mutant derivatives] form of the gene KRAS as opposed to those with the mutated form of KRAS.In order to evaluate the potential benefit of cetuximab, in addition to the modified sixth version of the FOLFOX regimen (mFOLFOX6), in individuals with resected stage III wild-type KRAS colon cancer, investigators conducted a study involving 2,686 patients. In this study, 1,863 of the 2,686 patients had wild-type KRAS, 106 patients indeterminate KRAS, and 717 patients mutated KRAS. Participants were randomly assigned to receive either 12 biweekly cycles of mFOLFOX6 with or without cetuximab. Study participants received median follow-up of 28 months. Adding cetuximab provided no benefit, according to results from the study. The researchers found that three-year disease-free survival for patients with wild-type KRAS receiving mFOLFOX6 alone was 74.6%, compared with 71.5% in patients who received mFOLFOX6 in addition to cetuximab, and 67.1% vs. 65.0% in participants with mutated KRAS. The team found no evidence of benefit in any individual subgroup. Furthermore, between treatment groups, no considerable difference was found between overall survival and time-to-recurrence. The team highlight that they are unsure as to why mFOLFOX6 in addition to cetuximab provided no additional benefit. The study authors concluded: “In this randomized phase III trial for patients with resected stage III colon cancer expressing wild-type KRAS mutations, the addition of cetuximab to mFOLFOX6 did not improve disease-free or overall survival in contradistinction to the original study of cetuximab combined with FOLFOX in metastatic colorectal cancer. New approaches are needed to identify drugs that may be of benefit in adjuvant therapy, because as shown in our trial, promising activity in the metastatic setting did not translate into adjuvant therapy benefit and underscores the importance of performing clinical trials." Alberts, Steven, et al., Effect of oxaliplatin, fluorouracil, and leucovorin with or without certuximab on survival among patients with resected stage III colon cancer: a randomized trial. JAMA. 2012; 307(13): pp. 1383-1393 Intra-Arterial Infusion of Irinotecan-loaded Drug Eluting Beads (DEBIRI) versus Intravenous Therapy (Folfiri) for Hepatic Metastases
Metastases to the liver receive most of their blood supply from the arterial route, therefore for patients with hepatic metastases from colorectal cancer, hepatic arterial infusion adopting drug-eluting beads preloaded with irinotecan (DEBIRI) may offer a chance of cure. In a multi-institutional study, 74 patients were randomly assigned to receive DEBIRI versus systemic irinotecan, fluorouracil and leucovorin (FOLFIRI). The primary end-point was survival; secondary end points were response, recurrence, toxicity, quality of life, cost and influence of molecular markers. At 50 months, overall survival was significantly longer for patients treated with DEBIRI than for those treated with FOLFIRI. Median survival was 22 months for DEBIRI and 15 months for FOLFIRI. Progression-free survival was 7 months in the DEBIRI group compared to 4 months in the FOLFIRI group and the difference between groups was statistically significant. Extrahepatic progression had occurred in all patients by the end of the study, at a median time of 13 months in the DEBIRI group compared to 9 months in the FOLFIRI group. The study authors concluded that this study showed a statistically significant difference between DEBIRI and FOLFIRI for overall survival (7 months), progression-free survival (3 months) and quality of life (5
months). In addition, a clinically significant improvement in time to extrahepatic progression (4 months) was observed for DEBIRI, a reversal of the expectation for a regional treatment. This suggests a benefit of DEBIRI treatment over standard chemotherapy and serves to establish the expected difference between these two treatment options for planning future large randomized studies.
Fiorentini, Giammaria, et al., Intra-arterial infusion of irinotecan loaded drug eluting beads (DEBIRI) versus intravenous therapy (folfiri) for hepatic metastases from colorectal cancer: final results of a phase III study. Anticancer Research. April 2012 Vol. 32, no.4: pp. 1387-1395. Research Backs Using Panitumumab (Vectibix) in Colorectal Cancer Patients Deemed to be KRAS Wild Type
The results of this study strongly suggest that panitumumab (better known as vectibix) should be reserved for metastatic colorectal cancer (mCRC) tumors with wild-type KRAS (no genetic mutation in the kras gene). The investigators stated that panitumumab should not be used in tumors with KRAS mutations, even those with specific G12 and G13 mutations previously suggested to confer a favorable response to anti-EGFR therapy like panitumumab. Patients with mCRC tumors that harbor any of the most common codon 12 or 13 mutant KRAS alleles are unlikely to benefit from panitumumab therapy. Currently, only mCRC patients with wild-type KRAS tumors should be treated with EGFR antibodies such as erbitux or vectibix. “In general, patients with mutant tumors do not benefit from EGFR inhibitors. The discussion [about mutations] is still open from a scientific point of view”. “More research is needed.”
Peeters M, et al., Mutant Kras codon 12 and 13 alleles in patients with metastatic colorectal cancer: assessment as prognostic and predictive biomarkers of response to panitumumab. J Clin Oncol. 2012, 30: suppl 4; abstr 383 11. Oncotype DX Colon Cancer Test Changes Treatment in Close to One Third of Patients (Apr. 16/12)
A survey of oncologists suggests that the Oncotype DX colon cancer test changes treatment recommendations for 29% of patients with Stage II colon cancer. These results were presented at the 2012 Gastrointestinal Cancers Symposium. Gene expression profiling explores the patterns of genes that are active in tumor cells. Studies suggest that gene expression may provide important information about prognosis or likely response to treatment in several types of cancer. For example, among selected women with early-stage breast cancer, the Oncotype DX breast cancer test has been shown to predict the likelihood of cancer recurrence and the likelihood of benefit from chemotherapy. As a result, the test has been added to medical guidelines for early-stage breast cancer. A similar test became available for patients with Stage II colon cancer in 2010. Stage II colon cancer refers to cancer that extends through the wall of the colon but has not invaded lymph nodes or spread to distant parts of the body. Many patients with this stage of disease have good outcomes with surgery alone, and routine adjuvant (post-surgery) chemotherapy is not currently recommended for Stage II colon cancer. Chemotherapy may, however, be considered for Stage II patients with a higher risk of cancer recurrence. Previous research has demonstrated that the Oncotype DX colon cancer test provides information about the risk of recurrence among patients with Stage II colon cancer. Researchers are now evaluating how this information affects treatment decisions. In the current study, researchers surveyed US oncologists who had experience with the Oncotype DX colon cancer test. All participating oncologists had ordered the test for at least three patients with Stage II colon cancer, and were asked to provide treatment information for the most recent patient. The study is ongoing, and the current, preliminary analysis includes information from 92 oncologists.
Among the patients who had an initial treatment plan (either chemotherapy or observation), 29% had
a change in recommended treatment after the Oncotype DX test, including changes from chemotherapy to observation and vice-versa.
These results build upon previous studies of the Oncotype DX colon cancer test by demonstrating that use of the test can influence treatment decisions for Stage II colon cancer.
Cartwright T, Chao C, Lopatin M, Bentley T, Broder M, Change E. Effect of Oncotype® DX Colon Cancer Test Results on Treatment Recommendations in Patients with Stage II Colon Cancer: Preliminary Results. Paper presented at: 2012 Gastrointestinal Cancers Symposium; January 19-21, 2012; San Francisco, CA. Abstract 398. Regorafenib Available in the U.S. Via Expanded Access
The first four sites where colorectal cancer patients can get regorafenib in the U.S. are now open. Bayer Healthcare (the manufacturer of the drug) expects to open additional sites in the next two or three weeks. Colorectal cancer patients whose cancer has gotten worse on all standard treatments can now be considered for the Regorafenib Extended Access program. Bayer Healthcare has applied for FDA approval of regorafenib to treat colorectal cancer, but until it is actually approved and on the market, the expanded access program is the only way patients who might benefit can receive it. Last fall, early results from the randomized Phase 3 CORRECT clinical trial showed colorectal cancer patients who received regorafenib lived longer than a similar group who got a placebo. Results of the CORRECT trial were discussed at the 2012 GI Cancers Symposium in January. Axel Grothey, MD and his team concluded: “Statistically significant benefit in overall survival and progression-free survival was observed for regorafenib over placebo in patients with metastatic colorectal cancer who have failed all approved standard therapies. No new or unexpected safety signal was found. Patients in the expanded access
program will get regorafenib pills every day for three weeks, followed by a week’s rest before repeating the treatment cycle.“ The first sites are now open in:
For additional information email [email protected]http://fightcolorectalcancer.org/research_news/2012/04/regorafenib_now_available_via_expanded_access Chemoradiotherapy Using Xeloda versus 5FU for Locally Advanced Rectal Cancer (Apr. 30/12)
Fluorouracil-based chemoradiotherapy is regarded as a standard treatment in locally advanced rectal cancer. Researchers investigated the efficacy and safety of substituting fluorouracil (5FU) with the oral prodrug capecitabine (Xeloda). This randomized, open-label, multicentre, non-inferiority, phase 3 trial began in March, 2002, as an adjuvant trial comparing capecitabine-based chemoradiotherapy with fluorouracil-based chemoradiotherapy, in patients aged 18 years or older with pathological stage II—III locally advanced rectal cancer from 35 German institutions. Patients in the capecitabine group were scheduled to receive two cycles of capecitabine, followed by chemoradiotherapy, then three cycles of capecitabine. Patients in the fluorouracil group received two cycles of bolus fluorouracil, followed by chemoradiotherapy, then two cycles of bolus fluorouracil. The protocol was amended in March, 2005, to allow a neoadjuvant cohort in which patients in the capecitabine group received chemoradiotherapy followed by radical surgery and five cycles of capecitabine and patients in the fluorouracil group received chemoradiotherapy followed by radical surgery and four cycles of bolus fluorouracil. Patients were randomly assigned to treatment group in a 1:1 ratio. The primary endpoint was overall survival. Between March, 2002, and December, 2007, 401 patients were randomly allocated; 392 patients were evaluable (197 in the capecitabine group, 195 in the fluorouracil group), with a median follow-up of 52 months. 5-year overall survival in the capecitabine group was non-inferior to that in the fluorouracil group (76% vs 67%). 3-year disease-free survival was 75% in the capecitabine group and 67% in the fluorouracil group. Similar numbers of patients had local recurrences in each group (12 [6%] in the capecitabine group vs 14 [7%] in the fluorouracil group), but fewer patients developed distant metastases in the capecitabine group (37 [19%] vs 54 [28%]). Investigators concluded that capecitabine could replace fluorouracil in adjuvant or neoadjuvant chemoradiotherapy regimens for patients with locally advanced rectal cancer.
Hofheinz, R, et al., Chemoradiotherapy with capecitabine versus fluorouracil for locally advanced rectal cancer: a randomized, multicentre, non-inferiority, phase III trial. Lancet Oncol. 2012 Apr 13; Epub Ahead of Print. SURGICAL THERAPIES Large Bowel Obstruction Can Be Treated Using a Stent
Cytoreductive surgery (CRS) and intraperitoneal chemotherapy (IPC) treatment of colorectal peritoneal carcinomatosis (PC) is gaining acceptance, but controversy remains, according to the authors of this study. The primary aims of this study were to analyze the outcome of colorectal PC patients treated with CRS and IPC, and to report on the outcome of additional surgical treatments of subsequent recurrences. Patients referred for treatment of colorectal PC between 1996 and 2010 were included in this study. The following data was collected:
perioperative chemotherapy (chemo given before surgery)
type of IPC (hyperthermic intraperitoneal chemotherapy, HIPEC; or sequential postoperative
The median OS was 34 months (range: 2-77) for CRS and HIPEC with five-year survival
predicted at 40% (five-year disease-free survival 32%).
For CRS and SPIC, the OS was 25 months (range: 2-188) with five-year survival at 18%.
OS for patients undergoing additional surgical treatment of recurrences was 25 months vs. 10 months with best supportive care or palliative chemotherapy. The authors concluded that substantial long-term survival is possible in patients with colorectal PC. HIPEC was associated with better OS than SPIC and adjuvant systemic chemotherapy may improve the outcome in patients. Good OS is achievable in selected patients undergoing additional surgical treatment of isolated liver or peritoneal recurrences after prior complete CRS. Cashin, PH, et al., Cytoreductive surgery and intraperitoneal chemotherapy for colorectal peritoneal carcinomatosis: Prognosis and treatment recurrences in a cohort study. RADIOTHERAPY / INTERVENTIONAL RADIOLOGY Radioembolization Shows SIR-Spheres Microspheres Significantly Improves Survival for Liver Mets Patients (Mar. 25/12)
New Australian data provides further evidence of survival benefit for patients undergoing radioembolization. Findings from the largest comparative multi-centre study performed to date using radioembolization report a significantly prolonged survival benefit following SIR-Spheres microspheres in patients who had exhausted all standard therapies (treatment-refractory) for the treatment of their liver tumours originating from colorectal and other cancers. Radioembolization, which is also called Selective Internal Radiation Therapy or SIRT, is a novel approach to treating liver tumours using microspheres labeled with radioactive yttrium-90 (90Y). The microspheres are implanted by interventional radiologists to selectively target the liver tumours with radiation while sparing the remaining healthy liver tissue. SIR-Spheres microspheres deliver millions of microscopic radioactive beads – each about a third of the width of a human hair– directly to the tumor site. Because the microspheres are too large to pass through the small blood vessels within the tumor, they become permanently lodged in the tumor bed, targeting the tumor with a dose of internal radiation up to 40 times higher than conventional radiotherapy, while sparing healthy tissue. The treatment is suitable only for patients with liver tumors and has no effect on tumors outside the liver. Researchers in this study evaluated 463 patients with chemotherapy refractory liver-dominant tumours and found that "radioembolization is associated with a significantly improved and clinically meaningful survival benefit”. Among the 251 patients with colorectal liver metastases, median survival in the 220 patients treated with SIR-Spheres microspheres was 11.6 months, compared to only 6.6 months for the 31 patients who received standard or best supportive care. The significant improvement in overall survival in this study confirm the benefits demonstrated in two previous but smaller comparative studies that were performed in patients with treatment-refractory colorectal liver metastases, notably the multi-centre phase III randomized controlled trial conducted by Hendlisz and colleagues in Belgium, and the matched-pair analysis by Seidensticker and colleagues from Magdeburg, Germany, that reported median survivals of 10.0 and 8.3 months. Two large international randomized controlled trials are currently underway to evaluate the effectiveness of adding radioembolization using SIR-Spheres microspheres to first-line chemotherapy in order to assess whether this treatment should be used as an early intervention in the treatment of patients with colorectal cancer liver metastases. Saxena A, et al. Radioembolization with yttrium-90 microspheres is associated with a significantly improved survival compared to conservative therapy after treatment of unresectable hepatic tumors: A large single center experience of 537 patients. 65th Annual Cancer Symposium of the Society of Surgical Oncology, Asia-Pacific Journal of Clinical Oncology 2012; 7 (Supplement s4): Abstract 212. PET Evaluation of Treatment Response to Neoadjuvant Therapy in Patients with Locally Advanced Rectal Cancer
The purpose of this meta-analysis (review of multiple studies) was to evaluate the utility of positron emission tomography (PET) using fluor-18-deoxyglucose (FDG – radioactive sugar) to predict the response of rectal cancer to neo-adjuvant therapy (therapy administered before surgery). All previously published studies on the role of FDG-PET in predicting the response of rectal cancer to neo-adjuvant therapy were collected. A total of 28 studies, comprising 1204 patients with rectal cancer, were included in the review. Based on the subgroup analyses, there was no significant difference between the response index (RI), the standardized uptake value (SUV) and the visual response score (VRS) in predicting the therapy response. However, the accuracy of the group that underwent PET scanning during therapy showed significantly higher values (sensitivity 86% and specificity 80%) than the group that was scanned after completion of the therapy. Therefore, FDG- PET is valuable for predicting the response of rectal carcinoma to neo-adjuvant therapy, and early evaluation of response during the therapy may be more promising. However, the authors note that additional studies using prospective clinical trials will be required to assess the clinical benefit of this strategy.
Zhang, Chenpeng, et al., 18F-FDG-PET evaluation of treatment response to neo-adjuvant therapy in patients with locally advanced rectal cancer: a meta-analysis. Inter J of Cancer. Online print. SCREENING Cutting Out Polyps Cuts Colorectal Cancer Deaths in Half
The results of this study concluded that colonoscopy reduces death from colorectal cancer.
A Colon Polyp Snared and Gone
In a follow up analysis from the National Polyp Study, people who had adenomas — the risky kind of polyps — removed during the study were much less likely to die from colon or rectal cancer than the general US population. In fact, removing adenomas cut the death rate from colorectal cancer in half. Colonoscopies find and remove precancerous polyps and reduce the number of new colorectal cancers, but this is the first study to actually link colonoscopy to cutting back death from colorectal cancer. There was also good news in the study for people who didn’t have adenomas. They had a very low risk of colorectal cancer death. Only one person out of nearly 800 with no adenomas found at the initial exam died of colorectal cancer. Between 1980 and 1990, the National Polyp Study (NPS) enrolled patients who were having a colonoscopy to rule out colorectal cancer due to symptoms or positive finding on another test. All polyps were removed during the exam. Patients with adenomas had another colonoscopy 1 or 3 years later and again at 6 years. Patients with no polyps or only benign hyperplastic ones had no further testing. For this long-term follow-up study, researchers used the National Death Index to find those patients in the NPS who died from colorectal cancer. The researchers used the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) registry to figure out how many colorectal cancers could be expected in a group of people with the same age, race, and sex of the NPS participants. Comparing 2602 NPS adenoma patients to what was expected in the general population there were:
Overall, 12 deaths in the NPS group compared to an expected 25.4. In less than 10 years, 4 NPS deaths compared to an expected 9.1. For more than 10 years, 8 NPS deaths compared to 16.3
In the follow-up study, 2602 patients had adenomas found during their initial colonoscopy, another 773 didn’t. About a third of the people in the control group did have polyps. But they were the safer hyperplastic type. Only one person in that group of 773 died of colorectal cancer. She died about 8 years after her initial colonoscopy. Researchers concluded that these findings support the hypothesis that colonoscopic removal of adenomatous polyps prevents death from colorectal cancer.
Zauber, Ann G, et al., Colonoscopic Polypectomy and Long-Term Prevention of Colorectal-Cancer Deaths. New England J of Med. Feb. 23, 2012. http://fightcolorectalcancer.org/research_news/2012/03/cutting_out_polyps_cuts_colorectal_cancer_deaths_in_half Colon Cancer Awareness Programs Are Helping
Efforts to educate the public on the importance of lab testing for colorectal cancer may be starting to pay off, as a new study has shown that individuals with more health problems are more likely to be screened. The researchers took the finding as a sign that more doctors are explaining why colorectal cancer screening is so important. For the study, researchers from the University of Kentucky surveyed nearly 1,200 adults between the ages of 50 and 75. The results showed that individuals who had other conditions, such as diabetes, heart disease or another form of cancer, were significantly more likely to have received a lab test for colorectal cancer. The researchers noted that public health agencies have embarked on aggressive campaigns over the past few years to encourage more individuals to seek colorectal cancer testing. These programs also encourage doctors to explain the benefits of screening to their patients. The fact that more people who have had contact with the healthcare system have been tested is a sign that these efforts may be working.
http://www.privatemdlabs.com/blood-testing-news/Colon/Colon-cancer-awareness-programs-may-be-delivering-results--- $800733829.php Pre-Cancerous Polyps May Be Hidden When Bowel Prep Inadequate Prior to Colonoscopy (Apr.1/12)
Researchers have found that when patients don't adequately prep for their colonoscopy test by cleansing their colons, doctors often can't see potentially dangerous pre-cancerous lesions. Researchers say that doctors often missed at least one pre-cancerous growth in about one-third of patients who did not properly prepare for their colonoscopy. Those polyps and other markers of cancer risk were only
discovered months later when patients had their next colonoscopy. Although several studies have found that up to a quarter of colonoscopy patients don't prepare adequately for the test, the new study is the first to point out the potential consequences of poor bowel preparation in patients at average risk. "Because so many of the patients had a follow-up screening less than a year after the initial test, we strongly suspect that most of the pre-cancerous growths found during the second colonoscopy already were present at the time of the initial test," says first author Reena Chokshi, MD. The researchers say their findings suggest that if a physician is having difficulty seeing the colon due to inadequate bowel prep, the colonoscopy should be stopped and rescheduled. Physicians often can detect preparation problems during the first few minutes of the procedure. "And based on this study, we would say that rather than subjecting a patient to the potential risks of a full colonoscopy when we may not be able to detect polyps, or other pre-cancerous growths called adenomas, it may be better to bring that patient back as soon as possible for a repeat procedure with better bowel preparation. On the day before a colonoscopy exam, people are asked to stop eating solid food and to consume only clear liquids. Later in the day and the next morning, patients drink bowel-cleansing mixtures to empty the colon prior to the examination. The test itself usually takes less than an hour, and patients are sedated during that time. Using a tiny camera, doctors are able to look at the walls of the colon in an attempt to detect polyps and other pre-cancerous growths. Once detected, those growths can be removed during the course of the colonoscopy. Patients often must miss two days of work: the day of preparation and the day of the test. The researchers retrospectively studied patients who had an average risk of colon cancer and got screening colonoscopies in the outpatient endoscopy center. Individuals with a history of inflammatory bowel disease, a family history of colorectal cancer or a medical history of colon polyps were not included in the study. In the five-year span between 2004-09, 373 patients at the center were identified as having inadequate bowel preparation. Of the 133 patients who later had a second colonoscopy during the study period, 33.8% had at least one pre-cancerous adenoma detected in that repeat screening. And almost one in five of that group were considered to be at high risk for colon cancer because they either had more than three adenomas detected, or the test discovered at least one large lesion. In fact, the researchers found that 18% of the patients who had a second colonoscopy would have been given different recommendations if their polyps and adenomas had been detected during the initial screening, such as more frequent colonoscopies to monitor the development of growths in the colon.
Chokshi, RV, et al., Prevalence of missed adenomas in patients with inadequate bowel preparation on screening colonoscopy. Gastr Endos, vol. 75, 2012. Epub ahead of print. Study Looks at Adherence to CRC Screening Recommendations
When patients were offered a choice of colorectal cancer screening with either FOBT or colonoscopy, they were significantly more likely to complete that screening than when their doctors recommended only FOBT or only colonoscopy. Nearly 1000 racially and ethnically diverse patients in urban primary care practices were randomly assigned to get colorectal cancer screening via:
Fecal occult blood testing (FOBT) Colonoscopy,
Their choice of either FOBT or colonoscopy.
Overall, 58% were screened within the next year with the following results:
67% of those offered an FOBT home test finished screening. 38% of those who got a colonoscopy recommendation actually had the exam. 69% of patients who had a choice were screened.
Non-whites were more likely to complete FOBT, while whites accepted colonoscopy more often. Latinos and Asians were more likely to complete screening than African Americans. Investigators concluded: The common practice of universally recommending colonoscopy may reduce adherence to CRC screening, especially among racial/ethnic minorities. Significant variation in overall and strategy-specific adherence exists between racial/ethnic groups; however, this may be a proxy for health beliefs and/or language. These results suggest that patient preferences should be considered when making CRC screening recommendations. Inadomi, John M, et al., Adherence to Colorectal Cancer ScreeningA Randomized Clinical Trial of Competing Strategies. Archives of Internal Medicine, Vol. 172, No. 7, April 9, 2012. No Laxative Required for Certain Type of Virtual Colonoscopy (May 17/12)
A CT-scan-based form of virtual colonoscopy that does not require laxative preparation appears to be as effective as standard colonoscopy in identifying the intestinal polyps most likely to become cancerous. The new technique, which uses computer-aided systems both to virtually cleanse and to analyze the images acquired, was able to identify more than 90% of the common polyps called adenomas that were 10 mm or larger. Colon screening can save lives, but not enough people participate, in part because of the discomfort of the required laxative preparation. In this study, the laxative-free form of CT colonography performed well enough that it might someday become an option for screening, which will hopefully increase patient participation. Optical colonoscopy, the most common form of screening for colon cancer, allows examination of the internal surface of the colon through a fiberoptic tube with a light and camera at the end. In addition to being sedated for the examination, patients must ingest laxative
preparations - sometimes up to a gallon of liquid - the preceding day in order to completely clean out the colon, a process universally regarded as unpleasant. CT colonography, which produces images via CT scanning and not direct visualization, has become available in recent years. But while it is as effective as colonoscopy for detecting polyps, does not require sedation, and can be used in some patients for whom colonoscopy is not appropriate. CT colonography still requires the laxative preparation that many patients choose to avoid. Preparation for the procedure tested in the current study involves two days of a low-fiber diet and oral ingestion of small doses of a contrast agent to label fecal material in the colon. Software programs developed by the research team subtract labeled feces from the CT images and analyze the images for the presence of lesions - primarily adenomas, the type of polyps most likely to develop into cancer. The investigators recruited patients scheduled for screening colonoscopy between June 2005 and October 2010. Study results showed the effectiveness of computer-assisted, laxative-free CT colonography to be comparable to that of optical colonoscopy for detecting adenomas 10 mm or larger. While it did not do as well finding smaller polyps, those lesions are less likely to show cellular changes associated with higher risk for cancer development. Among colonoscopy-confirmed lesions that showed such risk-associated changes, 85% were 10 mm or larger. Three cases of colon cancer were diagnosed among the study group, and all of those lesions were 10 mm or larger and were detected by both screening methods. Participants completing the survey indicated that laxative-free CT colonography is more comfortable and easier to prepare for, and it was the preferred screening method for 62% of respondents.
http://www.medicalnewstoday.com/releases/245368.php Young Colon Cancer Patients Have Challenges with Treatment Costs
Although nearly four out of ten stage III colon cancer patients had serious financial problems during treatment, treatment-related expenses were particularly hard on patients under fifty. After taking all factors into account, young patients were more than fifty times more likely to experience financial hardship than patients over 75. Treatment costs drove them to:
be in debt have to borrow money from family or friends sell or refinance their homes experience a more than 20% drop in income
Financial difficulties sometimes led to stopping treatment early despite the fact that nearly all patients had insurance. 5.4 percent skipped treatments and 7.2% refused treatment altogether because of financial problems. Young patients were nearly nine times more likely to skip or refuse treatments. Patients with incomes under $30,000 were six times more likely not to get recommended treatment. Not being able to work because of disability, leave of absence or employment also raised risk of not getting treatment. Researchers sent questionnaires to 555 stage III colon cancer patients treated in Washington State between January 1, 2008 and March 1, 2010, asking them about the financial impact of their cancer treatment. Over half returned the surveys. Serious financial hardships reported by all patients in the study included:
21.8% were in debt due to treatment-related expenses with an average debt of $26,860. 16.5% borrowed money from family or friends, on average $14,144. 5.4% either sold their home or took out a second mortgage 23.9% had at least a 20% drop in household income
Factors that contributed to financial problems were
Annual income less than $50,000 Medicaid or no insurance Work disability, leave of absence, or unemployment
People less likely to have serious financial issues were
Widows People insured by Medicare with supplemental insurance Retirees
Researchers concluded: A significant proportion of patients undergoing adjuvant chemotherapy for stage III colon cancer may experience financial hardship, despite having health insurance coverage. Interventions to help at-risk patients early on during therapy may prevent long-term financial adverse effects. They also wrote: Future research should focus on exploring the impact of various financial experiences on quality of life and identifying specific factors that contribute to financial hardship. Interventions should be developed to help at-risk individuals before they face financial ruin. Shankaran, Veena, et al., Risk Factors for Financial Hardship in Patients Receiving Adjuvant Chemotherapy for Colon Cancer: A Population-Based Exploratory Analysis. J of Clin Onc. Early Release, March 12, 2012. A New Biomarker That Predicts Colorectal Lesions
The most frequently occurring lesions in the colon are the hyperplastic polyps. Hyperplastic polyps have long been considered as lesions with no malignant potential and colonoscopy for these patients is not recommended. However, recent works suggest that hyperplastic polyps may represent precursor lesions of some sporadic colorectal cancers. Until now, no biomarker allows to identify the subset of hyperplastic polyps that may have a malignant potential. Because the hormone precursor progastrin has been involved in the development of colon cancer, researchers investigated whether its expression in hyperplastic polyps predicts the occurrence of colonic lesions after resection of hyperplastic polyps. They retrospectively analyzed progastrin expression in hyperplastic polyps from 74 patients without history of colorectal pathology. In the study, 41% of patients presenting an initial hyperplastic polyp subsequently developed adenomatous polyps, recognized as precursor lesions for colorectal adenocarcinomas. Progastrin was over expressed in the hyperplastic polyps in 40% of the patients. They showed a significant association between progastrin over expression and shortened neoplasm-free survival. Patients with high over expression of progastrin had a 5-year neoplasm-free survival rate of 38% as compared with 100% for the patients with low progastrin expression. In addition, they established a predictive test on the basis of progastrin staining and patients' age that predicts occurrence of neoplasm after developing a first hyperplastic polyp. They show that progastrin expression evaluation in hyperplastic polyps is an efficient prognostic tool to determine patients with higher risk of metachronous neoplasms who could benefit from an adapted follow-up.
Do, Catherine, et al., A New Biomarker That predicts colonic neoplasia outcome in patients with hyperplastic colonic polyps. Cancer Prev Res; 5(4); 675-84. Choosing the Cancer Tests and Treatments That Are Truly Required (Apr.3/12)
Oncologists have joined eight other physician specialty organizations in the Choosing Wisely® campaign with a list of the Top Five Cancer-Related Tests, Procedures, and Treatments That Many Patietns Do Not Need. Choosing Wisely asked each of the specialist groups to come up with a list of five things doctors and patients should question in order to improve evidence-based care, avoid tests or treatments that don’t help, and reduce the burden of health care costs. Here are the Top Five lists from the other groups. The American Society of Clinical Oncology built the Top Five List for Oncology, based on work that ASCO’s Cost of Care Task Force has been doing for several years to identify diagnostic tests or treatments that are commonly ordered, expensive, and of unproven value. While the Top Five list is based on evidence for effective cancer care, its recommendations are not written in stone. They are guidelines for patients, families, and doctors to begin a conversation about tests and treatments and costs in order to make good decisions about the best care for each individual. Briefly the Top Five list recommends the following:
Stop active cancer treatment when patients are too ill to benefit, aren’t eligible for a clinical trial,
previous treatments haven’t worked, and there are no more standard treatment options.
Don’t use advanced imaging tests (CT, PET, bone scans) for early prostate cancer which has a
Don’t use similar imaging tests for early breast cancer that has a low risk of spreading. Don’t use PET, CT, bone scans or biomarkers to follow-up breast cancer patients without
symptoms after treatment intended to cure them.
Don’t give medicines to stimulate white cells in patients with a low risk of developing low counts
More specifically the Top Five for Oncology published ahead of print in the Journal of Clinical Oncology April 3 are:
Do not use cancer-directed therapy for patients with solid tumors who have the following
characteristics: low performance status (3 or 4), no benefit from prior evidence-based interventions, not eligible for a clinical trial, and with no strong evidence supporting the clinical value of further anticancer treatment.
Don’t perform PET, CT and radionuclide bone scans in the staging of early prostate cancer at
Don’t perform PET, CT and radionuclide bone scans in the staging of early breast cancer at
Don’t perform surveillance testing (biomarkers) or imaging (PET, CT and radionuclide bone
scans) for asymptomatic individuals who have been treated for breast cancer with curative intent.
Don’t use white cell stimulating factors for primary prevention of febrile neutropenia for
patients with less than 20% risk for this complication.
Patients with advanced colorectal cancer and their families may be alarmed at the recommendation to stop chemotherapy when performance status is poor and there are no standard, evidence-based treatments. Patients with a performance status of 3 spend at least half their day in bed or in a chair and have difficulty taking care of themselves. Poor performance status is often a sign of increasing toxicity from chemo, reduced response to the chemo drugs, and poor survival time. Treatment may do more harm than good. A rule of thumb for performance status is whether a patient can walk without help into the chemotherapy suite. At this point supportive care may benefit patients more than additional chemotherapy. It’s time for a frank discussion with the doctor about the benefit and harm of more treatment. Lowell E. Schnipper and the team who developed the Top Five write: The available guidelines established by expert panels have all concluded that if a patient’s cancer has grown during three different regimens, the likelihood of treatment success is so poor and toxicity so high that further anticancer treatment is not recommended. While patients and families may urge doing everything possible, this is not always the best course. Schipper and his colleagues conclude: The Top 5 list represents a series of practices in frequent use in common clinical scenarios that are not supported by strong evidence. Reconsidering their use, one patient at a time, is likely to improve the value of care that is provided, which in this case means the desired clinical outcome at the lowest cost to the patient and society. Nonetheless, ASCO recognizes that the care of every person with a life threatening disease is challenging and must be responsive to unique features of that particular individual’s circumstances. For that there will never be a substitute. http://fightcolorectalcancer.org/research_news/2012/04/choosing_wisely_what_cancertests_and_treatments_do_you_really_need GI Tests That Are Truly Required (Apr.5/12)
How soon should average risk people get another colorectal cancer screening after they have a normal colonoscopy? No sooner than 10 years, the American Gastroenterological Association recommends as part of the Choosing Wisely campaign. The AGA’s list of Five Things Physicians and Patients Should Question includes:
Use the lowest possible effective dose of acid reducing medicines to treat grastroesophageal
After a negative, quality colonoscopy, don’t repeat colorectal cancer screening by any method
After removing 1 or 2 small (less than 1 centimeter) adenomatous polyps without signs of
cellular change (dysplasia), don’t repeat the colonoscopy for at least 5 years.
After two endoscopies without dysplasia, people with Barrett’s esophagus shouldn’t have
another upper endoscopy for at least 3 years.
Patients with abdominal pain shouldn’t have a repeat CT scan unless there are major changes
AGA’s list is based on current published recommendations for the time between colonoscopy and endoscopy in people with low risks for cancer. The Choosing Wisely campaign wants doctors and patients to talk together about tests and treatments that are supported by evidence, don’t duplicate other tests or procedures, are free from harm, and are truly necessary.
http://fightcolorectalcancer.org/research_news/2012/04/do_you_need_that_test_wise_choices_from_gastroenterologists Genes Discovered That Cause Colorectal Cancer Recurrence (May 1/12)
For decades, patients diagnosed with early-stage colorectal cancer believed they were relatively fortunate. The view was, "The disease has been caught early; treatment with surgical removal of the tumor alone will suffice; I won’t need adjuvant chemotherapy; and my prospects for beating the disease are very good." This view was driven by the assumption that all early-stage colorectal cancer tumors were low-risk for recurrence. Recurrence and mortality rates associated with early-stage colorectal cancer are, in fact, much higher than previously realized. Nearly one in three patients with Stage 2 colon cancer who have undergone surgical removal of their tumor alone will have a recurrence of their cancer, and more than 80% of those who do have recurrence will die from their disease. Dr. Peter Lenehan, Everist Genomics’ chief medical officer, explained, “We now know that patients with ‘high-risk’ early-stage colorectal cancer are up to 29 times more likely to have a recurrence of their tumors than patients with low-risk disease. More specifically, in a recently completed study involving 291 colorectal cancer patients, fewer than 3% of patients identified with low-risk tumors experienced a recurrence of their cancers compared to a staggering 68% recurrence rate in patients with high-risk early-stage disease." This insight led the scientific team at Everist Genomics to ask several questions. “Could it be that previous research suggested that adjuvant chemotherapy had little impact on recurrence rates in early-stage colorectal cancer precisely because physicians were unable to distinguish early-stage low-risk tumors from high-risk tumors? What if we had a test that would accurately identify patients with early-stage high-risk tumors and you treat these patients with surgical removal of their tumor and add chemotherapy?" "What would happen to survival rates in these patients? The answers to these questions were remarkable." The scientific team at Everist Genomics identified research which revealed that patients
with high-risk Stage II colorectal tumors can benefit greatly from adjuvant therapy, with three-year disease-free survival rates increasing from 84.7% in patients that did not receive chemotherapy to 96.4% in those that did. Improvements in five-year overall survival rates increase from 86.4% to over 98%. These insights led the scientists at Everist Genomics to commence a two-year development program to discover the combination of genes and their expression levels that would identify patients with these high- risk early-stage colorectal cancer tumors. Alex Charlton, executive vice chairman of Everist Genomics, pointed out, “The human genome consists of roughly 25,000 genes. In order to develop a test capable of identifying these high-risk tumors, our task was to pinpoint the handful of genes and specific gene expression levels responsible for creating these tumors. Accomplishing this required analyzing and evaluating vast quantities of genomic information and potential combinations of genes. The genomic culprits turned out to be a combination of five specific genes and gene expression levels. If they are present in a patient’s early-stage colorectal cancer tumor, then it’s a high-risk tumor. Based on these insights, Everist Genomics has created the world’s only molecular diagnostic test, OncoDefender-CRC, capable of accurately identifying tumors at high risk for recurrence amongst all early-stage (Stage I/II) colon and rectal cancers. OncoDefender-CRC testing is provided as a CLIA lab-based service. “The total cost of treating a patient after they have experienced a recurrence of their colorectal cancer is over $280,000" Charlton explained. “However, preventive chemotherapy costs the healthcare system about 20% of this amount. We believe that this combination of improved medical outcomes and reduced healthcare costs are key drivers for OncoDefender-CRC testing." Everist Genomics made the OncoDefender-CRC test available commercially in November 2011. During the first month of commercial availability, Everist Genomics has already fulfilled physician requests for over 1,000 OncoDefender specimen collection kits. Further supporting the clinical and financial merits of the test, Sanford Health Plan has established a reimbursement policy for OncoDefender-CRC, which will allow its members to receive coverage for the test beginning in January 2012. http://www.endonurse.com/articles/2012/05/researchers-find-genes-that-cause-colorectal-canc.aspx New Colorectal Cancer Survivorship Program Established at NYGH (May 8/12)
The Honourable Deb Matthews, Minister of Health and Long-Term Care, MPP Michael Coteau, the North York Family Health Team, and North York General Hospital celebrated the launch of the Colorectal Cancer Survivorship Program (CCSP). The CCSP is a new model of cancer survivorship care that transfers the monitoring of patients, who have finished active treatment, to primary care from oncologists and surgeons. This innovative program, developed by the North York Family Health Team (NYFHT) and North York General Hospital (NYGH), will centralize follow-up care for patients and alleviate wait times for newly diagnosed patients needing to see a cancer specialist. "As part of our Action Plan for Health Care, we are supporting transformation that aims to provide patients with the right care, in the right place, at the right time," said Deb Matthews, Minister of Health and Long-Term Care. "Programs like the Colorectal Cancer Survivorship Program here at the North York FHT are prime examples of innovations that are not only putting the needs of patients first , but are also highlighting the integral role Ontario's nurse practitioners have to play in improving patient care." The Program's model follows the latest best practices and includes three important components: nurse practitioners lead and coordinate follow up testing, stoma care is available, and psychological support from a social worker is also provided. Other services offered include, group sessions by the Colorectal Cancer Association of Canada and consults with psychiatrists from NYGH who also support the Hospital's cancer care program. "This model is a smart innovation," said Dr. Kimberly Wintemute, medical director, NYFHT. "The Colorectal Cancer Survivorship Program will increase the capacity of oncologists to provide care to patients requiring active treatment, reducing the duplication of services and tests by centralizing care with a nurse practitioner who will communicate the patient's care plan to everyone who needs to know." "Our partnership with the North York Family Health Team provides cancer survivors with a comprehensive care experience that addresses both their physical and psychological needs," said Dr. Tim Rutledge, President and CEO, NYGH. "This program is a terrific example of how, through collaboration, and with interprofessional teams, we can provide high quality care in an efficient manner." Utilizing an interdisciplinary team of primary care physicians, nurse practitioners and social workers, patients enrolled in the CCSP will benefit from the care provided by a robust program that translates evidence-based care into clinical best practices. The North York Family Health Team (NYFHT) is composed of a multidisciplinary team of Registered Nurses, Social Workers, Registered Dietitians, Nurse Practitioners and Pharmacists and 61 Family Physicians. There are approximately 60,000 patients rostered with the FHT Family Physicians. NYFHT is an academic Family Health Team associated with the Department of Family & Community Medicine at North York General Hospital and the University of Toronto. North York General Hospital, affiliated with the University of Toronto, is one of Canada's leading community academic hospitals. We offer our culturally diverse community a wide range of acute care, ambulatory and long-term care services across three sites. The hospital embraces health by providing innovative and compassionate care for the whole family at every stage of life.http://www.newswire.ca/fr/story/970235/new-colorectal-cancer-survivorship-program-the-first-of-its-kind-in-ontario Study Highlights Need for Coordination of Care in Stage II and III Rectal Cancer Treatment (May 17/12)
Research from the University of Alberta provides new insight into treatment patterns for people with stage two and three rectal cancer—information that ultimately will help physicians improve care strategies for patients province wide. The study of more than 900 patients with rectal cancer is a first step to
addressing gaps in care and ensuring that general practitioners, surgeons and oncologists improve co-ordination of treatment for patients. "Coordinating patient care is a challenge health-care agencies face around the world—how do we maximize co-ordination? There isn't a single answer," said Winget, who also holds an appointment with Cancer Care, Alberta Health Services. "One of the things this study shows is there is room for improvement in coordinating health care. We as a medical community need to figure out how to improve it." They examined records of rectal cancer patients diagnosed from 2002 to 2005. The goal was to determine whether patients received treatment consistent with guidelines and to identify patient groups at risk of not receiving guideline treatment. Canadian guidelines call for a minimum of surgery followed by chemotherapy. Radiation therapy may also be given before or after surgery. The study showed that 54% of patients did not receive treatment consistent with the guidelines, including 18% who did not see an oncologist—a necessary step to receive chemotherapy. Some 28% saw an oncologist but did not receive chemotherapy, and 8% received chemotherapy late (more than 12 weeks after surgery). The study also examined demographic data such as age, income and area of residence to look at how they may affect treatment patterns throughout the province. Patients living in Edmonton were twice as likely to have a consultation with an oncologist after surgery as those living in Calgary or other parts of central or southern Alberta. Once a patient had a consult with an oncologist, however, region of residence was not associated with receiving chemotherapy. Age was another factor, with 78% of patients aged 75 and older not receiving treatment according to guidelines. Some 42% were not referred to an oncologist. "Just being 75 or older should not be a reason not to see an oncologist or not to get treatment. However, the data reflect the complexity in making treatment decisions in this age group," claims the co-author of the study. The bottom line is there's variation in how individual oncologists perceive co-morbidities and age in a patient's ability to tolerate chemotherapy and be a chemo candidate," Winget said. "We wouldn't expect 100% of rectal cancer patients to be medically eligible, but surely the number should be more than 50%." Winget said the overall results suggest that tighter co-ordination between surgeons and oncologists is needed, as is greater clarity regarding guidelines for colon and rectal cancer, which are similar diseases but are treated slightly differently.
http://medicalxpress.com/news/2012-05-highlights-stage-rectal-cancer-treatment.html NUTRITION & HEALTHY LIFESTYLE Meat Consumption and Colorectal Cancer Risk (Mar.30/12)
Greater consumption of red and processed meat has been associated with an increased risk of colorectal cancer in several recent studies. Heterocyclic amines (HCAs) have been identified in this association. In this study conducted within the Multiethnic Cohort Study, researchers examined whether greater consumption of total, red or processed meat was associated with the risk of colorectal cancer among 165,717 participants who completed a detailed food frequency questionnaire at baseline. In addition, they examined whether greater estimated intake of HCAs was associated with the risk of colorectal cancer among 131,763 participants who completed a follow-up questionnaire that included a meat-cooking module. A total of 3,404 and 1,757 invasive colorectal cancers were identified from baseline to the end of follow-up and from the date of administration of the meat-cooking module to the end of follow-up, respectively. The results of this study did not support a role for meat or for HCAs from meat in the development of colorectal cancer, though the researchers did state that they could not rule out the possibility of a modest effect.
Ollberding, Nicholas, et al., Meat consumption, heterocyclic amines and colorectal cancer risk: the multiethnic cohort study. Inter J of Cancer. Early online view. Doi: 10.1002/ijc.27546 Obese Patients & Colorectal Cancer Survival
Patients who are obese before being diagnosed with colorectal cancer are more likely to die of their disease than patients who are at a normal weight prediagnosis, according to the results of this large prospective study. Investigators examined the association of pre- and postdiagnosis body mass index (BMI) with all-cause and cause-specific survival in 2303 men and women who were diagnosed with nonmetastatic colorectal cancer. The CPS-II Nutrition Cohort is a prospective study of cancer incidence in which participants completed a questionnaire at enrollment in 1992 and 1993 that sought information on demographics, medical history, body weight, physical activity, cigarette smoking, diet, and other lifestyle factors. Patients were also asked to respond to repeat questionnaires at multiple time points to provide updated information on weight and incident cancer. Given that there are more than 1.1 million colorectal cancer survivors in the United States, it is important to identify factors that affect colorectal cancer survivors. The only established prognostic factors for colorectal cancer are tumor characteristics, including tumor stage and grade, lymph node involvement, and the presence of distant metastasis. Little is known about the prognostic role of factors such as BMI, which has important clinical and public health significance. A total of 851 participants with colorectal cancer died during the 16-year follow-up period, including 380 deaths due to colorectal cancer and 153 deaths due to cardiovascular disease (CVD). The investigators analyzed prediagnosis BMI at a mean of 7 years before patients were diagnosed with colorectal cancer, and found that obese BMI relative to normal was associated with a higher risk of all-cause mortality. Obesity was defined as a BMI ≥ 30 kg/m2, and normal weight was defined as a BMI from 18.5 to 24.9 kg/m2. The association between BMI and all-cause mortality was stronger for patients diagnosed with rectal cancer than for those diagnosed with colon cancer. There were no associations of postdiagnosis obese BMI, which was reported a mean of 18 months after colorectal cancer diagnosis, with all-cause or cause-specific mortality. Investigators maintain that the mechanisms by which obesity
influences colorectal cancer prognosis are not well defined and may include biologic mechanisms that are associated with colorectal cancer incidence, including insulin and insulin-like growth factors, among others. The authors cite the ability to examine both pre- and postdiagnosis reports of BMI as an important study strength, along with its relatively large sample size, prospective design, and the inclusion of detailed information on key confounders.
Campbell, PT, et al., Impact of body mass index on survival after colorectal cancer diagnosis: the cancer prevention study-ii nutrition cohort. Published online ahead of print. J Clin Oncol. 2012; 30(1): pp. 42-52 Vitamins, Minerals, Essential Fatty Acids and CRC
The risk for colorectal cancer may be influenced by the dietary intake of various vitamins, minerals and essential fatty acids. Researchers conducted a pooled analysis of dietary data collected using food diaries in seven prospective studies in the United Kingdom Dietary Cohort Consortium. Five hundred sixty-five cases of colorectal cancer were matched with 1,951 controls on study centre, age, sex and recruitment date. Dietary intakes of
the ratio of n − 6 to n − 3 fatty acids
were estimated and their associations with colorectal cancer examined adjusting for exact age, height, weight, energy intake, alcohol intake, fiber intake, smoking, education, social class and physical activity. The results showed that there were no statistically significant associations between colorectal cancer risk and dietary intake of any of the vitamins, minerals or essential fatty acids examined.
Key, Timothy J., et al., Vitamins, minerals, essential fatty acids and colorectal cancer risk in the united kingdom dietary cohort consortium. Inter J of Cancer. doi: 10.1002/ijc.27386 Starchy Foods Cut Bowel Cancer Risk
Eating more corn, lentils, peas, beans and other legumes can reduce the risk of developing bowel cancer, Australian researchers have found. These foods are high in resistant starch, a type of fiber that cannot be digested and instead passes through to the bowel where it is fermented. Australia's national science agency, the CSIRO, said even though Australians eat more dietary fiber than many other Western countries, bowel cancer was still the second most commonly reported cancer in the country. "We have been trying to find out why Australians aren't showing a reduction in bowel cancer rates and we think the answer is that we don't eat enough resistant starch, which is one of the major components of dietary fiber," the CSIRO's Dr. David Topping said of the findings. "We studied various sources of resistant starch, including corn and wheat, and the results suggest they could all protect against DNA damage in the colon, which is what can cause cancer." Resistant starch is sometimes called the third type of dietary fiber and is found in legumes, some whole grain breads and cereals, firm bananas and cooked potatoes, pasta and rice. The recommended daily intake of resistant starch is about 0.7 ounces (20 grams) -- equivalent to three cups of cooked lentils -- almost four times more than the amount consumed in a typical Western diet. CSIRO researcher said they had been able to develop a strain of wheat with increased levels of resistant starch. "If this is introduced to grains grown popularly then there will be an additional set of grains with high levels of resistant starch in commonly consumed foods." "Having a wheat high in resistant starch greatly expands the opportunity for people to eat it because it can be used in bread and other baked goods so more people will be increasing their intake and realizing the health benefits. "It takes about 15 years from the first bowel cancer-initiating DNA damage to full-blown cancer, so the earlier we improve our diets the better."
Topping, David, et al., Resistant Starches Protect against Colonic DNA Damage and Alter Microbiota and Gene Expression in Rats Fed a Western Diet. The J of Nutrition. Jn.111.147660 Exercise Might Improve Survival in Colon Cancer
Being physically active might lengthen the lives of people with breast and colon cancer, a new study suggests. Exercise may also benefit patients with other cancers, but there is no substantial evidence to make that claim, the researchers added. We have lots of data that says physical activity after a cancer diagnosis is generally safe and is associated with many improvements in overall quality of life, and these
data suggest that it may even be beneficial in terms of prolonging life. For the study, Ballard-Barbash's team analyzed 27 observational studies published between January 1950 and August 2011 that looked at cancer survival and physical activity. The evidence of these benefits was strongest for breast cancer patients, where exercise significantly reduced death from all causes including breast cancer, the researchers found. Strong data also existed for improved survival among colon cancer patients. The researchers also looked at other randomized controlled studies that suggested exercise benefited patients in a variety of ways, including improving insulin levels, reducing inflammation and possibly improving the body's immune system. Many treatments may increase survival, but at a cost of quality of life; physical activity may not only extend life but also enhances its quality. Samantha Heller, a dietitian, nutritionist, exercise physiologist and clinical nutrition coordinator of the Center for Cancer Care at Griffin Hospital, in Derby, Conn., said that "we have evidence to suggest that physical activity not only improves survival of people living with cancer, but it also decreases the risk of many other chronic diseases." "Conversely, physical inactivity has been associated with many cancers including breast, colon, prostate, pancreas and melanoma," she said. Because of certain chemotherapy and radiation therapy treatments for cancer, survivors may be at an increased risk of additional cancers and chronic diseases such as cardiovascular disease, Heller said. "Therefore, a healthy lifestyle including regular exercise and a healthy diet is essential for survivors to reduce the risk of cancer recurrences and other diseases," she said. Regular physical activity also improves sleep, psychological and emotional well-being and helps manage stress, Heller said. "The number of cancer survivors is, happily, growing in the U.S.," she said. "We need to get the word out to them that exercise, whether it is walking, dancing, running, swimming or hula hooping, will boost their health, fitness level and quality of life."
Ballard-Barbash, Rachel, et al., Physical Activity Linked To Reduced Mortality in Breast and Colon Cancer PatientsJournal of the National Cancer Institute. May 8, 2012. Fish May Prevent Colorectal Cancers
People who frequently eat plenty of fish may have a significantly lower risk of colon cancer and rectal cancer compared with non-consumers. The finding was a result of an analysis of 41 past international studies about association between fish consumption and cancer diagnoses and death. “Our findings from this meta-analysis suggest that fish consumption is inversely associated with colorectal cancer,” wrote Jie Liang and colleagues from Xijing Hospital of Digestive Diseases in Xian, China. Overall, regularly eating fish was tied to a 12% lower risk of developing or dying of colorectal cancers, said the scientists who found that the protective effect was stronger for rectal cancer. Reportedly, people who consumed the highest amounts of fish had a 21% lower risk of rectal cancer while their colon cancer odds was just 4% lower than non-fish eaters. The study focused specifically on benefits of eating fresh fish. It was also unable to pinpoint what types of fish or which of the cooking methods were tied to the most benefits. "Cooking temperatures might affect the risk of colorectal cancer," suggested Liang. He cited recent evidence suggesting that eating plenty of meat and fish barbecued or grilled over high heat is tied to greater risk of cancer.
Liang, Jie, et al., Fish consumption and colorectal cancer risk in humans: a systematic review and meta-analysis. The Amer J of Medicine. Published online April 18, 2012.
Does hormone replacement therapy cause breast cancer? An application of causal principles to three studies Part 4. The Million Women Study Samuel Shapiro,1 Richard D T Farmer,2 John C Stevenson,3 Henry G Burger,4 Alfred O Mueck5 Abstract Part 1 we concluded that the CR findings Background Based principally on fi ndings in three studies, the collaborative reanalysis (CR), the To
 COLORECTAL CANCER RESEARCH UPDATES
COLORECTAL CANCER RESEARCH UPDATES 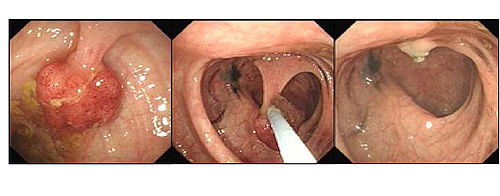 A Colon Polyp Snared and Gone
A Colon Polyp Snared and Gone