Tadalafil appartiene alla classe degli inibitori selettivi della fosfodiesterasi di tipo 5, con un profilo farmacocinetico caratterizzato da un’emivita terminale di circa diciotto ore. Dopo somministrazione orale viene assorbito rapidamente e raggiunge concentrazioni plasmatiche massime in due ore. La biotrasformazione avviene principalmente tramite CYP3A4 con formazione di metaboliti inattivi, escreti in prevalenza con le feci. L’elevato legame alle proteine plasmatiche (>90%) assicura una distribuzione stabile. Nei confronti delle altre molecole della stessa classe, cialis compresse italia è noto per la durata prolungata dell’attività farmacologica.
Evaluation of adipose-derived stromal vascular fraction or bone marrow-derived mesenchymal stem cells for treatment of osteoarthritis
Evaluation of Adipose-Derived Stromal Vascular Fraction orBone Marrow-Derived Mesenchymal Stem Cells for Treatment ofOsteoarthritis
David D. Frisbie, John D. Kisiday, Chris E. Kawcak, Natasha M. Werpy, C. Wayne McIlwraith
Equine Orthopaedic Research Center, Department of Clinical Sciences, Colorado State University, 300 West Drake Road, Fort Collins, Colorado80523
Received 19 December 2008; accepted 7 May 2009Published online in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/jor.20933
ABSTRACT: The purpose of this study was the assessment of clinical, biochemical, and histologic effects of intraarticular administeredadipose-derived stromal vascular fraction or bone marrow-derived mesenchymal stem cells for treatment of osteoarthritis. Osteoarthritiswas induced arthroscopically in the middle carpal joint of all horses, the contralateral joint being sham-operated. All horses receivedtreatment on Day 14. Eight horses received placebo treatment and eight horses received adipose-derived stromal vascular fraction in theirosteoarthritis-affected joint. The final eight horses were treated the in osteoarthritis-affected joint with bone marrow-derived mesenchymalstem cells. Evaluations included clinical, radiographic, synovial fluid analysis, gross, histologic, histochemical, and biochemical evaluations. No adverse treatment-related events were observed. The model induced a significant change in all but two parameters, no significanttreatment effects were demonstrated, with the exception of improvement in synovial fluid effusion PGE2 levels with bone marrow-derivedmesenchymal stem cells when compared to placebo. A greater improvement was seen with bone marrow-derived mesenchymal stem cellswhen compared to adipose-derived stromal vascular fraction and placebo treatment. Overall, the findings of this study were not significantenough to recommend the use of stem cells for the treatment of osteoarthritis represented in this model. ß 2009 Orthopaedic ResearchSociety. Published by Wiley Periodicals, Inc. J Orthop Res
bone marrow-derived mesenchymal stem cells; stromal vascular fraction; osteoarthritis; in vivo model; equine
Joint disease and specifically osteoarthritis (OA) is one
study10 has been published limiting the overall trans-
of the most prevalent and debilitating diseases clinically
lational information. The goal of this study was to assess
affecting both humans1 and horses.2,3 Furthermore,
BMDMSC and ADSVF ability to decrease the progres-
similarities in joint disease between the two species
sion of OA without joint instability, as well as compare
have allowed translational research to be conducted in
the horse.4 Specifically, models of cartilage healing andOA have been developed in the horse allowing controlled
studies to be performed on therapeutic interventions
Experimental Design and Induction of Osteoarthritis
that have clinical relevance to both human and equine
Twenty-four skeletally mature 2–5-year-old horses, free of
patients.4,5 To date,12 other studies assessing clinically
musculoskeletal abnormalities [pain, range of motion, and
relevant therapeutic interventions have been published
joint effusion in the carpal joints (front knee)], were utilizedin the study. Horses were randomly assigned to one of three
using a randomized blinded placebo controlled model
treatments groups: ADSVF (N ¼ 8), BMDMSC (N ¼ 8), or
of OA in the horse. Currently, no one therapeutic
placebo (PCB) (N ¼ 8). All evaluators were unaware of treat-
intervention for OA in any species has proven effective
at long-term symptom-modifying or disease-modifying
As previously described,5,11 on Day 0, following anesthesia
effects.6 Recently, anecdotal reports have described full
and routine preparation for surgery, each horse underwent
return to athletic function in 70% of equine OA patients
bilateral arthroscopic surgery of the middle carpal joints to
treated using intraarticular (IA) administration of
ensure that there were no preexisting abnormalities. During
adipose-derived stromal vascular fraction (ADSVF)
this procedure, an 8-mm osteochondral fragment was created
(R. Harman et al., 2007, personal communication,
in one randomly selected middle carpal joint. The fragment was
http://www.vet-stem.com). Also, an uncontrolled multi-
allowed to remain adhered to the joint capsule proximally. Amotorized arthroburr was used to debride the exposed sub-
center equine clinical trial using IA treatment of bone
chondral bone between the fragment and parent bone creating a
marrow-derived mesenchymal stem cells (BMDMSC)
15-mm defect. The debris was not actively flushed from the
for inoperable meniscal lesions has shown early prom-
joint, thereby participating in the induction of osteoarthritis.
ise.7 These results, coupled with in vivo studies that
This joint was designated as the OA-affected joint; the sham-
have shown significant disease-modifying effects using
operated contralateral joint was used as the control joint. The
BMDMSC for the treatment of joint instability8 and
arthroscopic portals were closed routinely. Horses assigned to
collagen-induced arthritis,9 have fueled new enthusi-
the BMDMSC group also had a 40–50 mL aspirate of bone
asm for mesenchymal stem cells (MSC) as a novel
marrow suspended in 3,000 units of sodium heparin which was
treatment for OA. To date, one controlled clinical
aseptically harvested from the sternum. Postoperative carefollowed routine clinical standards.
Correspondence to: David D. Frisbie (T: 970-297-4555; F: 970-297-
Routine harvest of adipose tissue occurred for the ADSVF
horses (Vet-StemTM, Poway, CA). Briefly, using systemic
ß 2009 Orthopaedic Research Society. Published by Wiley Periodicals, Inc.
sedation, routine surgical preparation, and local anesthetic, a
6-cm skin incision parallel to the spine at the level of the tail
Tumor Necrosis Factor-a (TNF-a) concentrations in serum
head was made and 10–20 g of adipose tissue was harvested.
and synovial fluid samples were determined using a commer-
A routine closure of the incision was performed. The adipose
cially available indirect ELISA kit (Endogen, Rockford, IL) that
was shipped to the manufacturer, where the tissue was washed
has been previously validated in equine samples.15,16 The assay
with phosphate buffered saline (PBS), minced, then digested in
was used according to manufacturer’s instructions, and
low glucose Dulbecco’s modified Eagle’s medium (DMEM)
absorbance was measured at A450. The upper and lower
containing 10% fetal bovine serum (FBS) and 0.1% collagenase
detection limits were 5,702.196 and 2.1 pg/mL, respectively.
for 3–4 h with agitation. Nucleated adipose cells were pelleted,washed, and resuspended in PBS for injection; finally, the cells
were shipped to CSU. The total nucleated cell count normalized
Following euthanasia on Day 70 with an overdose of pento-
to the lowest quantity obtained, which was 16.3 million
barbital, both middle carpal joints were specifically examined
for degree and location of articular cartilage fibrillation orerosion, as well as synovial membrane hemorrhage.
BMDMSC Culture TechniqueMarrow aspirates were washed in PBS and then mixed with0.8% ammonium chloride. The cell pellet was rinsed with PBS,
resuspended in low glucose DMEM containing 10% FBS, and
Synovial membrane was harvested and placed in neutral-
seeded in flasks at a concentration of 0.66 Â 106 nucleated cells/
buffered 10% formalin, embedded in paraffin, 5-mm sections
cm2. Confluent BMDMSC colonies developed over 10–12 days,
created and stained with hematoxylin and eosin (H&E).
at which point the cells were reseeded and expanded in growth
Sections were assessed for cellular infiltration, synovial
medium containing 1 ng/mL FGF-2. BMDMSC cultures were
intimal hyperplasia, subintimal edema, subintimal fibrosis,
passaged at a split ratio of 1:3 twice prior to treatment.12
Articular cartilage pieces (5 mm2) were obtained from each
joint; samples were fixed neutral-buffered 10% formalin
Horses were housed in stalls (3.65 Â 3.65 m each). Beginning
embedded in paraffin, 5-mm sections created and stained with
on Day 15, horses were exercised on a high-speed treadmill
both H&E or Safranin O, fast green (SOFG). H&E sections
5 days each week throughout the study. Horses were trotted
were evaluated for articular cartilage fibrillation, chondrocyte
(16–19 km/h) for 2 min, galloped (approximately 32 km/h)
necrosis, chondrone formation, and focal cell loss.11 SOFG
for 2 min, and trotted again (16–19 km/h) for 2 min daily to
sections were evaluated for intensity of staining in each
simulate the strenuous exercise of race training.
All horses were treated on Day 14 postsurgery. PCB horses
Articular cartilage proteoglycan content was estimated by use
received 2 mL 0.9% NaCl in their OA-affected joint. The
of a 1,9-dimethyl-methylene blue technique14 on samples
ADSVF horses received 16.3 million total nucleated cells
obtained from each joint that were stored at À808C. For
suspended in 2 mL of 0.9% buffered NaCl in their OA-affected
analysis of cartilage matrix metabolism, articular cartilage
joint. OA affected joints of BMDMSC horses were treated
samples were aseptically collected, and radiolabeled SO4
with a mean of 10.5 million (SEM ¼ 1.1 million cells, range of
(35SO4) incorporation was measured by use of previously
5.6–15 million cells) culture expanded BMDMSC suspended in
Data were evaluated using an ANOVA framework with PROC
Clinical examinations of both forelimbs were performed
GLIMMIX of SAS17 with the horse as a random variable. The
every 2 weeks throughout the study period. Pain was graded
ANOVA tables were used to determine significant main effect
on a standardized 0–5 scale.13 All other clinical, histologic,
and interactions between main effect variables. When indi-
and histochemical outcomes were graded on a 0–4 scale
vidual comparisons were made, a least square means was
(0 represented normal, 4 represented severe change). Joint
utilized and a p-value less than or equal to 0.05 was considered
effusion was measured as an indication of inflammation, and
significant. Data was tested for normality using residual plots
joint range of motion was measured through carpal flexion.
and, when required, natural log transformations performed to
Bilateral radiographic carpal evaluation occurred on
ensure normality. When transformation was performed, data
Day À7, Day 14, and Day 70. Images were evaluated for boney
proliferation at the joint capsule attachment, subchondral bonelysis, and osteophytes.
Synovial fluid was collected weekly from both middle carpal
joints. Samples were assessed for total protein concentration
using a refractometer, cytologic evaluation, total white blood
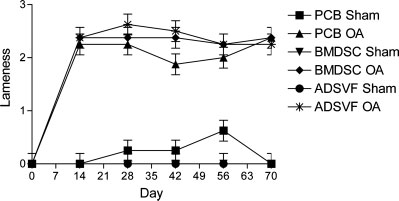
( p < 0.0001) in the OA-affected [2.33 Æ 0.06 (mean -
cell (WBC) count, or stored at À808C for biochemical protein
Æ SE)] limb when compared to the sham-operated limb
A modified 1,9-dimethyl-methylene blue dye-binding assay
(0.00 Æ 0.06) on Day 14 (prior to treatment). Change in
was used to determine glycosaminoglycan (GAG) concentra-
pain values were calculated using Day 14 (the last
tion.14 Synovial fluid concentration of prostaglandin E2 (PGE2)
pretreatment evaluation) as the post-osteoarthritis but
was also assessed (PGE2 Kit, Assay Designs, Ann Arbor, MI).
pretreatment baseline (a positive change score indicates
MESENCHYMAL STEM CELLS FOR OSTEOARTHRITIS
by a significantly ( p < 0.0001) higher cumulative radio-graphic score in the OA-affected (1.19 Æ 0.12) comparedto the sham-operated (0.06 Æ 0.12) joints. No significanttreatment effects were detectable.
Synovial FluidRoutine synovial fluid analysis indicated, as expected,the total protein concentration increased significantly( p < 0.0001) with induction of OA throughout the studyperiod when sham-operated (2.08 Æ 0.09) were com-pared to OA-affected joints (2.70 Æ 0.09). Synovial fluid
Raw lameness scores (mean Æ SEM) plotted by time for
WBC counts were significantly increased ( p < 0.0001)
each treatment group as well as for the osteoarthritis-affected and
by the induction of OA, with OA-affected joints having a
Sham limbs. No significant differences were noted in any compar-ison except for an increase in osteoarthritis joints postsurgery.
higher WBC count compared to sham-operated joints(245 Æ 32 vs. 169 Æ 32 cell/dL, respectively). Therewere no significant treatment effects seen in synovial
improvement). There was no significant improvement in
total protein or WBC counts. Based on the cytology
pain score with respect to treatment (Fig. 1).
of the synovial fluid WBCs, there were significantly( p ¼ 0.0070) less lymphocytes in the ADSVF OA-
affected joints compared to all other joints (Table 1).
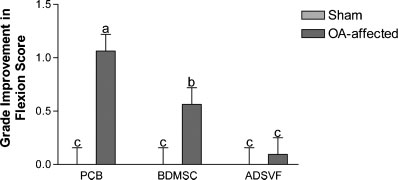
All horses showed a significant increase ( p < 0.0001) in
Synovial GAG concentrations were significantly
flexion score (representing a decreased range of motion)
( p < 0.0001) increased with induction of OA; OA-affected
in the OA-affected (2.50 Æ 0.08) limb when compared
joints (4.45 Æ 0.02 Ln mg GAG/mL) had an increase GAG
to the sham-operated limb (0.08 Æ 0.08) for Day 14.
concentration when compared to sham-operated joints
Change in flexion was calculated using Day 14 as the
pretreatment (4.33 Æ 0.02 Ln mg GAG/mL). No signifi-
post-osteoarthritis but pretreatment baseline, and sig-
cant treatment effects were seen in synovial fluid GAG
nificant improvements ( p ¼ 0.0013) based on treatment
group and joint were seen. Improvement in the
Synovial fluid PGE2 concentrations were signifi-
OA-affected limbs that received PCB and BMDMSC
cantly ( p < 0.0001) increased with induction of OA
treatments were seen when compared to ADSVF
(4.24 Æ 0.09 Ln pg/mL), compared to the sham-operated
joints (3.23 Æ 0.09 Ln pg/mL). A significant ( p ¼ 0.0423)decrease in synovial PGE2 concentration was seen inBMDMSC compared to PCB treatment horses starting
on Day 35 (Fig. 3a). This affect was independent of joint,
All horses showed a significant increase ( p < 0.0001) in
although synovial fluid from OA-affected joints demon-
effusion score in the OA-affected (2.25 Æ 0.08) joints
strated a more pronounced difference (Fig. 3b). Synovial
compared to the sham-operated joints (0.13 Æ 0.08)
fluid TNF concentrations were significantly ( p ¼ 0.0005)
for Day 14. Change in joint effusion was calculated
increased with induction of OA (2.18 Æ 0.3 Ln pg/mL),
using Day 14 as the post-osteoarthritis but pretreat-
compared to sham-operated joints (1.73 Æ 0.29 Ln pg/
ment baseline; no significant differences were observed
mL). The only significant ( p ¼ 0.0194) treatment differ-
ence was higher TNF concentrations in OA-affected(2.69 Æ 0.52 Ln pg/mL) compared to sham-operated
(1.72 Æ 0.51 Ln pg/mL) joints of ADSVF-treated horses.
A significant increase in radiographic joint pathologywas induced following induction of OA as demonstrated
Cytology of the Synovial Fluid White Blood
Cells, Specifically the Percentage of White Blood Cells thatWere Lymphocytes*
OA, osteoarthritis; BMDMSC, bone marrow-derived mesenchymalstem cells; ADSVF, adipose-derived stromal vascular fraction. *Significantly (p ¼ 0.0070) less lymphocytes were noted in the
The grade improvement in flexion score (mean Æ SEM)
adipose-derived stromal vascular fraction osteoarthritis-affected
plotted by treatment group. Different letters indicate a significant
joint compared to all other joints (different letters indicate a
concentration plotted by Day for eachtreatment group (average of boththe osteoarthritis-affected and Shamjoints). An asterisk represents asignificant difference between thecomparison. (b) Natural log of PGE2concentration plotted by Day for eachtreatment group (for both the osteo-arthritis-affected and Sham joints).
At necropsy, hemorrhage within the synovial mem-
Evaluation of articular cartilage for SOFG staining did
brane was significantly ( p ¼ 0.0002) increased in OA-
not demonstrated a significant difference when OA-
affected (1.79 Æ 0.13) compared with sham-operated
affected (8.35 Æ 0.42) were compared to sham-operated
(1.13 Æ 0.13) joints. Similarly, articular cartilage total
(8.28 Æ 0.42) joints or treatment comparisons.
erosion scores were significantly ( p < 0.0001) increasedin OA-affected joints (2.42 Æ 0.14) compared with sham-
operated joints (1.38 Æ 0.14). No significant treatment
No significant difference was noted with the cartilage
effects were seen for any of the gross pathologic
GAG content or GAG synthesis with respect to induc-
Histologic ExaminationsSynovial Membrane H&E
There was a significant ( p ¼ 0.0061) increase in the
The current study used a model of OA that effectively
cumulative pathology score for the synovial membrane
induced significant clinical, gross, histologic, and bio-
in OA-affected (5.17 Æ 0.45) when compared to sham-
chemical changes indicative of OA. The authors believe
operated (3.25 Æ 0.45) joints. No significant treatment
this is the first controlled study to assess clinical
musculoskeletal pain following the treatment of OAwith MSCs. While all of the clinical parameters were
significantly increased following the induction of OA,
Cartilage stained with H&E showed a significant
improvements were not demonstrated with ADSVF or
( p < 0.0131) increase in the modified Mankin score
BMDMSC treatment. This is in contrast to anecdotal
(cumulative score of all four outcome parameters) when
reports presented by Vet StemTM following the clinical
OA-affected (3.43 Æ 0.53) were compared with sham-
use of ADSVF (R Harman et al., 2007, personal
operated (1.63 Æ 0.53) joints based on location. No
communication, http://www.vet-stem.com). The authors
significant treatment effects were observed based on
assume the uncontrolled nature of case selection,
the total modified Mankin score or individual outcome
variability in clinical disease progression, as well as
lack of treatment uniformity in the Vet-StemTM cases
MESENCHYMAL STEM CELLS FOR OSTEOARTHRITIS
are most likely responsible for the disparity. In fact,
previous failure of medical treatment, as well as a poor
more improvement in range of motion (measured by
prognosis following diagnostic arthroscopy.7
joint flexion) was gained with placebo treatment than
A secondary goal of the current study was to compare
with either ADSVF or BMDMSC, with the least
treatment effects of ADSVF and BMDMSC. Because only
significant response being seen in the ADSVF-treated
significant improvement in synovial PGE2 concentra-
horses. It is difficult to explain these findings, given that
tions could be demonstrated with BMDMSC, this
other outcome parameters that typically accompany
comparison is somewhat limited; finding a greater
change in joint flexion (significant change in synovial
magnitude of an effect with bone marrow- versus
membrane pathology and radiographic pathology at
adipose-derived cells has also been seen with multiple
joint capsule margin) were not seen in this study.
other studies involving musculoskeletal tissues and is,
Induction of OA significantly increased synovial
fluid PGE2 concentrations. This finding would be
In summary, no adverse effects were noted with
expected with joint disease as a marker of inflamma-
tion5,18 and can be driven by a host of proinflammatory
ADSVF was associated with increased synovial fluid
cytokines. While a decrease in synovial fluid PGE2
TNF-a concentration, which is worrisome. The only
was seen with ADSVF treatment, this difference was
significant beneficial effect was noted in synovial PGE2
not statistically significant. Conversely, treatment with
level reduction following BMDMSC treatment. Overall,
BMDMSC not only significantly decreased synovial fluid
this modest improvement based on the number of other
PGE2 levels in the OA-affected limb, but also showed a
outcome parameters dampens the enthusiasm of the
systemic effect through significantly decreasing the
authors’ use of unmodified MSC in the treatment of OA.
PGE2 concentration in the sham-operated limb as well.
Further modification using gene therapy or selection of
The reduction of PGE2 represents a decrease in overall
subpopulations of MSC needs to be explored for the
joint inflammation and has historically been positively
correlated with a decrease in pain,18–21 although nosignificant reduction in pain was observed as a result
of BMDMSC or ADSVF treatment. Previously in this
Vet-StemTM Poway, CA provided partial funding for this
model, when a significant reduction of PGE2 has been
study. None of the authors’ professional or financial affiliations
noted, a decrease in clinical pain has also been observed
have biased this presentation. The authors thank all of thestaff and volunteers at the Equine Orthopaedic Research
as was the case following IA administration of cortico-
Center at Colorado State University for their help and
steroids.22,23 Treatment using interleukin-1 receptor
antagonist11,24 demonstrated both symptom- and dis-ease-modifying effects without reduction of synovial
PGE2 levels. Thus, PGE2 reduction is not a prerequisite
1. Lawrence R, Helmick C, Arnett F, et al. 1998. Estimates of the
for symptom-modifying effects. While a decrease of TNF-
prevalence of arthritis and selected musculoskeletal disorders
alpha has been shown to occur following peritoneal
in the United States. Arthritis Rheum 41:778–779.
2. Rossdale PD, Hopes R, Digby NJW, et al. 1985. Epidemio-
treatment with allogenic BMDMSC in mice with colla-
logical study of wastage among racehorses 1982 and 1983. Vet
gen-induced arthritis,9 leading to a decrease in inflam-
mation measured through paw size and discoloration,
3. USDA. 2000. Lameness and laminitis in U.S. horses. Fort
TNF-a was not decreased in the current study. In fact,
Collins, CO: USDA:APHIA:VS, CEAH, National Animal
treatment with ADSVF increased synovial fluid TNF-a.
Murphy et al. observed a decrease in progression of
4. McIlwraith CW, Frisbie DD, Kawcak CE, et al. 2009.
OA following treatment with autologous BMDMSC
Recommendation of criteria for the evaluation of macroscopicand histological changes occurring in equine osteoarthritis.
and hyaluronic acid using a medial meniscectomy and
Osteoarthritis Cartilage (in press).
anterior cruciate deficient model in the goat.8 This
5. Frisbie DD, Al-Sobayil F, Billinghurst RC, et al. 2008.
study also demonstrated a neomeniscal tissue formation
Changes in synovial fluid and serum biomarkers with exercise
associated with animals showing a decreased OA. Barry
and early osteoarthritis in horses. Osteoarthritis Cartilage
postulated that the increase in stability afforded from the
neomeniscal tissue was most likely responsible for the
6. Frisbie DD. 2005. Future directions in treatment of joint
disease in horses. Vet Clin North Am Equine Pract 21:713–
decreased progression of OA,25 a fact that is supported by
the lack of decreased OA progression in the current OA
7. Frisbie DD, Hague BA, Kisiday JD. 2007. Stem cells as a
model which does not have an instability component. It
treatment for osteoarthritis. Presented at American College
should be noted that the current study did not use the
of Veterinary Surgeons Veterinary Symposium, Chicago, IL
addition of hyaluronic acid with the MSC administration
[available in digital format from the corresponding author].
and, thus, may have decreased the resident time of the
8. Murphy JM, Fink DJ, Hunziker EB, et al. 2003. Stem cell
cells in the joint space. It is of interest to the authors that
therapy in a caprine model of osteoarthritis. Arthritis Rheum48:3464–3474.
a short-term follow-up (6–18 months) on equine patients
9. Augello A, Tasso R, Negrini SM, et al. 2007. Cell therapy using
suffering from meniscal disease, and treated with
allogeneic bone marrow mesenchymal stem cells prevents
BMDMSC plus hyaluronic acid, did show a better than
tissue damage in collagen-induced arthritis. Arthritis Rheum
expected return to full athletic work (67%) following
10. Black LL, Gaynor J, Gahring D, et al. 2007. Effect of adipose-
20. May SA, Hooke RE, Lees P. 1991. Adverse conditions in vitro
derived mesenchymal stem and regenerative cells on lame-
stimulate chondrocytes to produce prostaglandin E2 and
ness in dogs with chronic osteoarthritis of the coxofemoral
stomelysin. Equine Vet J 23:380–382.
joints: a randomized, double-blinded, multicenter, controlled
21. May SA, Hooke RE, Lees P. 1992. Inhibition of interleukin-1
activity by equine synovial fluid. Equine Vet J 24:99–102.
11. Frisbie DD, Ghivizzani SC, Robbins PD, et al. 2002. Treat-
22. Frisbie DD, Kawcak CE, Trotter GW, et al. 1998. The effects
ment of experimental equine osteoarthritis by in vivo delivery
of 6-alpha methylprednisolone acetate on an in vivo equine
of the equine interleukin-1 receptor antagonist gene. Gene
osteochondral fragment exercise model. Am J Vet Res 12:
12. Kisiday JD, Kopesky PW, Evans CH, et al. 2008. Evaluation of
23. Frisbie DD, Kawcak CE, Trotter GW, et al. 1997. The effects of
adult equine bone marrow- and adipose-derived progenitor
triamcinolone acetate on an in vivo equine osteochondral
cell chondrogenesis in hydrogel cultures. J Orthop Res 26:
fragment exercise model. Equine Vet J 29:349–359.
24. Frisbie DD, Kawcak CE, Werpy NM, et al. 2007. Clinical,
13. Anonymous. 1991. Definition and classification of lameness.
biochemical and histologic effects of intra-articular admin-
In: Guide for veterinary service and judging of equestrian
istration of autologous conditioned serum in horses with
experimentally induced osteoarthritis. Am J Vet Res 68:290–296.
14. Farndale RW, Buttle DJ, Barrett AJ. 1986. Improved
25. Barry FP. 2003. Mesenchymal stem cell therapy in joint
quantitation and discrimination of sulphated glycosaminogly-
disease. Novartis Found Symp 249:86–96; discussion –102,
cans by use of dimethylmethylene blue. Biochem Biophys Acta
26. Im GI, Shin YW, Lee KB. 2005. Do adipose tissue-derived
15. Vick MM, Adams AA, Murphy BA, et al. 2007. Relationships
mesenchymal stem cells have the same osteogenic and
among inflammatory cytokines, obesity, and insulin sensitiv-
chondrogenic potential as bone marrow-derived cells? Osteo-
ity in the horse J Anim Sci. 85:1144–1155.
16. McFarlane D, Holbrook TC. 2008. Cytokine dysregulation
27. Hennig T, Lorenz H, Thiel A, et al. 2007. Reduced chondro-
in aged horses and horses with pituitary pars intermedia
genic potential of adipose tissue derived stromal cells
dysfunction. J Vet Intern Med 22:436–442.
correlates with an altered TGFbeta receptor and BMP profile
17. Anonymous. 2006. The GLIMMIX Procedure. Cary, NC: SAS
and is overcome by BMP-6. J Cell Physiol 211:682–691.
28. Liu TM, Martina M, Hutmacher DW, et al. 2007. Identifica-
18. May SA, Hooke RE. 1987. The identity of the E-series
tion of common pathways mediating differentiation of bone
prostaglandins produced by chondrocytes and synovial cells
marrow- and adipose tissue-derived human mesenchymal
in response to a variety of stimuli. Proc Br Equine Vet Assoc
stem cells into three mesenchymal lineages. Stem Cells 25:
19. May SA, Hooke RE, Lees P. 1989. Identity of the E-series
29. Noel D, Caton D, Roche S, et al. 2008. Cell specific differences
prostaglandin produced by equine chondrocytes and synovial
between human adipose-derived and mesenchymal-stromal
cells in response to a variety of stimuli. Res Vet Sci 46:
cells despite similar differentiation potentials. Exp Cell Res
Renesas Releases 36 New Flash Microcontrollers: the SH7216 Group 32-bit On- Chip Flash Memory Microcontrollers for Industrial Applications Featuring 200 MHz Operation and an Extensive Set of Communications and Other Peripheral Functions ⎯ Operating speed increased 1.25 times and processing capabilities increased up to 1.5 times over earlier Renesas products. Furthermore, these de
G u i d e l i n e s for the use of q u i n o l o n e s in veterinary medicine Prudent therapeutic use of quinolones in food-producing animals Bayer`s position: Expertise with responsibility As one of the world's leading research-based chemical and pharmaceutical companies, Bayer's first concern is to ensure that its products offer the highest possibl
 MESENCHYMAL STEM CELLS FOR OSTEOARTHRITIS
by a significantly ( p < 0.0001) higher cumulative radio-graphic score in the OA-affected (1.19 Æ 0.12) comparedto the sham-operated (0.06 Æ 0.12) joints. No significanttreatment effects were detectable.
MESENCHYMAL STEM CELLS FOR OSTEOARTHRITIS
by a significantly ( p < 0.0001) higher cumulative radio-graphic score in the OA-affected (1.19 Æ 0.12) comparedto the sham-operated (0.06 Æ 0.12) joints. No significanttreatment effects were detectable.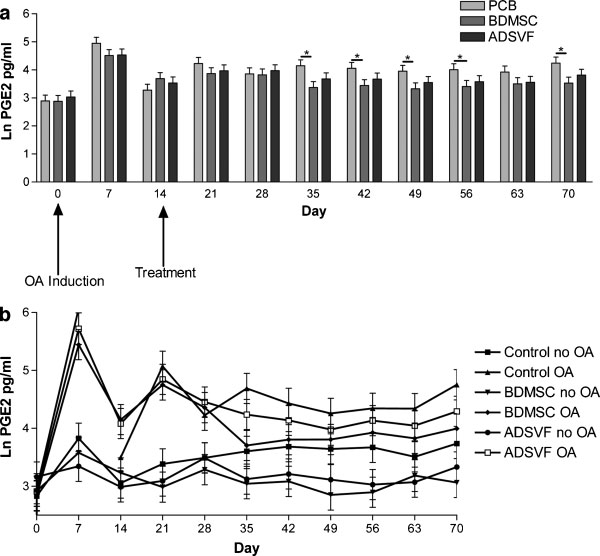 concentration plotted by Day for eachtreatment group (average of boththe osteoarthritis-affected and Shamjoints). An asterisk represents asignificant difference between thecomparison. (b) Natural log of PGE2concentration plotted by Day for eachtreatment group (for both the osteo-arthritis-affected and Sham joints).
concentration plotted by Day for eachtreatment group (average of boththe osteoarthritis-affected and Shamjoints). An asterisk represents asignificant difference between thecomparison. (b) Natural log of PGE2concentration plotted by Day for eachtreatment group (for both the osteo-arthritis-affected and Sham joints).